

Abstract
This is a case of a 33-year-old male complaining of severe headache, neck pain, photophobia, vomiting and high-grade fever of several days. He had history of nasal polyp removal and recurrent sinusitis in the last 8 years. On examination: conscious with glasco coma scale (GCS) 15/15 and normal limbs strength but with positive Babinski sign. For further observation, he was admitted and full work-up was done. Even though full empirical antibiotics were started, there was no immediate improvement and he deteriorated dramatically developing ocular deficit, hydrocephalus and lower level of consciousness with multiple infarctions found at different areas in brain. After that point, a decompressive craniectomy was done, and multiple antibiotics and antifungal medications were prescribed. However, he deteriorated to GCS 3/15; cardiopulmonary resuscitations were not successful, as he demised next day. It shall be noted that aspergillosis can lead to difficult complications, so diagnosis and treatments should not be delayed.
Fungal infections of the paranasal sinuses are uncommon and usually occur in individuals who are immunocompromised. However, recently, the occurrence of fungal sinusitis has increased in the immunocompetent population. This case report is for young man who is none-smoker and none-alcoholic immunocompetent patient who complained of severe headache and neck pain of several days; he was exposed to a highly invasive aspergillus fungal infection that showed drastic invasive complications even with aggressive medical and surgical interventions.
Case Report
Patient information
A 33-year-old patient with a history of nasal polyp removal and recurrent sinusitis in the last 8 years, presented to the emergency department complaining of severe headache, neck pain, photophobia, vomiting and high-grade fever but with no sore throat, dysuria, diarrhea, cough or convulsions.
Clinical findings
Patient was conscious oriented, glasco coma scale (GCS) 15\15, pupils: equal bilateral, no focal neurologic deficit, positive Babinski sign, as seen in Table 1.
Relevant past medical history and interventions for a 33 years old male with a past medical history of nasal polyp removal and recurrent sinusitis in the last 8 years.
Diagnostic assessment
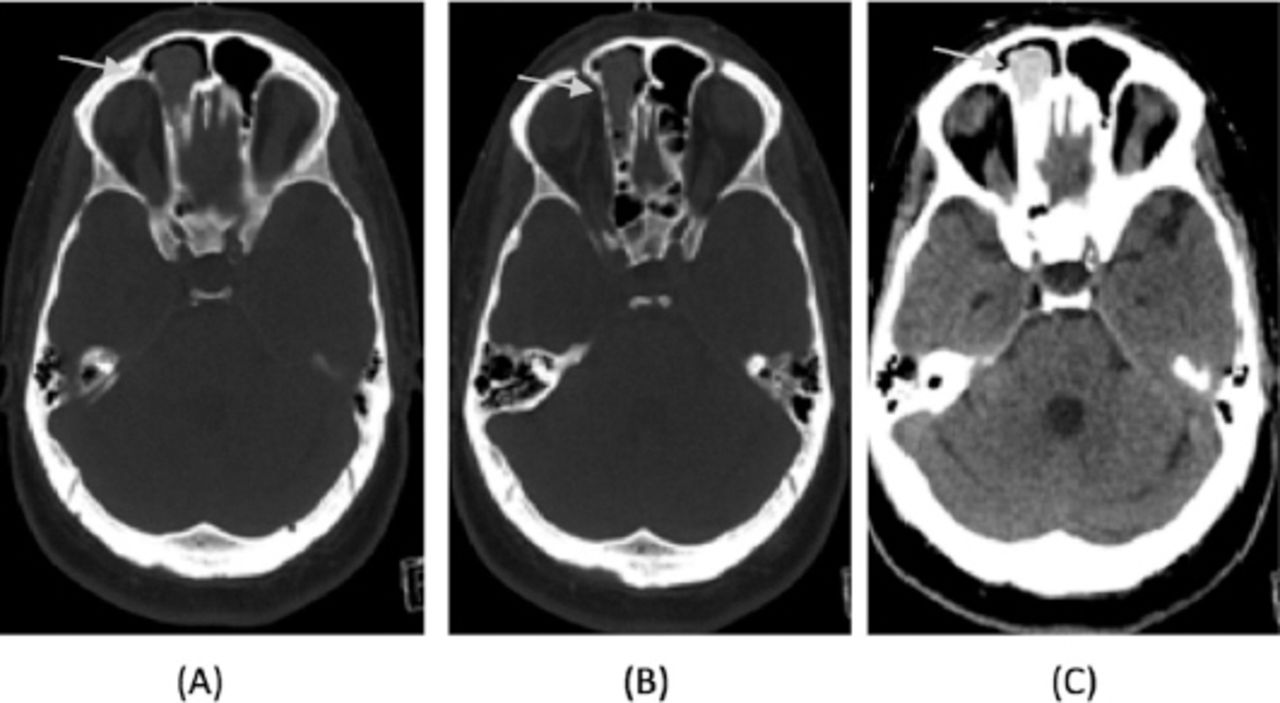
The CT brain showed: frontal sinus muocele and sinusitis (Figure 1). CT scan of the brain with contrast showed sphenoid sinuses with bone resorption and right frontal mucocele. He was started on intravenous ceftriaxone, acyclovir, vancomycin and paracetamol. Multiple investigations were carried out including lumbar puncture, HIV screening, P-ANCA, C-ANCA and ANA were all negative. The CSF was sent for bacterial culture but AFB culture was negative. Patient diagnosis was invasive fungal sinusitis as bacterial sinusitis can rarely cause bone resorption in immunocompetent patient.

CT brain A-C) There is a well defined oval shaped at the right frontal sinus as seen in arrows (B) ethmoidal air cells suggestive of a mucocele.
Symptoms were persistent even with empirical antibiotics therapy, and then he was started on anti-tuberculous medication for suspicion of tuberculous meningitis, as patient received antibiotics for 3 days with no improvement and follow up CSF results showed increased in cell counts with lymphocytes predominance. Cerebrospinal fluid results analysis is as follows: white blood cells=336 (normal from=0-5), red blood cells=804 (normal from=0-5), lymphocyte= 80%, and neutrophil=20%.
Therapeutic interventions
The ENT consultation was done carried out and advised to add empirical antifungal medication. Intravenous amphotericin was added to medication and patient was still on persistent symptoms, and underwent for turbinectomy, septoplasty and sampling from the mass lesion and sent to histopathology. The next plan was to let the patient see a neurosurgeon and take a sample of sphenoid and frontal lesions that invaded the skull bone to excluded tumor or fungal infection.
Follow up and outcomes
His symptoms were progressing and developed severe headache, dizziness blurred of vision with RT 3rd nerve palsy that indicated increased intracranial pressure and ptosis. Urgent CT brain showed hydrocephalous, which necessitated quick external ventricular drain to release intracerebral pressure.
He then had decreased level of consciousness, then intubated and shifted to ICU. The CT scan of the brain was carried out done and showed external ventricular drain on place with multiple infarctions in cerebellum, cerebrum and brain stem.
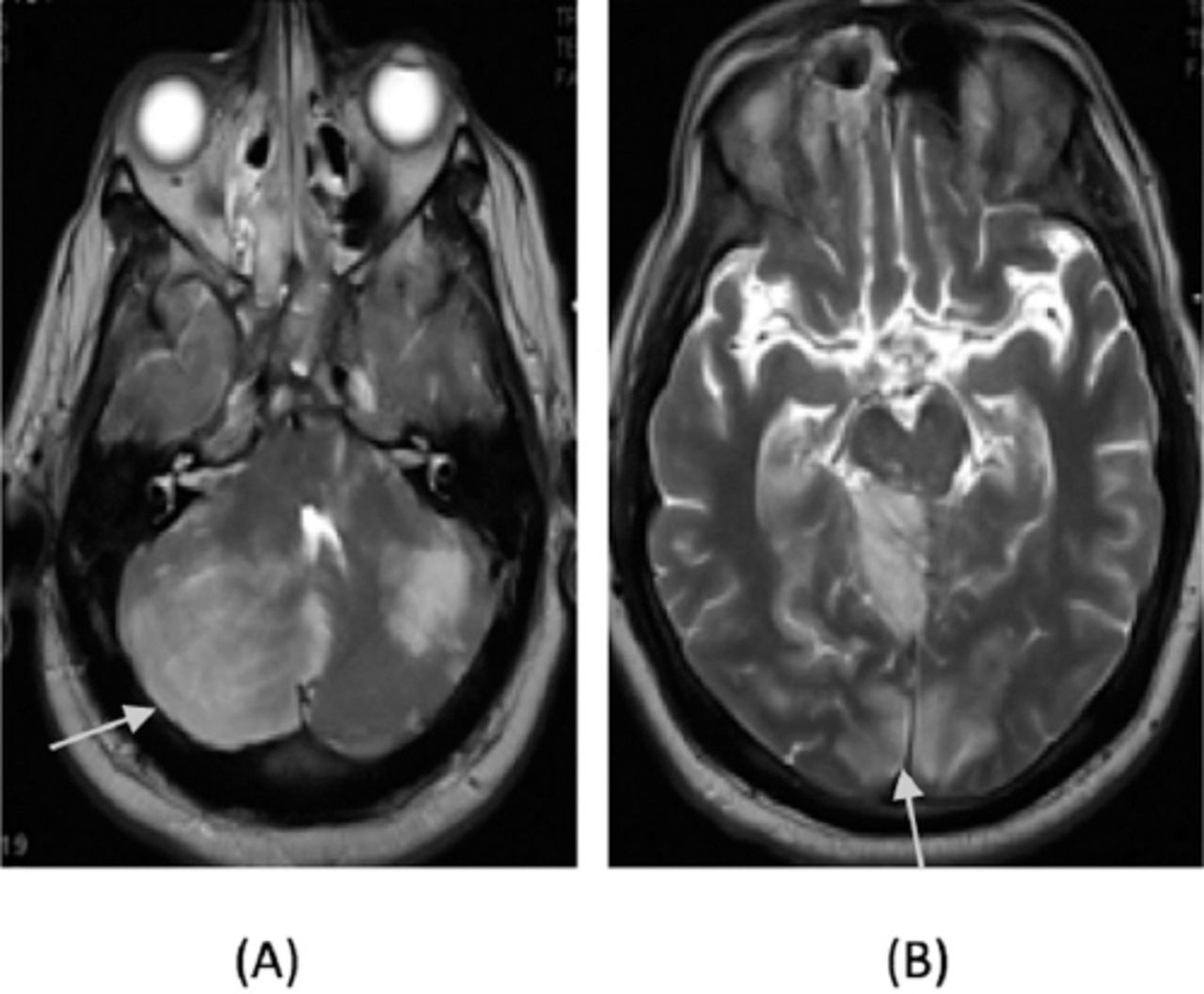
MRI Brain was also carried out and showed acute arterial infarction with restricted diffusion involving the right bilateral cerebellar hemisphere more than the left bilateral cerebellar hemispheres, cerebellar vermis and tonsil, bilateral occipital cortex, bilateral thalami and both hippocampus with posterior circulation territory infarcts, few scattered acute infarcts in midbrain, left middle cerebellar peduncle, left posterior temporal lobe, there was compression of right posterolateral aspect of medulla and midbrain. Cerebellar tonsil herniation seen in upper cervical canal, EVD in place with no hydrocephalous, bilateral ethmoid sinusitis, right frontal and maxillary opacification and complete sphenoid sinus opacification with clival and floor of Sella destruction Brain taken show no sinus thrombosis, as on Figure 2.

MRI brain A) Acute arterial infarction of bilateral cerebellar hemispheres (RT>>LT), cerebellar vermis, B) bilateral occipital cortex, bilateral thalami and both hippocampi midbrain as seen in arrows.
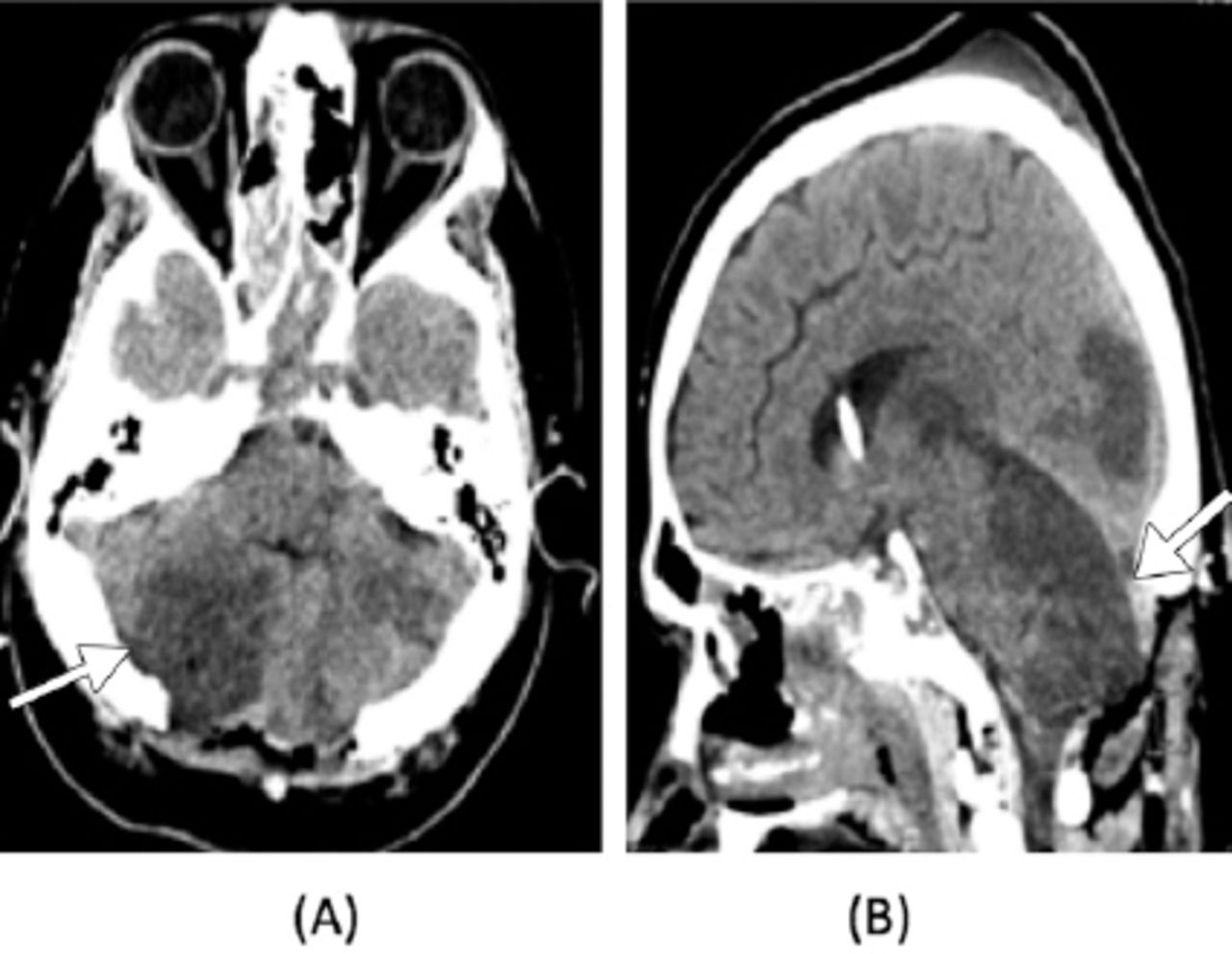
The MRI brain with contrast was carried out showed heterogeneous enhancement noted within sphenoid sinus mass lesion extending into right posterior ethmoid, no retro clival extension, for further evaluation with histopathology. Mass effect with tonsillar herniation. Emergency posterior fossa decompressive craniectomy with cerebellar extension duroplasty were carried out (Figure 3), then returned to ICU, patient was kept intubated on mechanical ventilator with GCS 4-5\15.

{kind=link}
{kind=link}
{kind=link}
CT brain A-B) increase cerebellar and occipital lobes hypo densities as seen in arrows, post posterior fossa decompression and extra-ventricular drain insertion
Biopsy result showed right and left sphenoid sinus; invasive fungal sinusitis (given the presence of septae and acute angling of the PAS + fungal hyphae, Aspergillosis species is favored. Cytology report was negative for malignant cells.
Trails of weaning from mechanical ventilator carried out but no improved GCS. Later, he developed pulseless electrical activity, then cardiac arrest and he revived after one CPR cycle. Unfortunately, he demised next day.
Discussion
Invasive fungal sinusitis includes the acute fulminant type, which has a high mortality rate if not recognized early and treated aggressively and the chronic and granulomatous types. Saprophytic fungi of the order Mucorales, including Rhizopus, Rhizomucor, Absidia, Mucor, Cunninghamella, Mortierella, Saksenaea, and Apophysomyces species, cause acute invasive fungal sinusitis.
It is found that invasive cerebral aspergillosis is a complicated and quick progressive disease that cause high mortality rate up to hundred percent even with effective management.1 Aspergillus species can invade cerebral vessels leading to different pathologies including infarction or hemorrhage leading to progressive inflammation.
Acute invasive fungal sinusitis results from a rapid spread of fungi through vascular invasion into the orbit and CNS. It is common in patients with diabetes and in patients who are immunocompromised and has been reported in immunocompetent individuals.6 Typically, patients with acute invasive sinusitis are severely ill with fever, cough, nasal discharge, headache and mental status changes. They usually require hospitalization. Initiate emergency treatment once this condition is suspected. This rapidly progressive disease that invades adjacent structures, causing tissue damage and necrosis; Cavernous sinus thrombosis and invasion of the CNS are common and carry a high mortality rate.
Invasive aspergillus sinusitis of this patient showed invasive complications that rarely happened in other populations based on previous researches of meningitis as seen on time line Table 1, orbital involvement, skull base erosion with intracranial extension, and infratemporal fossa extension multiple vasculitis with diffuse brain edema and hydrocephalous.1,2 The likely pathogenesis of cerebral infarction is by direct angioinvasion and less likely compression by oedema.
Although diagnosis of this disease is not easy, clinical suspension is highly required with quick medical and neurosurgical interventions. Surgical interventions that he exposed to included external ventricular drain for hydrocephalous, posterior fossa decompression and turbinectomy, septoplasty for the sinuses.
According to other researches, chronic invasive sinonasal aspergillosis has been documented in immunocompetent patients living in dry-air climates similar to desert Sahara and Middle Eastern countries.1,5 Prognosis of acute invasive fungal sinusitis is often misleading, it carries a poor prognosis. Mortality rate is reported at 50%, even with aggressive surgical and medical treatment,3,4 Relapses are common during subsequent episodes of neutropenia. Treatments with systemic antifungals as prophylaxis are indicated in cases of neutropenia.
In conclusion, Aspergillosis infection usually misdiagnosed especially with immunocompetent patients that can lead to difficult complications, so diagnosis and treatments should not be delayed. However, quick invasion of this invasive infection is fatal even with proper medical and surgical interventions.
Footnotes
Disclosure. The authors declare no conflicting interests, support or funding from any drug company.
- Received August 8, 2017.
- Accepted December 6, 2017.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.