


Abstract
Objectives: Guillain–Barre syndrome (GBS) is an acute autoimmune-mediated peripheral nervous system disease. Different studies from various geographical regions have reported considerable variability regarding its epidemiology, clinical features, and outcome. Our study aimed to document demographics, clinical features, and outcomes among GBS patients admitted to a single tertiary care hospital in Muscat, Oman.
Methods: A retrospective data analysis of 44 GBS patients, who were admitted during a two-year period from January 2016 to December 2018 at Khoula hospital, was carried out. Demographics, antecedent illness, duration of symptoms, muscle power graded by the Medical Research Council scale (MRCs), sensory & autonomic involvements, nerve conduction study results, CSF study, need for ventilation, condition at discharge and subsequent follow-up status were obtained.
Results: Ninety-one percent of the patients were Omanis, with male predominant 63.6% and the average age was 42.69 years. Quadriparesis was the predominant presenting complaint (61.3%) and AIDP was the commonest variant (52%). All patients received a single cycle of IVIg and (13.6%) patients admitted to the ICU for mechanical ventilation. The study showed good outcome and recovery in 18 months follow up.
Conclusion: The clinical presentation of GBS in the majority of patients in Oman is similar to those reported in previous studies, and most patients had favorable prognoses. Our results can be used as baseline data for understanding the characteristics of GBS in Oman and, consequently, for better management.
Guillain–Barre syndrome (GBS), also known as Landry’s paralysis, is an acute immune-mediated polyradiculoneuropathy;1,2,3 with males are about 1.5 times more affected than females, and an overall incidence rate of 1–2 per 100,000 population per year worldwide.4,5 The syndrome is characterized by an acute or subacute progressive generalized muscle weakness of upper and lower limbs with relative or complete areflexia, and limb paraesthesia.1 The typical pattern starts with typically ascending flaccid paralysis, which progresses over a few days to a few weeks. Patients may also develop cranial nerves involvement, usually as a facial or pharyngeal weakness. In addition, autonomic dysfunction is common in the disease, which manifests as postural hypotension, loss of vasomotor control (causing wide fluctuation in blood pressure), and a variety of cardiac arrhythmias. Ventilator assistance is required when respiratory failure and oropharyngeal weakness develop in the course of the disease, which has been reported to be required in approximately one-third of hospitalized patients; these data indicate that early management is vitally important for GBS.1,3
Proceeding infections (such as infections with Campylobacter jejuni, Cytomegalovirus, Epstein–Barr virus, Mycoplasma pneumonia, and HIV)2,4,5,6,7 may activate the immune response, owing to molecular mimicry, to cross-react with the peripheral nerve’s components (the myelin and/or the axon) resulting in the endoneural inflammation of spinal nerve roots, nerve’s distal segments, and at potential nerve entrapments sites.2 Some triggering factors (e.g., immunization, trauma, bone marrow transplantation, and surgery) may also affect the pathogenesis of GBS .6⇓–8
Seasonal variability is reported for GBS, which can reflect seasonal changes in the peaks of the predisposing factors, such as infections, although GBS may occur during any season.9,10 Seasonal occurrence has been reported to peak during the summer season in Asian countries.11,12
The GBS is believed to include a variety of acute neuropathies with underlying immune-mediated pathogenic mechanisms rather than a single disease; therefore, GBS recognized variants are considered as syndromes [including acute inflammatory demyelinating polyneuropathy (AIDP), acute motor axonal neuropathy (AMAN), acute motor-sensory axonal neuropathy (AMSAN), and Miller–Fisher syndrome]. The most prevalent form of GBS reported is AIDP which is responsible for 70–90% of cases.5,6 In addition to history and clinical examination, confirming the diagnosis of GBS may include cerebrospinal fluid (CSF) analysis and electroneurodiagnostic testing, both of which can be normal in the early phase of the disease.3,4
Therapeutic plasma exchange (TPE) and intravenous immunoglobulin (IVIg) are used effectively for adult and pediatric patients with GBS; and if these treatments are administered during the first few weeks of the disease along with a efficient supportive care, they can minimize mortality and improve the outcome of the disease.13,14 Physical therapy is considered as an essential part of the supportive management for decreasing complications’ incidence, such as respiratory complications and deep venous thrombosis (DVT), as well as for pain management and to enhance early mobilization.15
The understanding of clinical presentation and epidemiology of GBS in each population can help us better understand the pathogenesis of the disease, its risk factors, and prognosis.16 Moreover, the evaluation of GBS outcome may be effective for planning an appropriate therapeutic strategy and for determining disease-related morbidity and mortality. The results of different studies from various geographical regions have reported considerable variability regarding the epidemiology, clinical features, and outcomes of GBS.17,18 Therefore, our study aims to assess the presentation, clinical findings, demographics, seasonal variations, and outcomes among patients with GBS in a tertiary care institute in Muscat, Oman.
Methods
This study is an observational, retrospective and descriptive study. Data analysis of 44 GBS patients, who were admitted to a tertiary care hospital (Khoula Hospital) in Muscat, Oman from January 2016 to December 2018, was carried out after obtaining ethical approval by the Institutional Ethics Committee (code No. PRO04202056).
The GBS patients were included according to the modified criteria for GBS diagnosis developed by the National Institute of Neurological Disorders and Stroke (NINDS).19⇓–21 Patients who did not fulfill the diagnostic criteria and those with co-morbidities were excluded from the study.
The patient demographics features and clinical characteristics were collected and included the age, gender, antecedent illness, duration of symptoms at admission, time to report to the hospital, muscle power grade by using Medical Research Council sum score (MRC-SS) at 18 months of follow up, sensory and autonomic involvement, and cranial nerve paralysis. Ancillary investigations (e.g., nerve conduction study and CSF test results) were extracted from the medical files. The data of hospital course, Intensive Care Unit complications, need for ventilation, and treatment plan were collected.
In this study, the outcome analysis was not limited to the period of hospital stay of the patients; a clinical follow up at regular intervals was made at 6, 12, and 18 months after discharge to determine their functional recovery. The MRC-SS 22 was utilized to assess the outcome and grade of recovery for each patient, by the end of the 18-month follow up. We divided recovery grade and outcome into 4 categories using the MRC sum score (maximum score of 60):23 Full recovery: Normal (no residual weakness, the MRC-SS score of 60); Good recovery (minor residual weakness with the MRC-SS score of >45); Partial recovery (significant residual weakness with the MRC-SS score of 20–45); Limited recovery (disabled with the MRC-SS score of <20).
Statistical analysis
Only descriptive data are used, e.g. percentages and frequencies are calculated for categorical (nominal and ordinal) data; and averages (means, medians, and ranges) with standard deviations are calculated for continuous data. The primary method used for searching the related research literature was by using the electronic databases. These include PubMed, Trip database, OpenMD, Grepmed, and JSTOR.
Results
Of the 44 patients, 28 were males (63.6%). The mean age of all patients was 42.69±19.67 years old with a range of 26–63 years for males and 17–76 years for females; and a male-to-female ratio of 1.75:1 (Table 1).
Age and Gender characteristics of the patients.
Ninety-one percent of the GBS patients (40 patients) were Omani, and only 4 patients (9%) were expatriates. Most Omani patients (54.5%) were from the Muscat area. All patients developed their neurological illness within 2 weeks of symptoms’ onset, and 6.4 days was the average duration from the onset of symptoms until reporting to the hospital.
A total of 31.8% of the patients had a history of preceding illness, which was mainly a flu-like illness and upper respiratory infections (in 7 patients). Gastritis was identified as a prior disease in 5 patients (Table 2). The majority of the patients (61.3%) were admitted to the hospital with progressive weakness in all 4 limbs (quadriparesis) as a common clinical feature followed by paraparesis (in 34% of patients). Respiratory distress and sensory symptoms were noted in 7 patients (16%). Bladder involvement was the least observed clinical feature (only in 4.5% of the cases); Table 3.
Antecedent events observed in GBS patients.
Symptoms of the GBS patients.
All patients underwent a nerve conduction study within the second week of the symptoms’ onset to confirm the clinical diagnosis and to uncover the underlying pathophysiologic variant. The majority (52%) of the patients had AIDP. However, 30% of the patients had AMAN, whereas only 14% of the patients had AMSAN. Only two patients (4%) presented the Miller Fischer variant (Figure 1).

Guillain-Barre variants. AIDP - acute inflammatory demyelinating polyneuropathy, AMAN - acute motor axonal neuropathy, AMSAN - acute motor-sensory polyneuropathy.
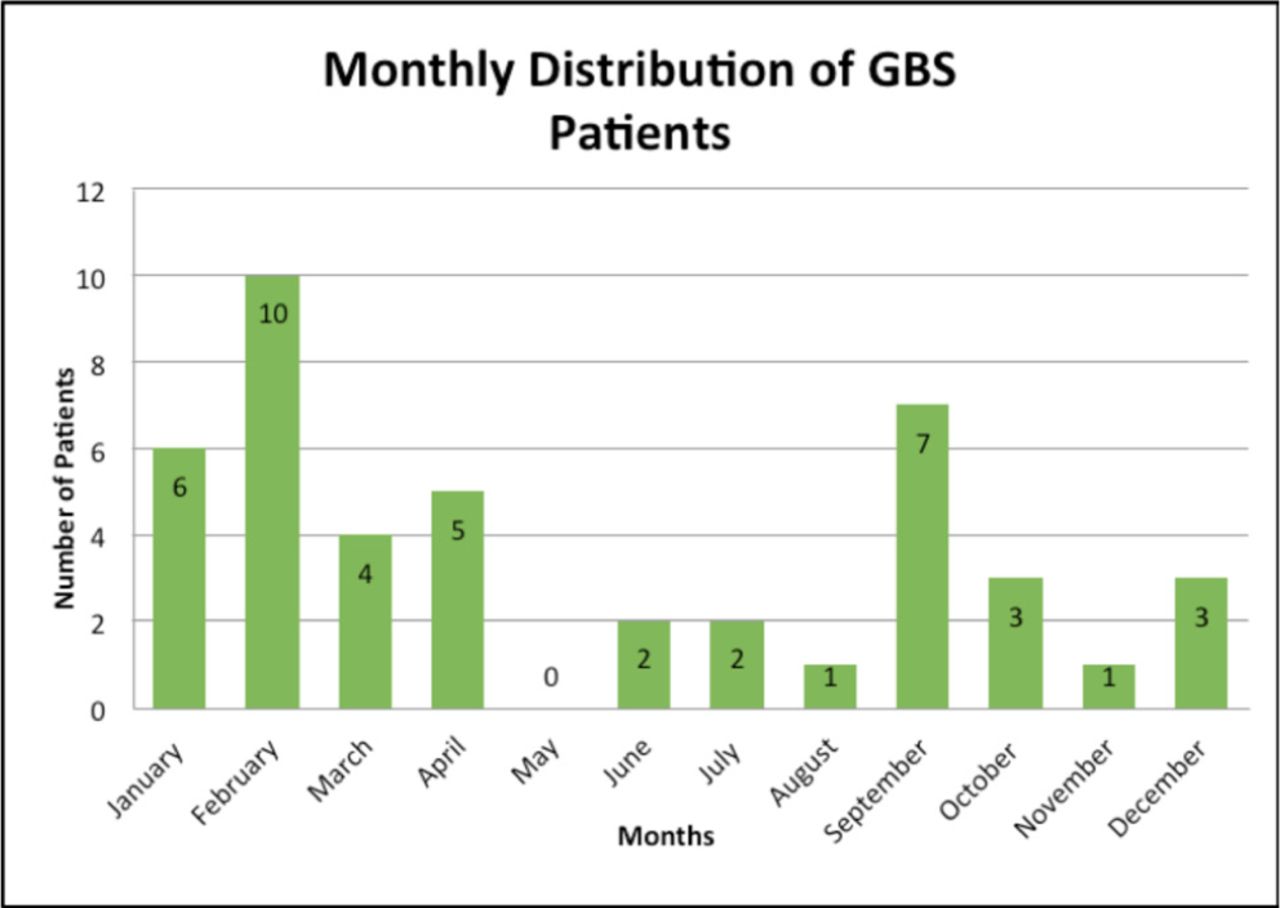
The disease showed sporadic occurrence throughout the year; as the number of patients was found to be highest during February and September (Figure 2). A total of 36 patients (81.8%) had a raised CSF protein. A total of 6 patients (13.6%) were admitted to ICU for mechanical ventilation. All patients received a five-day cycle of IVIg. A total of 8 patients (18.2%) had a second cycle of IVIg, and 6 patients (13.4%) underwent plasma exchange.
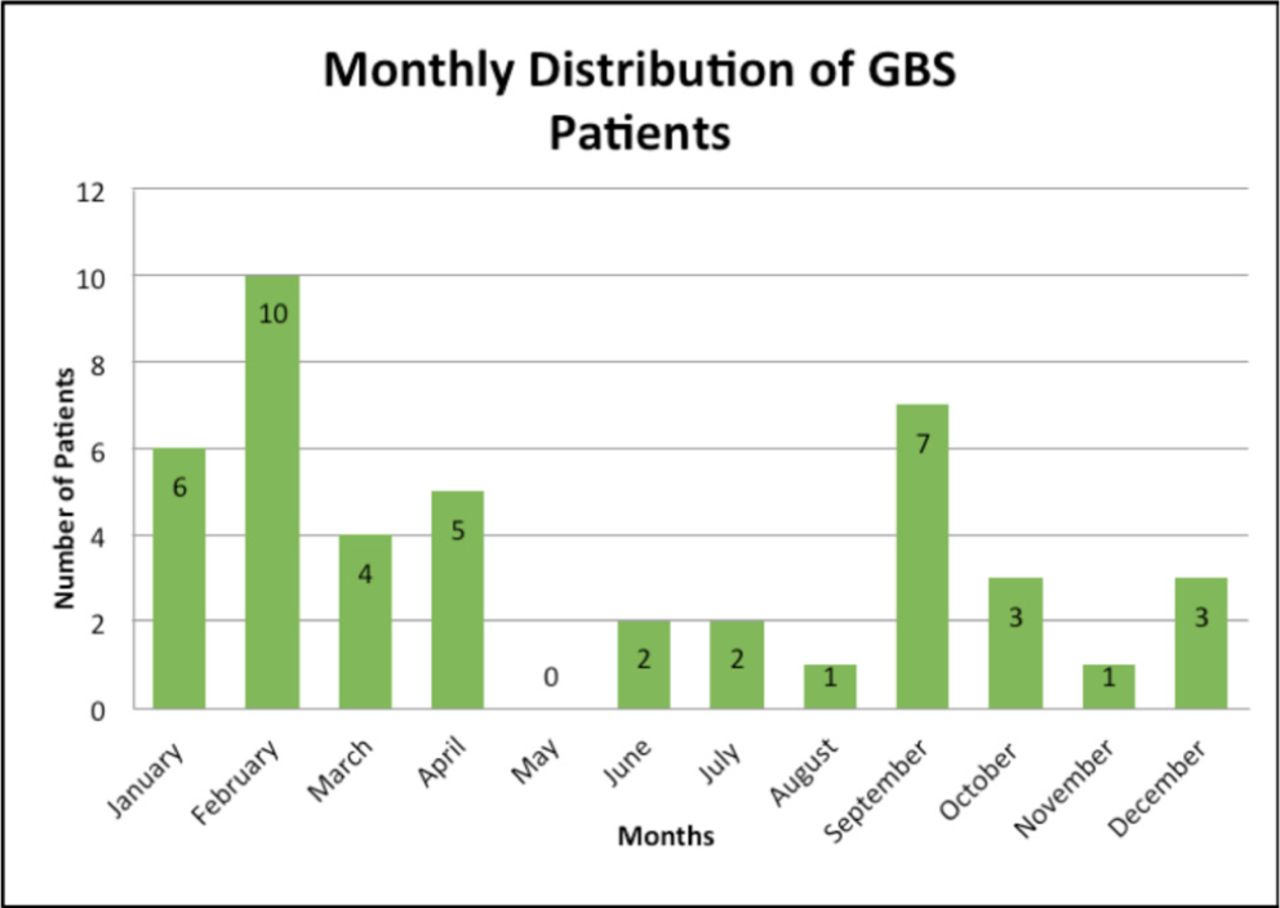
Monthly distribution of Guillain-Barre cases.
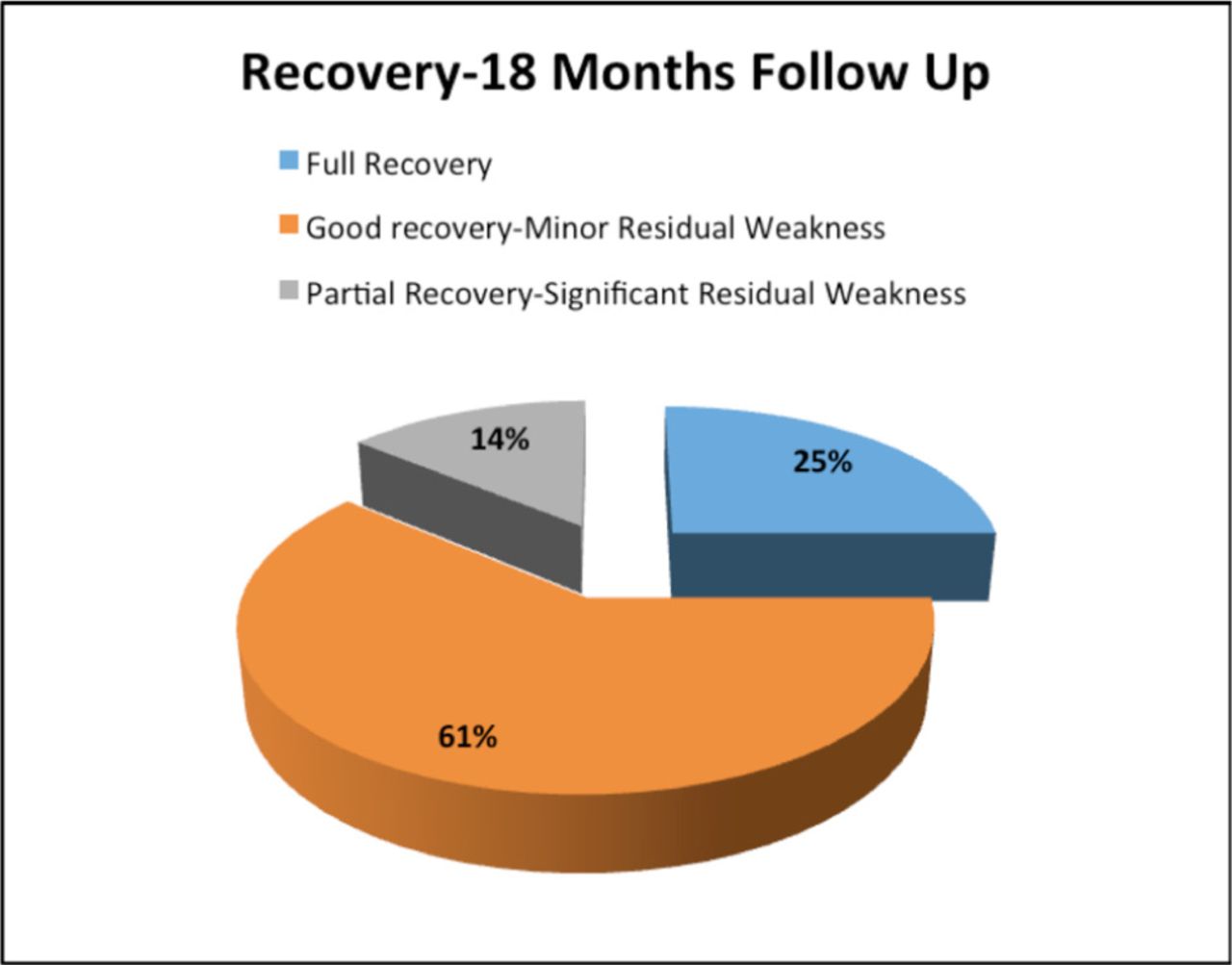
The outcome analysis was assessed after 18 months, using the MRC-SS score categorization. Specifically, only 11 patients (25%) showed full recovery, 27 patients (61.3%) showed good recovery but with minor residual weakness, and 6 patients (13.7%) had partial recovery with significant persistent weakness (Figure 3). There were no patients with limited or no recovery.
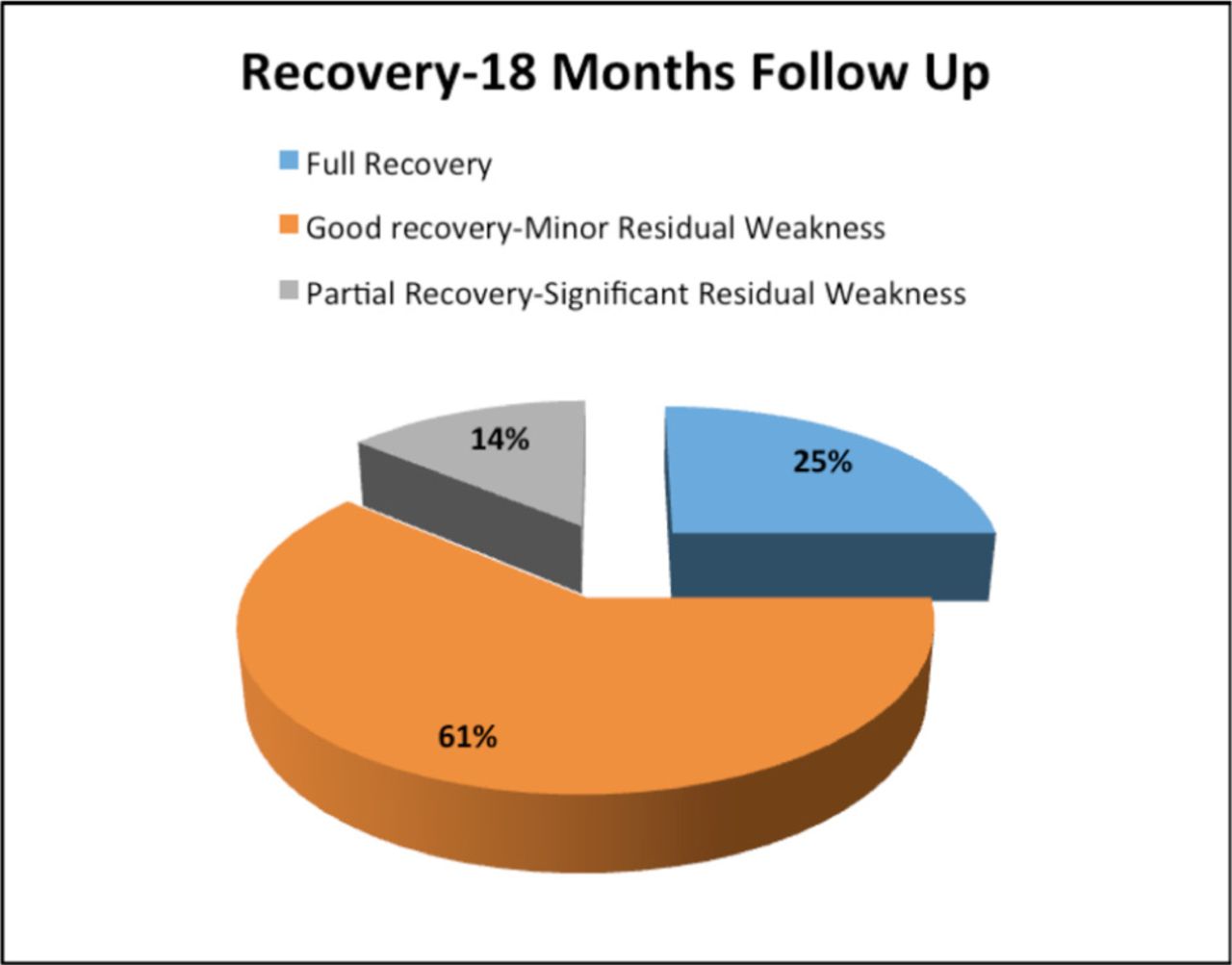
Follow up recovery results.
Discussion
Our study showed a male preponderance among the GBS patients in Oman with 1.75:1 male: female ratio, which was similar to what has been reported by other studies.1,4,5,8,12 In addition, upper respiratory tract illness, followed by gastroenteritis, was the most common antecedent illness, which was similar to what has been reported in earlier studies.9
Progressive muscular weakness of all four limbs (Quadriparesis) was the commonest clinical feature among our patients, which was similar to what has been reported in other studies;4,24 however, our study showed fewer patients with cranial nerve involvement (only in 6.8% of the patients) as compared to others’ reported range. Cranial nerve affection in GBS is common and many studies quote a variable range of 50% to 75% involvement of cranial nerves;25⇓–27 however, in these reports, all studied patients having cranial nerve palsies had evident quadriparesis, which suggested a more severe illness.
Anandan et al28 have shown that autonomic dysfunction most frequently manifests as diarrhea/constipation (15.5%), hyponatremia (14.9%), syndrome of inappropriate antidiuretic hormone secretion (SIADH, 4.8%), bradycardia (4.7%), and urinary retention (3.9%), in hospitalized patients with GBS. The frequency of autonomic dysfunction (which manifested as bladder dysfunction in our study) was 4.5%, which was similar to the previously reported percentage but lower than the rates reported by other studies.18,29 The persistence of autonomic changes is very rare in GBS patients, and dysautonomia is reported to occur more frequently in patients having severe weakness and in those who develop respiratory failure.28
Respiratory paralysis is a terrible complication of GBS, which occurs in up to 40% of patients.3,30,31 In our study, only 13.6% of patients received ventilator support owing to respiratory insufficiency. In a prospective multicenter study in Germany, 13% required artificial ventilation,25 which is similar to our finding.
The most common variant of GBS among the studied patients was AIDP followed by AMAN. Other studies, from different parts of the world, have shown similar variant prevalence but with higher frequency. Studies from Europe and the USA have reported that 60-80% of GBS patients had the demyelinating subtype, while AMAN has been reported to affect only a small percentage (6–7%).24,32 However, the reports from Asia and Central and South America have shown a considerably higher percentage for AMAN (30–67%).33⇓⇓–36 This variation in the distribution of subtypes between countries may be related to the exposure to different types of infections; however, the genetic characteristics of the population may also have an effect.24
In this retrospective analysis, 2 occurrence peaks were found for GBS patients, one in February and the other in September. The seasonal and monthly variation may be attributed to sudden temperature differences in seasonal conditions, which makes certain months more prone to infections. Climatic conditions may vary from region to region within the country and in other parts of the world, which produces differences in the observations. A similar bimodal incidence of GBS maximum occurrence in spring and winter has been reported.37,38
In this study, 61% of patients had good recovery with a minor residual weakness, and 25% had a full recovery after 18 months, which was similar to the outcome reported in a study from India.3 This good rate of recovery can be attributed to the early detection of symptoms and to the early intervention, which are important factors for the better prognosis of GBS.39 The mean time of admittance to hospital was only 6.4 days in our studied patients and all of them were given IVIg or TPE early in the course of the disease. Our patients were treated with IVIg regardless of the severity of their symptoms, which could explain the favorable outcome demonstrated in our study.
The mortality rate in an epidemiologic study carried on in 2008, has been reported to be 2-12% despite ICU management 40 and is less than 5% in tertiary care centers with medical professionals’ team familiar with GBS management.41 In contrast, our study showed no mortality among the patients included and followed up. Although this finding can be a serendipitous result to the modest sample size of this study, the early initiation of treatment can be a factor too; since it is reported that IVIg and TPE treatments when given during the first few weeks of the GBS symptoms, combined with efficient supportive care, can minimize mortality and improve the outcome of the disease.13,14 In view of the absence of evidence and guidelines; the management of GBS varies between different centers. In present practice, patients with mild and variant forms of GBS, or with treatment-related fluctuations and treatment failures, are often treated, even in the lack of randomized clinical trials or guidelines to support this choice.42
In conclusion, the clinical presentation of GBS in the majority of patients in Oman was mostly similar to what has been reported by previous studies, and most of the included patients had favorable prognoses. Our results can be used as baseline data to better understand the characteristics of GBS in Oman and, consequently, for the better management of the disease, as well as for further research related to immune-mediated neuropathies.
The limitation of our study is that it was an observational retrospective analysis with a small sample size. Additionally, the assessment of disease severity in the acute phase could not be retrieved retrospectively. A well-designed prospective analysis of a larger sample of GBS patients, from different healthcare centers and hospitals, needs to be carried out to achieve more reliable and representative data, which can lead to the best outcomes.
Acknowledgements
We would like to thank Falcon Scientific Editing (https://falconediting.com/cn/catalog/editing-cn) for English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received May 21, 2020.
- Accepted July 7, 2020.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.