


Abstract
Objectives: To review the patients operated by endoscopic transphenoidal approach for skull base lesions. All the clinical data including age, gender, type of pathology, surgical outcome and surgical complications were studied.
Methods: A clinical prospective study was conducted on 94 cases with skull base lesion that were treated in Neuroscience Hospital in Baghdad, Iraq between October 2011 and December 2016. We followed each patient for an average of 2 years after surgery to determine most common lesion involving the skull base, age and gender distribution, surgical outcome, complications and hospital accommodation. Freeze system of Storz all the cases in the study.
Result: The majority of our patients were between the ages of 20-29 years. Among the 94 patients, 67% had macro adenomas, followed by craniopharyngioma 11%. The mortality rate was 2.1%, Gross total removal was 57.4%. All patients show improvement of the headache after surgery, visual improvement was noticed in 73.4% and hospital accommodation was 2-5 days. Three patients developed cerebrospinal fluid leak, Infection meningitis developed in 3 patients 3.1%, and 2 patients (2.1%) suffered from hormonal disorders and were referred to endocrinologist for therapy. Diabetes insipidus developed as a temporary complication in 4 cases (4.2%).
Conclusion: Trassphenoidal surgery is relatively safe surgery for properly selected patients.
The earliest transsphenoidal surgery was described in 1901 by Schloffer, Von Eiselsberg, and Kocher.1 This surgery required external rhinotomy incisions. The endonasal and sublabial approaches were introduced in 1910 by Hirsch and Halstead, respectively.1 One of the most important advantages of transsphenoidal surgery is its favourable visualization of the anatomical structures. As transsphenoidal surgery evolved, technical advances improved the surgical view of the operative field and the orientation.2 For a century, the transsphenoidal approach was primarily used to resect pituitary and other sellar tumours. However, the endoscopic endonasal transsphenoidal approach has since been proposed as a minimally invasive surgical modality for treating pathologies of the sellar region.3 Recently, standard endoscopic endonasal procedures have extended to provide access to para-sellar lesions. This technical expansion offers significant potential for resecting skull base lesions.4-6 The sphenoidal sinus is the gateway to the skull base. The endoscopic transsphenoidal approach, combined with extended approaches, will provide access to the whole midline skull base, from the Crista Galli to the craniocervical junction.7 At present, the bi-portal four-handed technique (cusimano & fenton 1996) is the standard method used nowadays for trans nasal endoscopic surgery for skull base lesions.8,9 The objective of the study is to review the patients operated by endoscopic transphenoidal approach for skull base lesions. All the clinical data including age, gender, type of pathology, surgical outcome and surgical complications were studied.
Methods
This study was conducted from October 2011 to December 2016 in the Neuroscience Hospital, Baghdad. Approval from the Hospital Ethics Committee was issued for conducting this study. A total of 94 patients (51 females and 43 males) were included, and each patient was followed for an average of 2 years after surgery. The standard approach was used for lesions involving the sella, para sella and suprasellar region. The extended approach was used for lesions in the anterior (frontal) cranial fossa, petrous apex, clivus and foramen magnum. The freeze system of Storz was used in all patients.
General and neurological examination, blood tests, electrocardiogram, echo study, chest X-ray, brain CT-scan and MRI were performed for all patients. Preoperative endocrine profile and visual field assessment were also carried out. All cases underwent operations under general anaesthesia; lumbar puncture injection with a fluorescent dye was used in cases of CSF rhinorrhoea. After the operation, we measured the electrolytes, fluid balance, and hormones; when necessary, we provided replacement therapy. Antibiotics were provided to all patients and anti-epileptics (carbamazepine) were given to some patients. Consent for inclusion in the study was obtained from the patients and their families.
Excel software used for the data analysis. All patients with large tumors that necessitate combined trans nasal and cranial approach simultaneously were excluded from the study.
Results
The median follow-up period was 2 years. The extent of surgical removal was evaluated from postoperative MRI scans obtained 3 months later. There was more females in our study (n=51; 54%) than males (n=43; 46%), because the majority of our cases had pituitary macroadenoma, which is more common in females. Most patients were 20-29 years of age (45 patients).
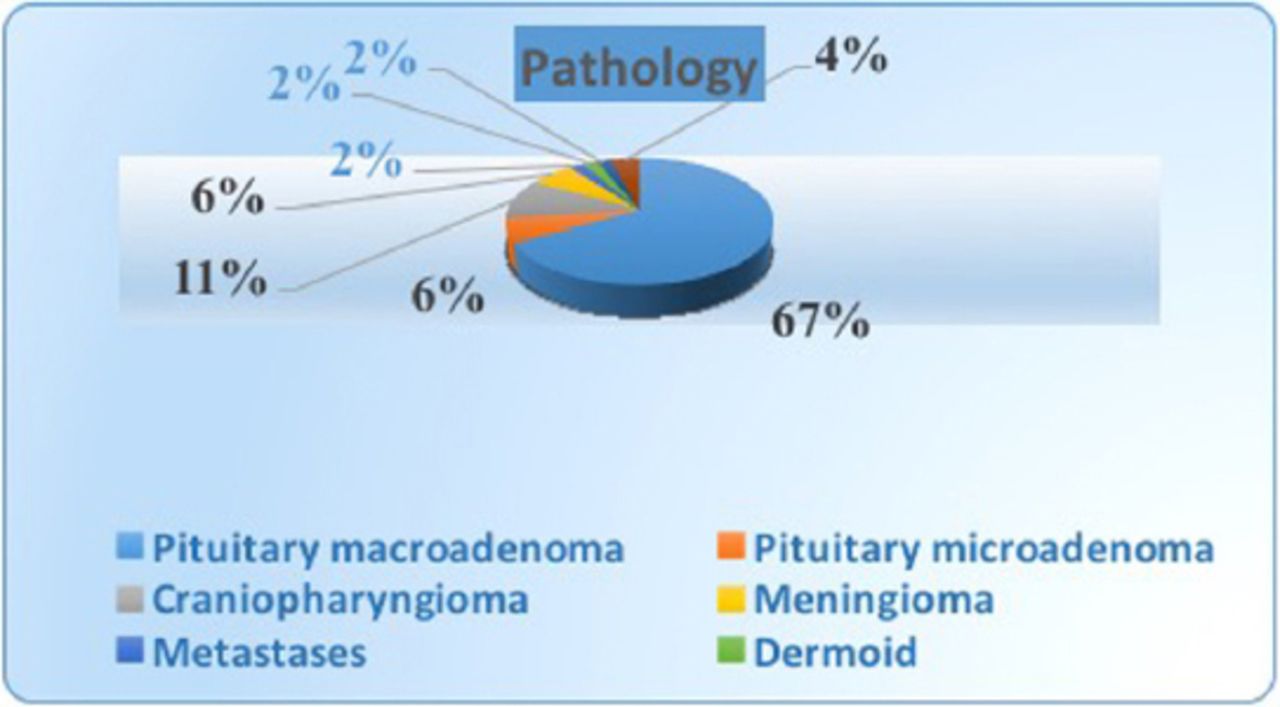
The most frequent tumour was pituitary macroadenoma (67%), which was followed by craniopharyngioma (11%) (Figure 1). The majority of macroadenoma cases were females complaining of hormonal disorder and infertility, which accounts for the predominant age being between 20-29 years. Re-operation was needed because of tumor recurrence in 5 patients (5.3%); 3 patients had a pituitary macroadenoma, one a meningioma, and one a craniopharyngioma.
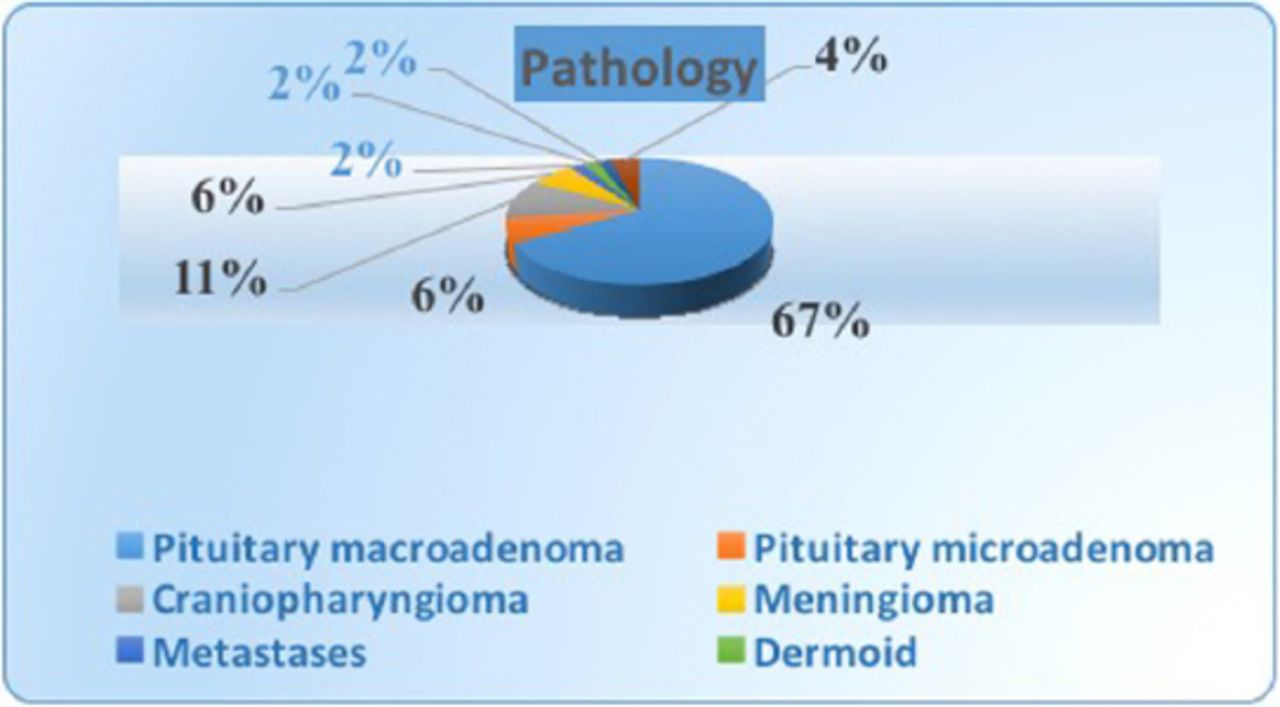
Pathological lesions operated.
Surgical outcome
Gross total tumour removal was achievable in 54 patients (57.4%) (Table 1). Headache symptoms improved in all cases. Visual field improvement was reported in 69 cases (73.4%); most of these cases had pituitary macroadenomas. Intraoperative bleeding from the cavernous sinus occurred in 3 cases, and it was controlled with the use of gentle pressure and surgery.
Surgical outcome. N=94
The CSF leak developed one week postoperatively in 3 patients. All of these patients had macroadenomas; one patient required surgical intervention and the other improved with conservative treatment. Meningitis occurred in three patients; one patient died because he presented in the late stage, while the other 2 had a good response to medication.
Diabetes insipidus temporarily developed in 4 patients; 3 of them had macroadenomas, and one patient had a craniopharyngioma. Desmopressin was given to those patients. Hormonal replacement therapy was needed in 2 patients. They were referred to an endocrinologist. Mortality occurred in 2 patients. One did not recover from anaesthesia, and the other developed meningitis 2 weeks after surgery. The latter case did not respond to medications.
Discussion
In recent decades, endoscopic endonasal trans-spheroidal surgery has become the most popular choice for neurosurgeons and otolaryngologists to treat lesions of the skull base. This is because of minimal invasiveness, a lower incidence of complications, and lower morbidity and mortality rates compared to the traditional approaches.10
In our research on 94 patients who underwent surgery, total gross removal of the tumour was noticed in 52% of the cases. In a study performed by Ensenet J11 on 40 cases, total removal was achieved in 75% of the cases. In another study performed by Shigetoshi Yano et al12 of 74 cases, total gross removal was achieved in pituitary adenomas and in 68% of meningiomas.13
Macro-adenoma was noted in 67% of cases in our study, which is comparable to studies in which 70% of their cases were macroadenomas.11,12 Visual function improvement was achieved in 82% of patients in this study, and this improvement was nearly the same as in other studies in which 90% of cases showed visual improvement after surgery.12,13 In both studies, the majority of cases that developed better visual results complained of pituitary macroadenomas.
The CSF leaks occurred in three cases (3.1%). In a study performed by Shi Ge Toshi et al,14 9.5% developed a CSF leak.14 In a study performed in a brain tumour centre (John Wayne Cancer Institute USA), 6 out of 102 patients (5.8%) developed a CSF leak.12 This variation in the percentage from one study to another is related to the tumour type and size. Larger tumors are more likely to have a CSF leak. The pituitary macroadenoma is the most frequent tumor type to have a post-operative CSF leak.14-16 This finding is similar to the result found in our study in which all cases that had a CSF leak complained of pituitary macroadenomas. The relatively small percentage of patients with a CSF leak in our study is related to the fact that the diaphragmatic sella was not opened unless there was suprasellar extension of the tumor. For these cases, we used 2 double surgical layers with gelfoam to close the defect, and we added an autologous fat graft from the para-umbilical area.
The majority of our patients were between the age of 20-29 years. In a study of 152 patients performed by Tumal Chowdhur, Hemanshu et al,16 the median age was 38 years. In that study, there was a predominance of males in all age groups;16 in this study, 54% of patients were females, and the majority of them were complaining of infertility due to macroadenoma.
The hospital stay was 2-5 days in our study, which was similar to other studies.17 Meningitis developed in 3 patients (3.1%), and other studies reported an incidence of meningitis was of between 0.7-1%,18,19
Such as in a study performed by Cappabianca P et al20 and a study by Dehdashti AR,21 Ganna et al20 in which 200 cases underwent endonasal endoscopic surgery. A high complication rate of meningitis has been reported for craniopharyngioma, while 2 cases in our study had a macroadenoma and one a craniopharyngioma.
Hormonal disorder developed in 2 of our patients (2.1%), requiring therapy, and the rate of diabetes insipidus was 4.2%. A study performed on 444 cases by Fatemi et al22 reported on 75% of cases with pituitary macroadenomas; there was anterior loss in 5% and permanent diabetes insipidus in 2.1%, as well as 2 patients who had total hypophysectomy.
After transsphenoidal adenomectomy, new unplanned hypopituitarism occurs in approximately 5% of patients, while improved hormonal function occurs in 50% of patients. The likelihood of new hormonal loss or recovery appears to depend on several factors. New hypopituitarism most commonly occurs in patients with tumors larger than 20 mm in size, while hormonal recovery is most likely to occur in younger patients without hypertension and in those without an intraoperative cerebrospinal fluid leak.23-25
In conclusion, the trans-spheroidal endoscopic approach from skull base tumors has become a well-established method for treating skull base lesions. However, this approach is technically demanding and requires significant practice. The major factors that predict the success of the trans-spheroidal endoscopic approach are appropriate patient selection along with good pre- and post-operative specialized care.
Acknowledgment
The authors gratefully acknowledge T. Ghiasvan and N. Shabab for their technical assistance.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received May 5, 2017.
- Accepted October 13, 2017.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.