


Clinical Presentation
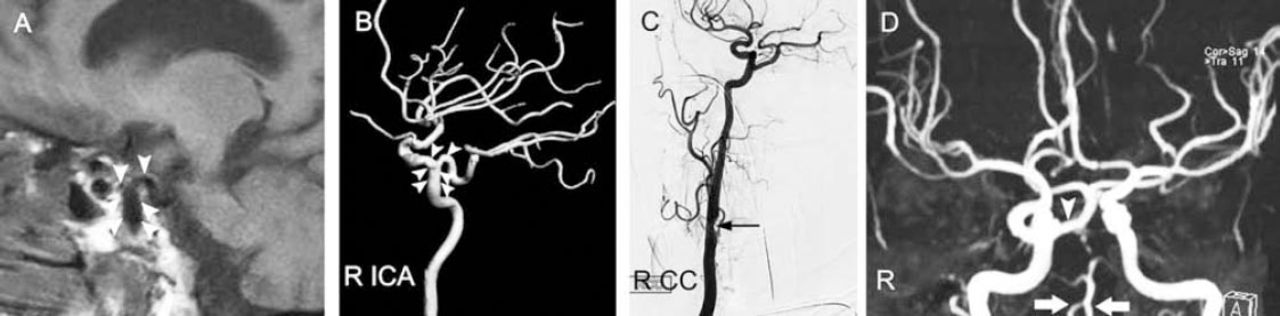
A 61-year-old woman underwent MRI scan of brain (Figure 1A), followed by conventional angiography (Figures 1B & 1C) and magnetic resonance cerebral angiography (Figure 1D, conventional angiography was performed for more specific details regarding the findings of the initial MR cerebral angiography) as part of the ischemic stroke work-up for recurrent episodes of right hemiparesis and expressive aphasia.
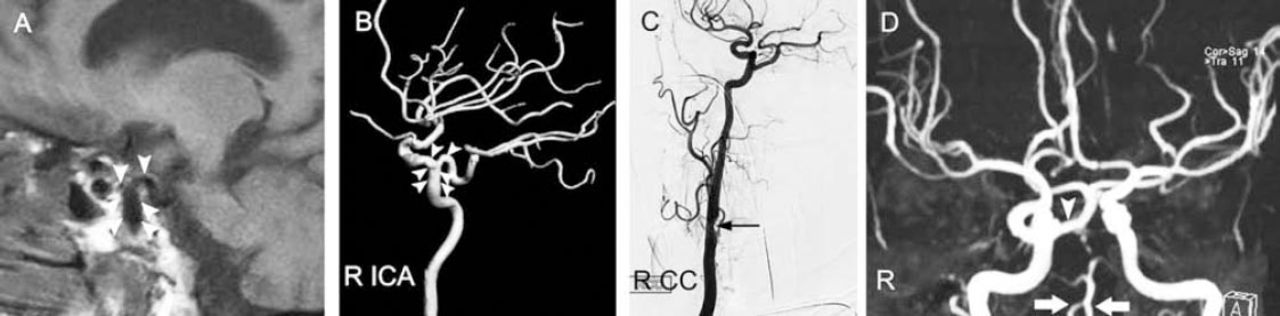
Patient’s MRI depicting sagittal view of T1 weighted image A), digital subtraction angiography B & C), and magnetic resonance angiography D). RICA- right internal carotid, RCC-right common carotid
Questions
Interpret the angiographic findings.
Answer
Parasagittal T1 weighted cranial MRI (Figure 1A) shows the configuration of flow voids (arrowheads) in the presellar segment of the right internal carotid artery (ICA) resembling the Greek letter t (spelled tau). This appearance is more obvious in the right carotid angiogram provided (Figure 1B). The vertical limb of t (arrowheads) is formed by the upwardly coursing proximal cavernous segment of ICA, while the posteriorly directed persistent trigeminal artery and the horizontally coursing intracavernous ICA segment constitutes the other arm. Indeed, the presence of this ‘tau sign’ in the sagittal T1 weighted MRI brain (appearing as vascular flow void) or cavernous ICA angiogram aids in the identification of persistent trigeminal artery, a rare embryogenic connection between the carotid and vertebro-basilar arterial systems. The right common carotid (R CC) angiography (lateral view, Figure 1C) shows the absent posterior communicating artery and asymptomatic 60% stenosis (thin arrow) of cervical internal carotid segment. Circle of Willis MR angiography (Figure 1D) shows the persistent trigeminal artery (arrowhead) continuing as the basilar artery. The vertebral arterial system is shown by thick arrows (Figure 1D). The proximal basilar artery (usually constituted by bilateral vertebral arteries) is vastly missing in this MR angiography (and in the conventional angiography), and the persistent trigeminal artery constitutes the main trunk of basilar artery.
Discussion
Imaging of vascular system (pipes) supplying the brain (parenchyma) constitutes an essential diagnostic work-up in the evaluation of stroke patients for identifying the culprit vascular lesion(s)/mechanism underlying the stroke, compensatory vascular changes or collateral flow, status of the circle of Willis, presence (or absence) of incidental vascular anomaly such as aneurysm or arterio-venous malformation (that may have clinical relevance for the recent or future vascular events), and variation(s) in the vascular anatomy (that may have therapeutic implications).1,2 Furthermore, vascular imaging with a CT, MRI, or conventional digital subtraction angiography is required for quantifying the arterial stenosis in the pre-surgical assessment for revascularization procedure such as carotid endarterectomy or angioplasty (that is indicated as an appropriate preventive strategy in the setting of a high grade symptomatic carotid stenosis underlying a single or recurrent stroke or transient ischemic attack[s]).1,2 The cerebral angiogram depicted here presents remarkable variations in the vascular anatomy.
Persistent trigeminal artery, the unusual arterial anastomotic channel between the carotid and vertebra-basilar system, has a reported angiographic incidence of 0.1 to 1%.3 The persistent trigeminal artery usually involutes at week 5 of embryonic development.3 In this adult, the persistent trigeminal artery continues as the basilar artery (Figures 1C & 1D), and the posterior communication artery (Figure 1C) is conspicuously absent (the disconnection). This pattern in which the persistent trigeminal artery constitutes the distal basilar artery with the superior cerebellar and posterior cerebellar arteries originating from the basilar artery, while the ipsilateral posterior communicating artery (the usual arterial connection between the distal ICA and posterior cerebral artery) is typically absent is termed Saltzman type 1 persistent trigeminal artery.3 The proximal basilar artery is usually hypoplastic or vastly missing in this setting (Figure 1D) and the posterior inferior cerebellar artery and the anterior inferior cerebellar arteries (not shown here) arise from the vertebral arterial system. In Saltzman type II, while the persistent trigeminal artery supplies the basilar artery, the posterior cerebral arteries originate from the distal carotid artery through posterior communicating arteries and not from the basilar artery.3
Persistent trigeminal artery, the unusual arterial connection, is an incidental finding in this patient and the vastly missing proximal basilar artery constitutes the unusual disconnection. Conventional angiography was performed to confirm the presence or absence of a significant stenosis in the carotid-middle cerebral arterial system on the left (symptomatic) side, and to evaluate for associated aneurysm or vascular malformation. While there was no significant narrowing of the left carotid/middle cerebral artery or associated vascular anomalies in the intracranial circulation, there was a 60% narrowing of the right cervical internal carotid artery at its origin (Figure 1C). Close clinical follow-up with serial imaging of the asymptomatic carotid stenosis was planned in this case (considering the benefit versus risk of a carotid revascularization procedure of asymptomatic carotid stenosis in a female subject), as the right carotid artery was the major provider of blood supplied to the anterior and posterior circulation.
Footnotes
Notice: Authors are encouraged to submit clinical images for possible publication in the Journal. These may be in any field of Clinical Neurosciences, and should approximately follow the format used here. Please address any submissions to the Assistant Editor, Neurosciences Journal, Prince Sultan Military Medical City, PO Box 7897, Riyadh 11159, Kingdom of Saudi Arabia. E-mail: sdouglas{at}psmmc.med.sa
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.