


ABSTRACT
Objectives: To assess how facet medial branch radiofrequency thermocoagulation (FMB-RFT) outcomes are affected by severe facet joint osteoarthritis (FJO).
Methods: This retrospective study involved 91 individuals with lumbar facet joint disease-related chronic lower back pain (CLBP), all of whom underwent FMB-RFT. The patients were assigned to 3 groups using the Weishaupt facet grading system (WFGS). Pain scores were assessed prior to treatment, as well as at the 1-, 6-, and 12-month marks.
Results: Based on the WFGS, 38 of the 91 patients were assigned a grade 1 FJO, 28 a grade 2 FJO, and 25 a grade 3 FJO. The percentage of patients in each group who saw a 50% or greater improvement in their pain scores at 1, 6, and 12 months did not differ significantly.
Conclusion: For patients with CLBP, FMB-RFT has been shown to be safe and effective in both the short and long terms. The results from FMB-RFT do not seem to be affected by the severity of FJO.
Approximately 15-45% of cases of chronic low back pain (CLBP) are attributed to the facet joint.1,2 Recurrent micro- and macro-traumas may lead to synovitis, osteoarthritic changes, and capsular narrowing, culminating in axial CLBP.3 The pain frequently extends to the lower back and hip region.4 Lumbar hyperextension, extension-rotation, and paraspinal tenderness often exacerbate the pain, indicating the involvement of symptomatic facet joints.5,6 Radiologic findings, such as subarticular bone erosions, subchondral cysts, facet joint space narrowing or enlargement, and osteophytes, may be seen in facet joint osteoarthritis (FJO). Although the debate on the gold standard in diagnosis continues, many authors claim that facet medial branch blocks (FMBBs) serve as the most effective diagnostic test for confirming FJO-related pain.7
In patients with CLBP who are nonresponsive to conservative methods, facet medial branch radiofrequency thermocoagulation (FMB-RFT) is recognized as an efficacious and secure therapeutic approach. However, data regarding the factors influencing the success of FMB-RFT treatment in facet-induced pain are scarce. These data generally include participants’ demographic and clinical characteristics.9 Furthermore, data on the effects of the severity of FJO on the outcomes of RFT treatment are limited. The purpose of this study was to evaluate the impact of the Weishaupt facet grading system on the results of FMB-RFT treatment in patients with CLBP.
Methods
The medical data of patients with CLBP who received lumbar FMB-RFT at Ankara Bilkent City Hospital, Department of Pain Medicine, Ankara from June 2019 to June 2021 were reviewed retrospectively. Diagnoses were confirmed through clinical evaluation during physical examination, as well as through radiological assessment.
The inclusion criteria were as follows: I) individuals aged 35 years or older who are; II) experiencing axial low back pain for a minimum of 3 months; III) suffering from lumbar facet-related pain (back pain worsened by hyperextension or extension-rotation and local paravertebral tenderness); IV) patients who responded positively to diagnostic medial block (≥80% for temporary pain relief); and V) patients who have received lumbar FMB-RFT after failing to respond to conventional therapies under fluoroscopic guidance and those who have undergone lumbar computed tomography (CT) - magnetic resonance imaging (MRI) available before the intervention. The exclusion criteria were as follows: I) having an extruded or sequestered disc, spondylolisthesis, advanced spinal stenosis (spinal canal diameter <10 mm), or lateral recess syndrome (foraminal height <15 mm) on lumbar MRI; II) a history of lumbar interventional procedures within the last year (except diagnostic median branch blocks) or previous lumbar surgeries; and III) missing follow-up visits. Patients who responded positively to diagnostic medial block (≥80% for temporary pain relief) and gave consent for the procedure underwent the RFT procedure.
Ethics approval from Ankara City Hospital Ethics Committee No. 1 (approval number: E1-22-2968) and the participants’ informed consent were obtained. The research followed the guidelines provided in the Declaration of Helsinki.
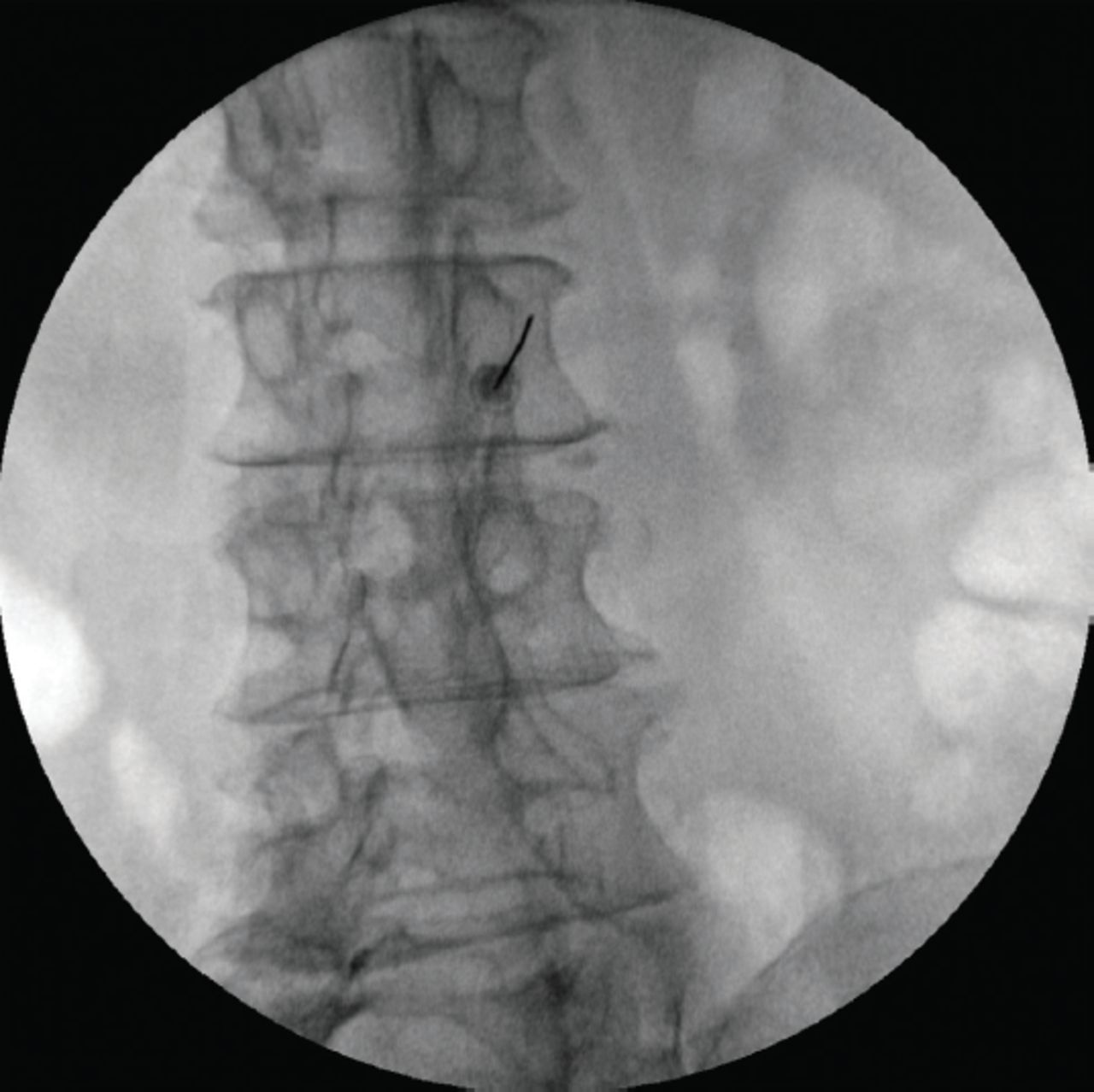
The procedures were carried out in an operating room with the patient positioned prone. Blood pressure, heart rate, and SpO2 were monitored. Fluoroscopy was utilized at a 30º oblique angle directed toward the treated side. A 21-gauge 10 cm radiofrequency needle equipped with a 10 mm active tip was navigated to the dog’s eye (Figure 1). The needle placement was confirmed with sensory (50 Hz, <0.5V - feeling of paresthesia in the waist) and motor (2 Hz, <1V - seeing multifidus muscle contractions and a lack of up to 2V motor activation in the legs) stimulations. One milliliter of 1% lidocaine was administered for analgesia upon confirmation of the needle’s precise position. Next, RFT was administered at 80°C for 60 seconds at a time at every level. For every facet joint block, 2 nearby median branches were blocked. In all cases, RFT was administered to the L3-4 median branches and to the L5 dorsal rami. Following RFT, 0.5 mL of saline and 1 mg of dexamethasone were injected.

- The “Scotty dog” sign and cannula placement during facet medial branch radiofrequency thermocoagulation.
The Weishaupt grading system was used to assess the severity of FJO on MRI and CT images.10 The following were the classifications of FJO: grade 0 (no narrowing, sclerosis, and osteophytes); grade 1 (hypertrophy in the facet joints); grade 2 (hypertrophy and minimal osteophytes in the facet joints); or grade 3 (hypertrophy in the facet joints, large osteophytes, and subarticular bone erosion). The CT and MR images were evaluated independently by 2 different physicians. The patients were categorized as grades 1, 2, or 3 using the Weishaupt facet grading system.
Demographic data, pain onset, and visual analogue scale (VAS) values were recorded from standardized patient chart forms. The VAS values (0= no pain, 10= worst possible pain) were routinely recorded in our clinic for pain assessment. These were evaluated at baseline and at 1, 6, and 12 months following treatment. A pain reduction of ≥50% was regarded as significant pain relief.
Statistical analysis
The Statistical Package for the Social Sciences, version 25.0 (IBM Corp., Armonk, NY, USA) was used. The Kolmogorov-Smirnov test was utilized to evaluate normal distribution. Quantitative data following a parametric distribution are reported as means ± standard deviations (SDs), whereas for non-parametric variables, the median and interquartile range (IQR) are presented. To investigate the correlation between the significant pain relief ratio and FJO grade, a Chi-square test was carried out. Additionally, Spearman correlation analysis was employed to identify potential variables associated with significant pain relief. A p-value of ≤0.05 was the threshold for statistical significance.
Results
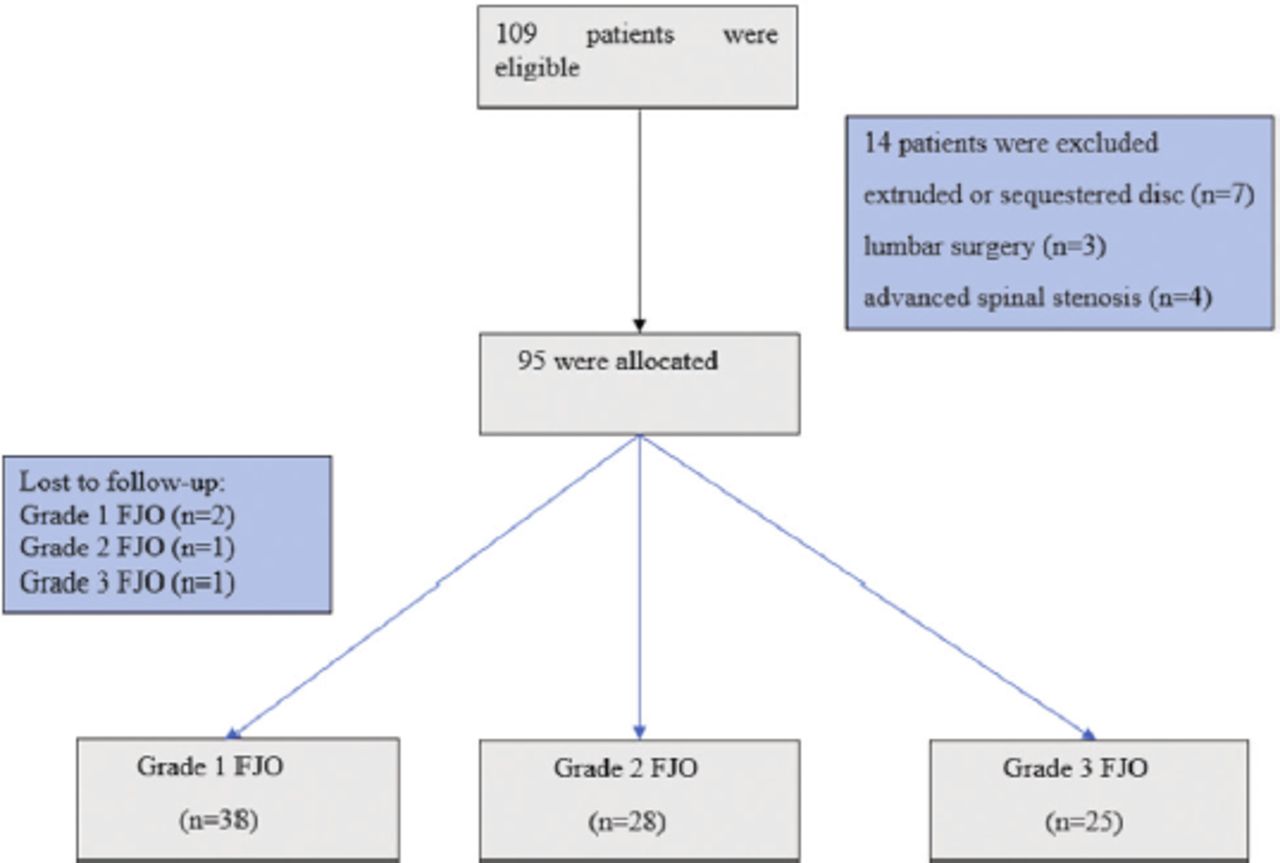
Figure 2 presents the consort flow diagram. The descriptive features and pain-related attributes of the patients are summarized in Table 1.

- Consort flowchart of the studied patients. FJO: facet joint osteoarthritis
- Demographic and pain characteristics of the patients.
The patients in the grade 1 FJO group were considerably younger than those in the grade 2 and grade 3 groups (p=0.006 and p=0.001). Between the groups, there was a notable variation in body mass index (BMI; p=0.032). No statistically significant differences were observed between the groups for pain duration or VAS scores at baseline, 1 month, 6 months, and 12 months (p>0.05; Table 2).
- Demographic features of the patients regarding the stage of facet joint osteoarthritis.
The percentage of individuals who experienced significant pain relief was nearly 80% during the first month, but it dropped to 65% by the sixth month and further declined to 47% after 12 months.
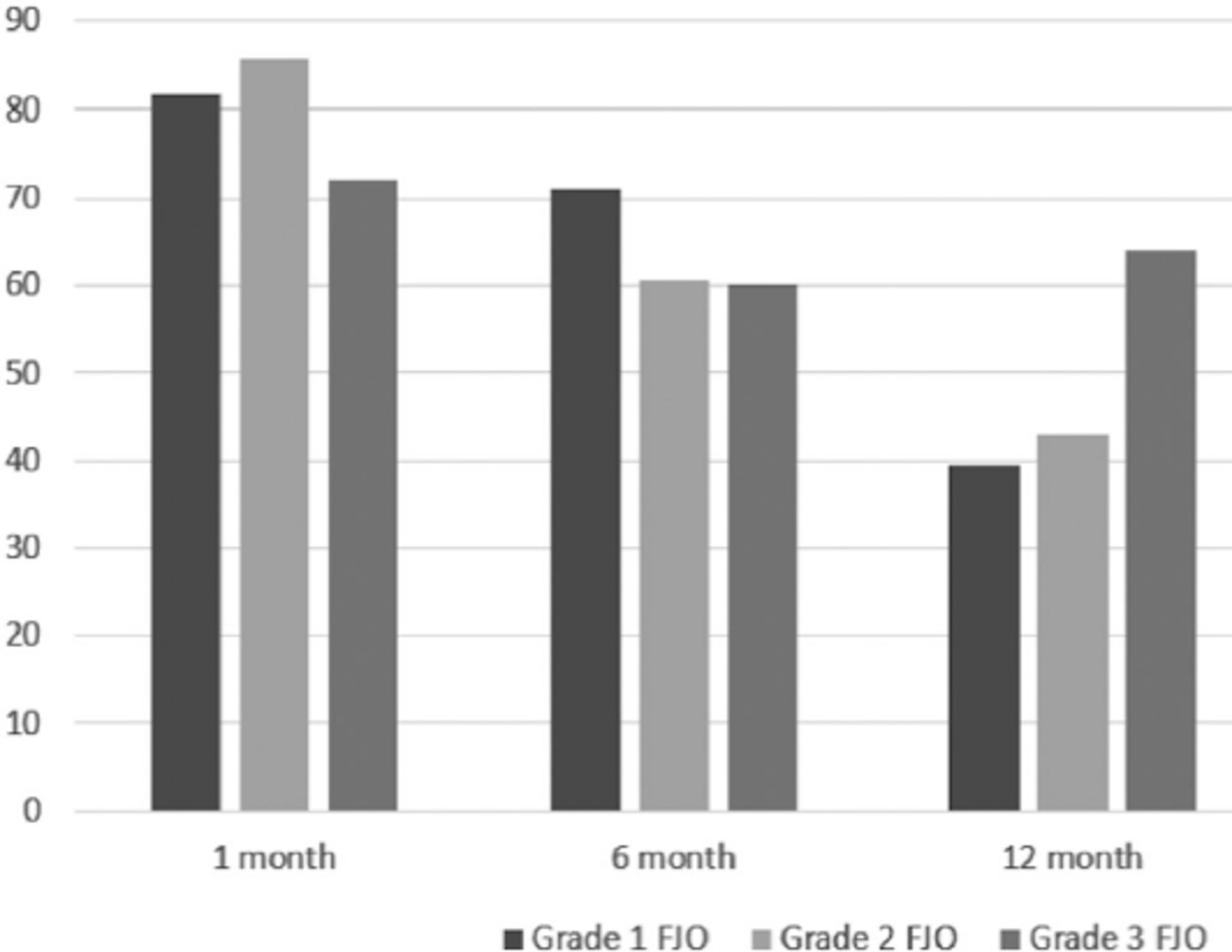
The relationship between the grade of FJO and the ratio of significant pain relief at 1, 6, and 12 months was analyzed and is shown in Figure 3. The percentage of patients achieving more than 50% improvement in VAS scores at these time points showed no significant differences among the groups categorized by FJO grade (month 1 [p=0.440], month 6 [p=0.574], and month 12 [p=0.139]).

- Significant pain relief rates of the patients regarding the grade of FJO at the 1st, 6th, and 12th months. There was no significant difference between the groups at each time point (p>0.05). FJO: facet joint osteoarthritis
Correlation analysis revealed a moderate positive correlation between age and FJO grade (p=0.001), and a weak positive correlation between BMI and FJO grade (p=0.008). Significant pain relief at 1, 6, and 12 months did not correlate with the examined variables (age, gender, BMI, and pain duration) and FJO grade (Table 3).
- Correlation analysis of the possible factors related to significant pain relief.
No complications or adverse effects related to the RFT procedure were noted.
Discussion
Micro and macro traumas or repetitive stress that occurs with age in the facet joint cause synovitis and synovial cell proliferation. As this degeneration progresses, it results in arthrosis of the facet joint.11 Degenerative alterations in the facet joints contribute to localized inflammation, leading to CLBP. Weishaupt et al10 evaluated facet joints with CT and MRI and staged them according to osteoarthritic changes. Wang et al12 observed an association between facet joint degeneration and FJO degree.
The relationship between radiologically assessed FJO and lower back pain remains a contentious topic. In some studies, it has been reported that there is no relationship between the presence of FJO and its severity on CT or MRI and lower back pain.13-15 Unfortunately, most of these studies did not use reliable and well-designed criteria for diagnosing FJO. Klessinger et al16 reported that painful joints were large in diameter and that the degree of osteoarthritis was high in painful joints. They found a higher rate of grades 2 and 3 FJO in patients with pain, and they did not detect grade 3 FJO in any of the asymptomatic patients. Hicks et al17 and Suri et al18 asserted that the severity of FJO was correlated with lower back pain in older individuals.
Thus far, the effect of FJO severity on FMB-RFT outcomes has only been examined in one study, with the current study being the second to investigate it. Balázsfi et al19 assigned patients who underwent FMB-RFT (80ºC for 60 seconds) into 3 groups according to the Fujiwara grading system. According to their findings, in grade 2 or 3 patients, the percentage of significant pain reduction was 51.4% at 6 months and 27.1% at 12 months. In grade 4 patients, the rate of significant pain relief was 3% at 6 and 12 months; none of the patients achieved significant pain reduction. They noted a long-term success rate of 15.5% in grade 1 patients. In our study, we could not find a correlation between FJO stage and treatment outcomes, contrary to Balázsfi et al’s study.19 In addition, our success rates were higher than those of the aforementioned study, although we applied RFT to the same degree and duration. This discrepancy may have resulted from the inclusion of patients who had undergone back surgery in Balázsfi et al’s study,19 which might have lowered the success rate. They reported that the vast majority of patients who had previous spinal surgery did not benefit from the treatment. For example, among patients with grade 1 FJO, none of the patients who had recovered for at least 6 months had undergone spine surgery.
Additionally, 2 studies examined the impact of FJO severity on the efficacy of facet joint injectios and FMBBs in CLBP patients. Kayalar et al20 assigned patients who underwent facet joint blockage with 40 mg of methylprednisolone acetate and 5 mg of bupivacaine to 3 groups according to the Weishaupt facet grading system. In all groups, they found a significant pain reduction with facet joint blockade but found no correlation between osteoarthritis severity and treatment results. Our study also revealed that FJO severity did not have any effect on the treatment outcomes, supporting the findings of Kayalar et al.20 However, some fundamental differences between the 2 studies should be considered. While Kayalar et al20 carried out facet joint injection, we carried out FMB-RFT. In addition, a major shortcoming of their study was that they did not specify how many joints they blocked, nor did they identify the post-injection evaluation period.
Klessinger et al16 tested patients with unilateral lower back pain with FMBB. They compared the MRI scans of positive responders with normal MRI scans and concluded that MRI could not positively predict the effect of FMBB. However, they reported that grade 0 FJO may be a negative predictor of the FMBB effect. Unlike Kayalar et al’s study,20 in the current research, FMBB was carried out instead of a joint blockade. Although different facet injections were applied in the 2 aforementioned studies, treatment outcomes have been reported to be unrelated to FJO severity. In the present study, we did not detect any effect of FJO on treatment outcomes at any time (1, 6, or 12 months) after RFT therapy, which is consistent with the findings of these studies.
Some researchers have evaluated the factors that affect RFT success in facet-induced CLBP. Cohen et al9 reported a negative correlation between FMB-RFT success and a long pain duration. Additionally, they stated that obesity and facet abnormalities on MRI were unrelated to RFT results. Stelzer et al21 reported that gender did not affect RFT results and that these results were more successful in patients with BMI of <30. In our study, we did not note any correlation between RFT results and age, gender, BMI, pain duration, or FJO grade.
In a meta-analysis, the efficacy of RFT in treating CLBP demonstrated level II evidence.8 In the literature, different results with the success rates of facet median branch RFT have been reported. Ertilav et al22 found the success rates of RFT to be 63.5% at one month and 57.2% at 6 months. They randomized patients into the following 3 groups according to RFT temperature and time: 90ºC for 50 seconds, 85ºC for 60 seconds, and 70ºC for 90 seconds. In the end, they found the 3 groups to be similar in terms of effectiveness. Manchikanti et al23 reported RFT success as 100% at 3 months, 74% at 6 months, and 65% at 12 months of follow-up. Our success rates were higher than those of Ertilav et al22 and lower than those of Manchikanti et al23 The fact that Manchikanti et al23 achieved higher success rates despite the same degree of (80ºC) RFT applications may be due to the RFT applications being twice as long as ours (120 seconds versus 60 seconds). The reason for these different results may be the various temperatures and durations of RFT in the studies.
Study limitations
A retrospective design, and it lacks functional metrics. Further research is required to determine all possible parameters influencing the success of RFT in the treatment of CLBP.
In conclusion, the findings suggest that FMB-RFT is beneficial and safe in patients with CBPL. The severity of FJO before RFT treatment has no effect on the treatment outcomes.
Acknowledgment
The authors gratefully acknowledge Scribendi for their English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received April 24, 2024.
- Accepted January 21, 2025.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.