


Abstract
Objectives: To assess the burden and describe the pattern of neurological disorders requiring admissions in a teaching hospital of Al Khobar.
Methods: This is a retrospective, cross sectional study, carried out in the Neurology Department of King Fahd Hospital of the University from January 2009 to December 2016. Neurological disorders were grouped as ischemic stroke, intracerebral hemorrhage, transient ischemic attack, cerebral venous sinus thrombosis, seizure disorders, central nervous system infection, multiple sclerosis, neuropathies, myopathies, headache, dementia and miscellaneous group. Data was entered and analyzed by Statistical Package for the Social Science (SPSS) version 22.0 (IBM Corp., Armonk, NY, USA).
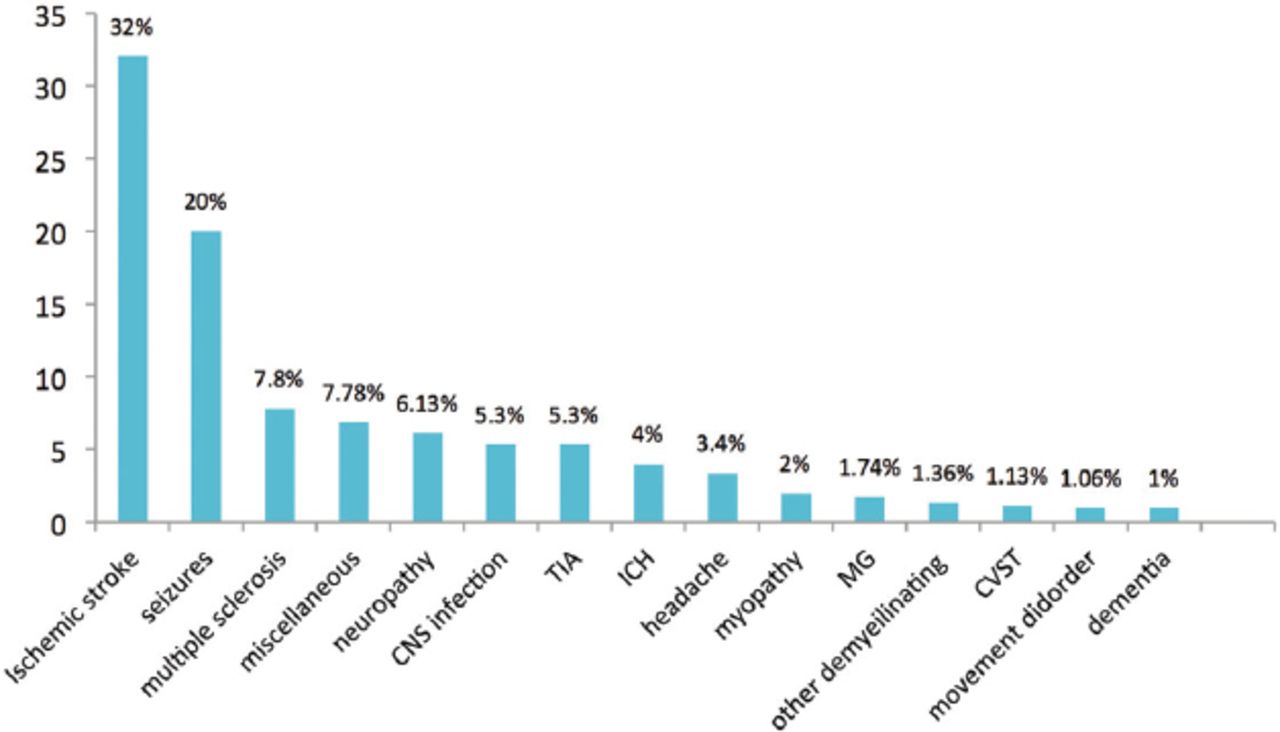
Results: The records of 1,317 patients admitted under Neurology Service were analyzed. Out of that, 740 (56.2%) were male and 577 (43.8%) were female. Mean age was 46.9±24 years (mean±standard deviation). Ischemic stroke was the most common diagnosis (32%) followed by seizures (20%). Multiple sclerosis accounted for around 8% and central nervous system infections 5% of neurological admission.
Conclusion: Ischemic stroke was found to be the most common etiology for hospitalization in our study. The results of our study are similar to previous literature. An urgent need to control major risk factors such as diabetes and hypertension is warranted to minimize the burden of stroke.
Neurological disorders (ND) represent a major burden of disease globally, and the spectrum ranges from non-communicable disorders such as cerebrovascular disease and neurodegenerative disorders to central nervous system (CNS) infections. The pattern of neurological admissions varies amongst different regions of the world, and depends on many factors, including the regional burden of disease. The spectrum of medical diseases in developing countries is different from that of developed countries due to multiple reasons.1 In a recent study, death was recorded in 19% of adults hospitalized with ND and disability in 53.6% of the survivors.2 In a one year retrospective survey from tropical African hospital, ND constituted 24.2% of all medical conditions and stroke accounted for 42.1% of all cases.3
A study from Nigeria found stroke and CNS infections as the most prevalent ND.4 One more study from Nigeria describing the profile of neurological admissions also found stroke and CNS infections as the most common reasons for admission.5 A retrospective study from tertiary care center in Ghana concluded that almost one in 3 patients admitted with ND died and most of them were attributed to non-communicable disorders.6
One study from Saudi Arabia (SA) focusing on common diseases in hospitalized patients found cardiovascular system as the most commonly affected system (19.9%) followed by respiratory (14.5%). Cerebrovascular disease was found in only 2.0% of patients in this study.7
The global burden of ND is approximately 20%, the majority being in the developing countries and still a significant portion is managed by non-neurologist physicians.8 In a community based survey from the Eastern province of SA, the reported crude prevalence of ND was 131/1000 population.9 Despite the fact that ND are projected to escalate worldwide in the coming decades; there is a paucity of published data on the burden, spectrum and outcomes of neurological admissions. There is a need to carry out research work in this field to know about the pattern of ND in hospitalized patients of SA, so more specialized centers can be established to deal with the diseases accordingly.
Methods
This is a retrospective, observational study, carried out in the Neurology Department of King Fahd Hospital of the University (KFHU). The KFHU is a 500-bedded tertiary care teaching and referral hospital. It has an established neurology team of residents, specialist and consultants providing round the clock service. Patients are admitted either through emergency or out-patient departments. The major source of admission is the Emergency Department. The department of neurology has separate specialty clinics for epilepsy, stroke, multiple sclerosis, dementia and neuromuscular disorders along with general neurology. These clinics are headed by consultants specialized in these fields. Acute ischemic stroke (IS) treatments as thrombolysis and neurovascular intervention are also provided at the center by a neurovascular team. A review of medical records of the patients admitted to KFHU over a period of 8 years (from January 2009 to December 2016) was performed after retrieving the data through the electronic data bank system. The study was approved by the institutional ethical committee. The records are maintained according to ICD-9 coding system in the electronic database system of the hospital. The medical records of all patients admitted under neurology service over the study period were reviewed. Patients found to have diseases requiring neurosurgery services care as cerebral neoplasms, compressive myelopathy, and subarachnoid hemorrhage were excluded from the current study. A structured form was used to collect the required information including demographic data as age, gender and nationality. Neurological disorders were grouped as IS, intracerebral hemorrhage (ICH), transient ischemic attack (TIA), cerebral venous sinus thrombosis (CVST), seizure disorders, CNS infection, multiple sclerosis (MS), neuropathies such as Guillian Barre´ Syndrome (GBS), chronic inflammatory demyelinating polyneuropathy (CIDP), diabetic and nutritional neuropathies, myopathies, headache, dementia, demyelinating diseases other than multiple sclerosis and miscellaneous group. Less common diseases such as motor neuron disease, radiculopathy, nonspecific encephalopathies and undiagnosed cases were included in miscellaneous group. Ischemic stroke, TIA, ICH and CVST were altogether considered as cerebrovascular disorders (CVD). Demographic characteristics as age, gender and nationality were recorded. Associated comorbidities such as hypertension, diabetes mellitus and ischemic heart disease were also recorded.
Relevant descriptive statistics, frequency and percentage were computed for neurological diagnoses and associated co morbidities such as diabetes mellitus, hypertension and ischemic heart disease. Data was expressed as mean ±standard deviation (SD) for age and length of stay. Data was entered and analyzed by Statistical Package for the Social Science (SPSS) version 22.0 (IBM Corp., Armonk, NY, USA). At 95% CI, p-value <0.05 was considered significant.
Results
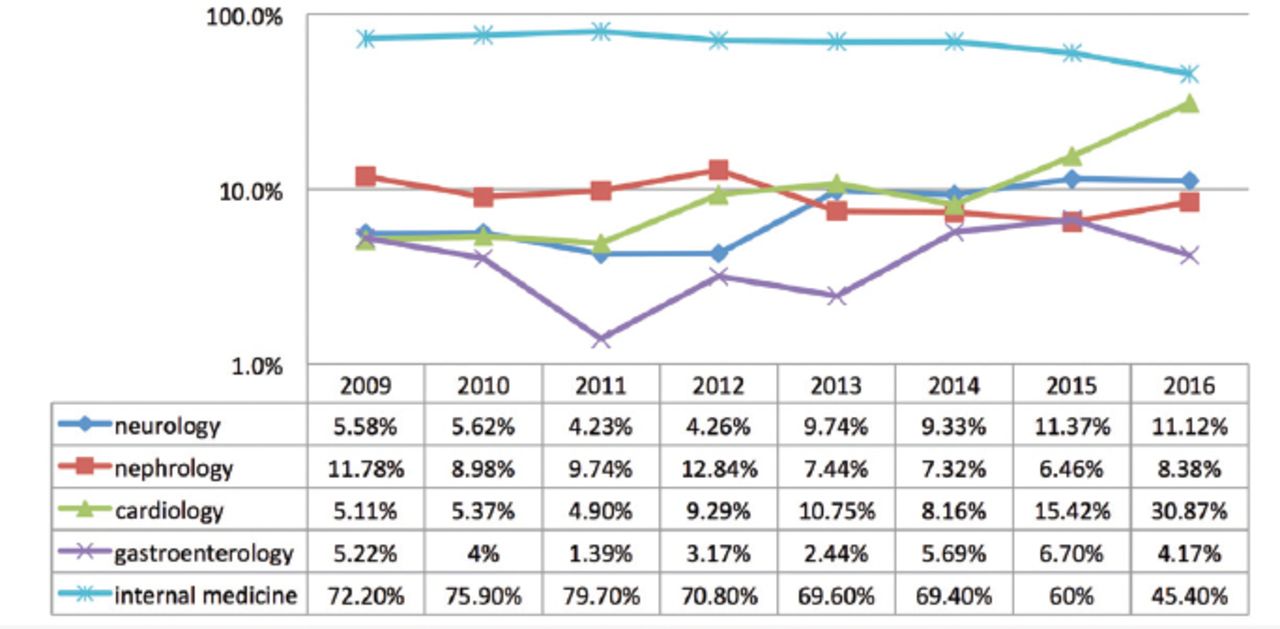
A total of 89,573 patients were admitted in the hospital over the study period. A total of 1,317 (1.47%) patients were admitted under neurology department compared with 10,849 (12.11%) admitted under internal medicine. Neurology contributed to 8.07% of total patients admitted under medicine and all major subspecialties (neurology, cardiology, nephrology and gastroenterology) altogether. Summary of total admissions along with number and percentages of admission under internal medicine and other major subspecialties are described in Table 1. Percentage wise distribution of patients under different specialties in relation to medicine is shown in Figure 1. The burden of inpatients services shared by department of neurology and cardiology has increased over the past four years. The records of 1,317 patients admitted under neurology service were included in the study. Males were 740 (56.2%) and females 577 (43.8%) with M:F ratio of 1.2:1. Saudi patients were 996 (75.6%) while non Saudis were 321 (24.4%). Mean age was 46.9±24 years (mean±SD). Mean length of stay was 16.8±52.7 days (mean±SD). Hypertension was the most commonly identified associated comorbidity (44%), followed by diabetes mellitus (35%) and ischemic heart disease (8.8%). Among the ND requiring admission, CVD was the leading cause. Ischemic stroke (IS), TIA, ICH, and CVST included in CVD accounted for 41.6% of all admissions. In CVD group, IS was found in 75.5%, TIA 12.5%, ICH 9.4% and CVST 2.3%. Overall, IS was the most common reason for admission followed by seizure disorder, multiple sclerosis, neuropathies and CNS infections in decreasing frequency. Guillian Barre´ Syndrome was the reason for admission in 2.35% and CIDP 2%. Details are summarized in Figure 2. Death was observed in 86 (6.5%) patients during hospital stay. As it was a retrospective study, it was difficult to verify the exact cause of mortality. Demographic characteristics of major ND as mean age±SD, gender distribution and associated comorbidities are shown in Table 2.
Total admissions in hospital along with number and percentages of admission under neurology and other medicine services.
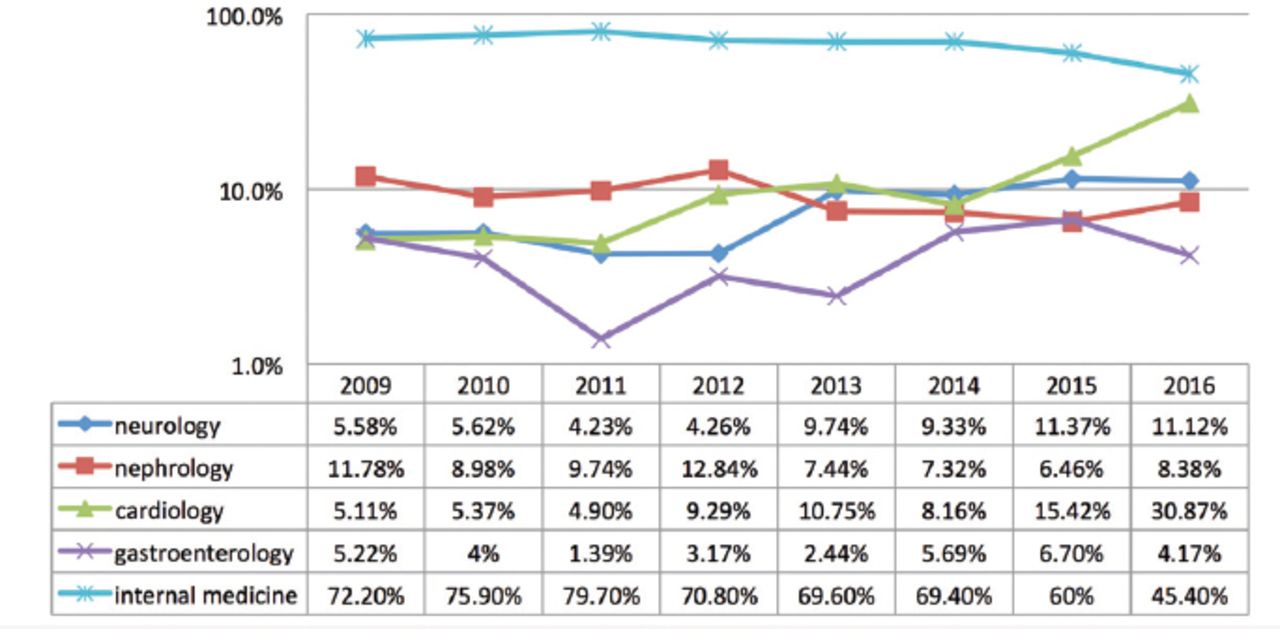
Yearly percentage distribution of patients under different specialties in relation to medicine

Neurological disorders identified in patients admitted under neurology
Demographic characteristics of major neurological disorders.
Discussion
Majority of the patients presented after the age of 40 years with mean age of 46.9±24 years. This is similar to a hospital based study from Bangladesh10 but lower compared with studies from Nigeria.11,12 No significant difference in gender distribution was identified in the study overall. However, there was significant male preponderance in IS, ICH, TIA and CNS infections while females preponderance in MS and CVST. The percentage of inpatients admission under neurology service was 8.07% taking medicine and other major subspecialties altogether. In a study from SA, analyzing 5,594 admitted patients with medical disease according to systemic involvement, CNS involvement was identified in nearly 5 % of cases and cerebrovascular events were ranked tenth among the sixteen most common diagnoses in hospitalized patients.7 The estimated burden of ND in our study was lower compared with other hospital based studies, reporting a burden range of 21-24%.3,11,12 However, an increase in absolute number and percentage of patients with neurological diseases has been observed over the past 4 years. Hypertension was the most commonly associated comorbidity in our cohort. The prevalence of hypertension in KSA is on rising side and affects more than one fourth of adult Saudi population. In a community based study, the reported prevalence was 28.6% for males and 23.9% for females.13 Diabetes mellitus was found in significant number (35.2%) of patients. An approximately 10 fold increase in diabetes has been observed in the past 3 eras in SA.14
Ischemic stroke was the most common reason for hospitalization as identified in other studies describing the pattern of in-patient ND. The percentage in our study was less as compared with hospital based registries from Nigeria as reported by Ekenze et al (64.9%),5 Eze et al (62%)11 and Philip-Ephrahim et al (42.1%),3 but comparable to a report by Gajurel et al (36%) from Nepal.15 Significantly higher prevalence of hypertension (74%) and diabetes mellitus (60%) in these patients is of real concern and emphasizes the need for implementation of adequate preventive measures to control these modifiable risk factors. Seizure was the second most commonly identified diagnosis. Seizure was also identified as the second most common cause of referral to neurologist after stroke by Chowdhury et al,10 and Gajurel et al.15 The reported prevalence rate (6.45/1000) of active epilepsy in Saudi nationals is not different from other developed and developing countries.16 Epilepsy is one of the chronic and common ND having significant physical, social and economic implications on the patients, care givers and health care system. According to a recent study describing the epilepsy services in SA, there is a real shortage of epileptologist and epilepsy monitoring units (EMU), especially in the northern and southern regions of KSA.17 Multiple sclerosis was the leading cause of hospitalization following IS and seizures. The change in epidemiology of MS has been observed worldwide. Although, the Arabian Gulf Region is located in a low risk zone, an increase in the incidence has been reported in recent years. Change in life style, relatively increase proportion of younger population, vitamin D deficiency and consanguineous marriages are considered as contributing factors.18 In one study from SA including 806 neurology patients, MS was diagnosed in 16 patients (2.35%).19 The mean age in our study was similar to overall estimated age of 28.5 years described in a literature survey on MS epidemiology in the Middle East and North African countries.20 Central Nervous System infections were less frequent than reported by Ekenze et al (21.8%).5 The difference could be attributed to better infection preventive measures in KSA. As KSA faces a huge burden of pilgrims annually during Hajj, the Saudi Ministry of Health acts strictly to prevent infections hazards as meningococcal meningitis and other infections by an effective international partnership in the area of infection control and preventive medicines.21 A major limitation of our study is its retrospective nature causing difficulty in ascertaining the diagnosis in a few cases and identifying the reasons for mortality.
Patients with a wide spectrum of ND were admitted during the study period. Cerebrovascular diseases, seizure disorders and multiple sclerosis are the main ND requiring hospitalization. There is a need for further prospective epidemiological studies to estimate the real burden and assess the spectrum of ND in the kingdom. Separate neurovascular services and establishment of stroke center along with rehabilitation center are the real need to optimize the care of patients with stroke, the leading ND.
Acknowledgment
We are thankful to the administration and statistics department of King Fahd Hospital of the University for providing records of admitted patients.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received April 16, 2017.
- Accepted October 4, 2017.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.