


Abstract
Epilepsia partialis continua (EPC) is a rare type of focal motor seizure characterized by continuous, involuntary muscle contractions in a specific part of the body. These contractions usually involve rhythmic, twitching movements and can last for several hours to days. The seizures are usually limited to one part of the body and can be clonic or dystonic. EPC can affect people of all ages but is more common in children and adolescents. The pathophysiology of EPC is complex and depends on the cause. There are several possible causes of EPC including structural brain abnormalities, infections, metabolic and genetic disorders, inflammatory conditions, traumatic brain injury, and vascular causes. The work-up of EPC includes electroencephalography (EEG), magnetic resonance imaging (MRI) of the brain, position emission tomography (PET) scan of the brain, autoimmune antibodies, infection work-up, and metabolic and genetic work-up. The management of EPC can be challenging. Antiseizure medications (ASDs) including benzodiazepines are an integral part of the management of EPC. Immunotherapy trials are recommended in resistant cases. Epilepsy surgery is one of the effective modalities in some surgically amenable cases. This article reviews the topic of EPC and summarizes diagnostic and .treatment recommendations
The International League Against Epilepsy “ILAE” defines EPC as a syndrome of continuous, localized motor seizures that persist for more than an hour, often over the course of days or even years.1 The seizures are usually limited to one part of the body and can be either clonic (involving rhythmic muscle contractions) or dystonic (involving sustained muscle contractions).2 The term “partialis” refers to the fact that the seizure activity is limited to a specific part of the body, while “continua” indicates that the seizure activity persists for an extended period.3 The EPC typically affects one limb, such as an arm or leg, but it can also affect the face, tongue, or other body parts.4 The muscle twitching or jerking is usually mild, but it can be severe enough to interfere with daily activities such as writing, walking, or eating. Unlike other forms of epilepsy, EPC does not cause a loss of consciousness.4 The EPC is classified as a type of focal seizure, which means that it starts in a specific area of the brain. It is often associated with underlying neurological conditions.5 The first documented case of epilepsia partialis continua was in the late 19th century by the German neurologist Carl Westphal. He described a patient with continuous, localized muscle twitching in one limb, which he referred to as “continuous muscular twitching.” Over the years, various terms have been used to describe this condition, including “simple partial status epilepticus,” “focal motor status epilepticus,” and “partial continuous epilepsy”.6 In 1989, the ILAE proposed the term Epilepsia Partialis Continua to describe this specific type of epilepsy.1 Since then, there have been numerous case reports and studies on EPC, which have improved our understanding of the clinical features, underlying causes, and treatment options for this rare form of epilepsy.
Epidemiology
The incidence of EPC in the general population is not well established. However, several studies have reported on the frequency of EPC among patients with epilepsy.7,8 These studies has also concluded a higher prevalence in males than in females.7,8 One study conducted in Europe evaluated 2,437 patients with epilepsy and found that EPC accounted for only 0.1% of all cases.9 Another study from Japan reported a slightly higher prevalence, with EPC accounting for approximately 1.5% of all cases of epilepsy.10 A study conducted in India found that EPC accounted for 2.5% of all cases of focal epilepsy.11 In children, EPC appears to be even rarer. A study from Spain that evaluated 1,337 children with epilepsy found that only 0.2% had EPC. Another study from Japan reported that EPC was present in only 0.6% of children with epilepsy.12 Overall, the available literature suggests that EPC is a rare form of epilepsy, accounting for less than 3% of all cases of epilepsy. However, it should be noted that the frequency of EPC may vary depending on the population studied.
Pathophysiology
The pathophysiology of EPC is complex and not completely understood. It is believed to involve a combination of factors and different etiologies that lead to the generation and maintenance of abnormal electrical activity in the motor cortex. These multiple etiologies (inflammatory, structural, etc…) can cause an imbalance between excitatory and inhibitory neurotransmission, changes in ion channel function, and alterations in synaptic connectivity. Moreover, the spread of abnormal electrical activity to adjacent cortical and subcortical structures may contribute to the persistent motor symptoms observed in EPC.13,14
Etiologies
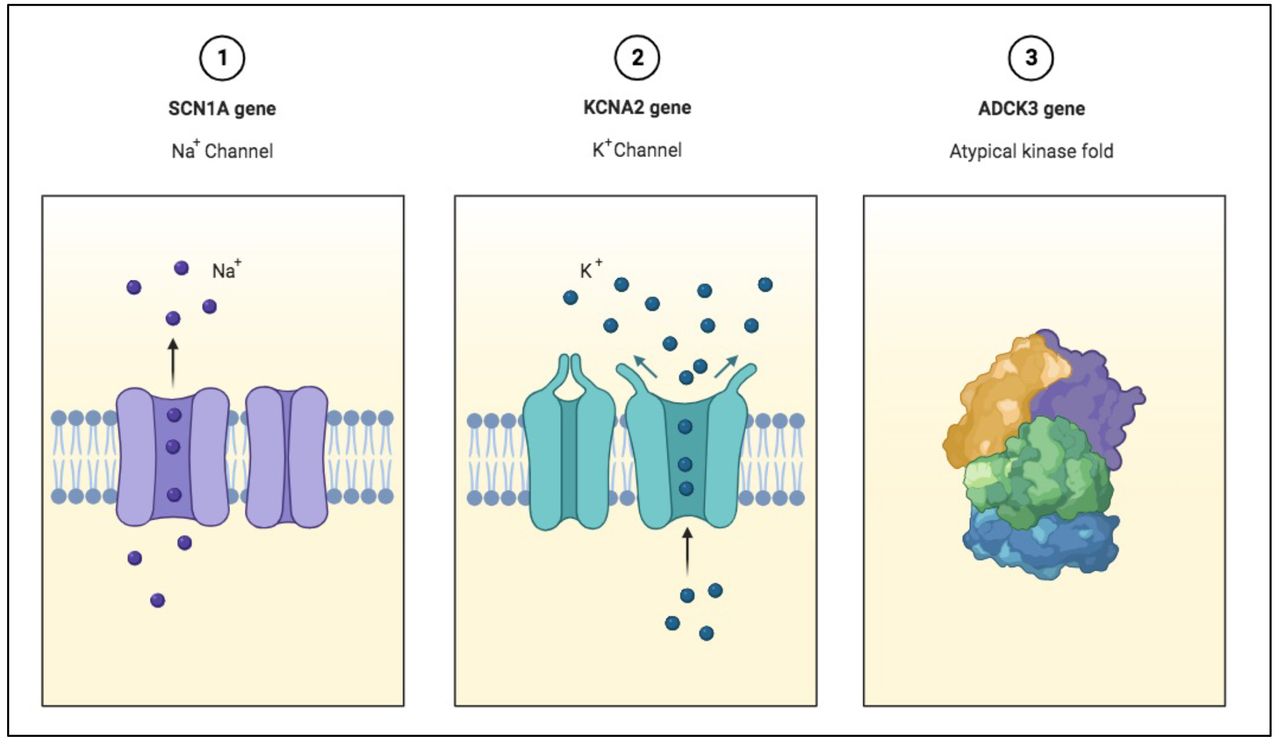
The EPC can have various underlying causes, including structural, metabolic, genetic, vascular, infectious, and autoimmune etiologies. In some cases, the cause is unknown (Table 1). One study conducted in Japan found that structural abnormalities were the most common cause of EPC, accounting for 60% of cases.15 These included brain tumors, stroke, and traumatic brain injury. In another study from India, structural abnormalities were identified in 36% of cases of EPC, with brain tumors and malformations being the most common causes.15 Brain tumors, stroke, and traumatic brain injuries are all known causes of EPC, and they account for a significant proportion of cases of this condition.14 Brain tumors are a common cause of EPC, and they can be either primary or metastatic. In one study, brain tumors were identified as the cause of EPC in 30% of patients. The most common types of tumors associated with EPC were gliomas and meningiomas.16 Stroke is another cause of EPC, and it usually results from a focal ischemic or hemorrhagic lesion in the brain. EPC may occur as a result of the focal lesion caused by the stroke or due to post-stroke epilepsy.17 The prevalence of EPC in patients with stroke varies between studies. In one study, EPC occurred in 10% of patients with stroke, with a higher incidence in patients with cortical or subcortical ischemic stroke. Another study reported an incidence of 2.5% in patients with hemorrhagic stroke.17 Post-stroke epilepsy is another potential complication of stroke, and it can occur in up to 20% of patients. The risk of post-stroke epilepsy is higher in patients with cortical or subcortical lesions, as well as in patients with a history of previous stroke or head injury.17 Traumatic brain injury (TBI) is also a known cause of EPC, and it can result from direct impact or acceleration-deceleration forces on the brain. In one study, TBI was identified as the cause of EPC in 9% of cases. The seizures in these cases may be difficult to control with medication, and surgical intervention may be necessary to prevent further brain damage. Another structural brain abnormality that can present with EPC is focal cortical dysplasia (FCD). This developmental abnormality of the brain can cause cortical irritation. Cortical dysplasia refers to a group of disorders in which the normal development of the cerebral cortex is disrupted, leading to abnormal neuronal migration, organization, and connectivity. Cortical dysplasia was reported to be the cause of EPC in 2.5 to 5.6% in different studies. Also, FCD can present with EPC in cases diagnosed with tuberous sclerosis complex (TSC).17 Infections of the central nervous system, such as meningitis and encephalitis, are also implicated in the etiology of EPC. The incidence of EPC associated with infections is relatively low. Infections accounted for about 7.5% of cases of EPC in published cases series. The most common infectious etiology was herpes simplex encephalitis, followed by tuberculous meningitis. In addition to meningitis and encephalitis, other infections of the central nervous system, such as human immunodeficiency virus (HIV) and neurocysticercosis, have also been reported as a cause of EPC.18 Autoimmune and inflammatory conditions are well-known causes of EPC. These conditions can lead to an inflammation cascade and result in seizures and focal weakness in some cases. Some of the autoimmune and inflammatory conditions that have been associated with EPC include anti-NMDA receptor encephalitis, Rasmussen’s encephalitis, and demyelinating disorders like multiple sclerosis.19 Anti-NMDA receptor encephalitis is an autoimmune condition in which the immune system produces antibodies against the NMDA receptors in the brain. Autoimmune etiologies, including anti-NMDA receptor encephalitis, accounted for 6% of cases of EPC.19 The LGI1 antibodies can be also associated with EPC due to limbic encephalitis. It can present with focal face-arm-leg seizures or faciobrachial dystonic seizures.20 Rasmussen’s encephalitis is a rare inflammatory condition that affects one hemisphere of the brain, leading to cognitive decline, motor deficits, and seizures. The EPC can be a presenting symptom of autoimmune encephalitis, and it may be refractory to medical treatment. Different seizure pattern has been described like focal motor seizures without impaired awareness, secondarily generalized tonic-clonic seizures, and focal motor seizures with impaired awareness. It occurs mainly in children and is rarely reported in adults.11 Subacute sclerosing panencephalitis (SSPE) is a rare form of progressive epileptic encephalopathy that can present with EPC. It develops several years after the initial measles infection and is more common in unvaccinated individuals and children who contracted measles before the age of 2 years. Multiple sclerosis is a chronic autoimmune condition that affects the central nervous system, leading to inflammation, demyelination, and axonal damage. EPC can be a rare manifestation of multiple sclerosis, and it can present with intractable focal seizures.21 Anti-myelin oligodendrocyte glycoprotein (MOG) antibodies also can present with cerebral demyelination with EPC. Other autoimmune antibodies like antineuronal nuclear autoantibody type 1/anti-Hu (ANNA-1/anti-Hu) have been reported.22 Another etiology of EPC can be metabolic disorders. Amino acids, organic acids, and neurotransmitter disorders can present with EPC. Mitochondrial diseases, inborn errors of metabolism, and urea cycle disorders are also among the reported cases. Metabolic disorders can represent 10-12% of cases of EPC. For example, non-ketotic hyperglycemia (NKH) and Alpers disease have been reported to present with prolonged focal seizures. Among the metabolic disorders, mitochondrial diseases were the most common cause of EPC, followed by inborn errors of metabolism such as maple syrup urine disease and propionic acidemia.23 Mitochondrial diseases like mitochondrial encephalomyopathy, lactic acidosis and stroke-like episodes (MELAS), Leigh syndrome, and myoclonic epilepsy with ragged red fibers (MERRF) can cause EPC.23 In our region, metabolic and neurogenetic causes are important etiologies for EPC. Neuronal ceroid lipofuscinosis, POLG-related mitochondrial disease and Menkes have been reported in EPC cases in Saudi Arabia.24,25 An increasing literature in the past decade found genetic causes to be associated with EPC. Several genetic mutations have been associated with EPC, including mutations in the KCNA2 and SCN1A genes. KCNA2 mutations are a rare cause of EPC, and they typically present with continuous focal motor seizures affecting one limb. Genetic causes accounted for around 5% of cases of EPC. The SCN1A mutations are another genetic cause of EPC, and they are typically associated with a more severe form of epilepsy, such as Dravet syndrome. It can present with prolonged, fever-provoked, EPC in some cases (Figure 1).26

- Some of the genetic causes reported to be associated with EPC.
- Reported etiologies of EPC.
Investigations
The clinical approach to EPC depends on multiple factors. The age of presentation, progression pattern, preceding history of fever or trauma, travel history, consanguinity, cognitive changes, systemic symptoms, and medication history are important factors to be considered in the evaluation. Table 2 summarizes the investigations of EPC.
- The EPC investigations.
Treatment options for epilepsia partialis continua
The management of EPC can be challenging. Upon presentation with EPC, the initial treatment with a benzodiazepine should be considered to break the cycle of focal seizures. Further escalation of medications according to status epilepticus guidelines is advised. Many patients continue to have focal seizures despite early aggressive treatment with ASMs. Some patients were reported to continue to have EPC for weeks and months.27 Treatment for EPC generally can involve antiseizure medications (ASMs), immunotherapy, and, in some cases, surgery (Table 3). The specific treatment plan will depend on the underlying cause of the seizures and the severity of symptoms. Antiseizure medications (ASMs) are the mainstay of treatment for EPC. Commonly used ASMs include carbamazepine, phenytoin, valproate, levetiracetam, and topiramate. Also oxcarbazepine, lacosamide, perampanel and lamotrigine have been effective is some cases.28 Multiple ASMs may be used in combination to control seizures. Failure of multiple ASMs is not uncommon in treating individuals with EPC.14 Immunomodulatory therapy: Treatment with immunomodulatory therapy should be considered after failure of initial ASMs or if the clinical presentation is in keeping with an autoimmune condition like positive autoantibodies or a clinical picture suggestive of Rasmussen`s encephalitis. Commonly used immunomodulatory treatments in EPC are corticosteroids, intravenous immunoglobulin (IVIG), or plasmapheresis.14 Resistant cases of EPC, especially due to presumed autoimmune etiologies could also benefit from other non-conventional immunomodulatory agents. There is a growing medical literature supporting the use of rituximab as an anti-CD20 monoclonal antibody targeting B cells. Also, inhibitors of purine synthesis like mycophenolate mofetil and azathioprine has been reported.28 Anakinra, an IL-1 inhibitor was reported in a case of EPC due to Rasmussen’s encephalitis.29
- Epilepsia partialis continua treatment.
Surgery
Effective treatment for EPC will depend on the underlying cause and the individual patient’s response to therapy. In some cases, surgery may be the most effective option for achieving seizure control. It is essential to develop a personalized treatment plan based on the specific etiology and clinical course of EPC in each case.30 In cases with drug-resistant progressive focal seizures, progressive weakness of the right or left body, hemispheric atrophy on the MRI brain, and cognitive decline, hemispherectomy is the recommended surgical option, especially in younger individuals with a success rate in controlling seizures up to 80%.31 In rare cases, EPC can be caused by metabolic disorders such as NKH. Dietary modification, such as the restriction of glycine and the use of sodium Benzoate and dextromethorphan can be considered. In some cases, surgical intervention, such as liver transplantation or bone marrow transplantation, may also be necessary to treat the underlying metabolic disorder.30,31
Conclusion
Overall, EPC is a rare but potentially debilitating form of epilepsy that requires expert diagnosis and treatment to manage its symptoms and underlying causes. Despite this progress, EPC remains a challenging condition to diagnose and manage, and further research is needed to develop more effective therapies for patients with this condition.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.