


Notice: Authors are encouraged to submit clinical images for possible publication in the Journal. These may be in any field of Clinical Neurosciences, and should approximately follow the format used here. Please address any submissions to the Assistant Editor, Neurosciences Journal, Prince Sultan Military Medical City, PO Box 7897, Riyadh 11159, Kingdom of Saudi Arabia. E-mail: malaskar{at}psmmc.med.sa
Artery of Adamkiewicz supplying metastatic renal cell carcinoma of the thoracic spine
Clinical Presentation
A 51-year-old man with hypertension and hyperlipidemia was found to have a left-sided renal mass during a workup for new-onset hematuria. A radical left side nephrectomy was performed successfully. Pathologic analysis revealed clear cell renal carcinoma with focal rhabdoid features. No metastases were noted at the time. Eight months after initial presentation, the patient developed progressive back pain. He was neurologically intact and asymptomatic. Metastatic workup showed lesions in the lungs, pleura, ribs, and thoracic T11 vertebral body. The T11 metastasis was associated with a pathologic fracture and central height loss causing posterior cortical bowing and severe spinal stenosis (Figure 1). A spinal angiogram with embolization of the lesion was planned, followed by open surgical circumferential decompression and stabilization. The spinal angiogram showed that the tumor was exclusively derived from the T11 intercostal artery pedicle, via many small racemose feeding vessels. However, the artery of Adamkiewicz (AKA) origin was also found to arise from this pedicle (Figure 2). It was determined that embolizing the tumor would also risk occluding the AKA. Embolization was thus not undertaken. Instead, the patient was treated with circumferential surgical decompression and posterior fusion.
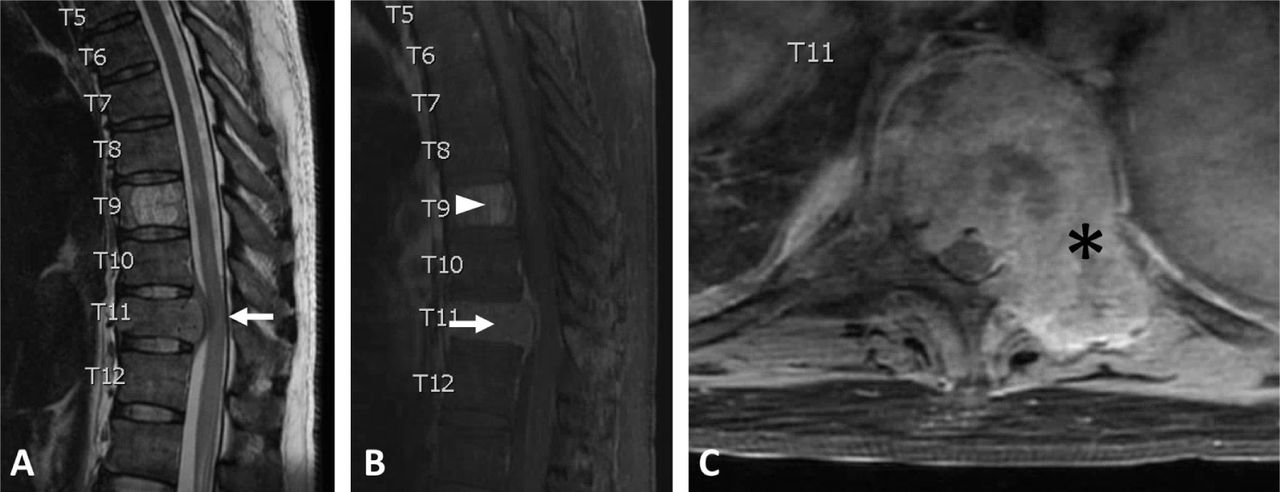
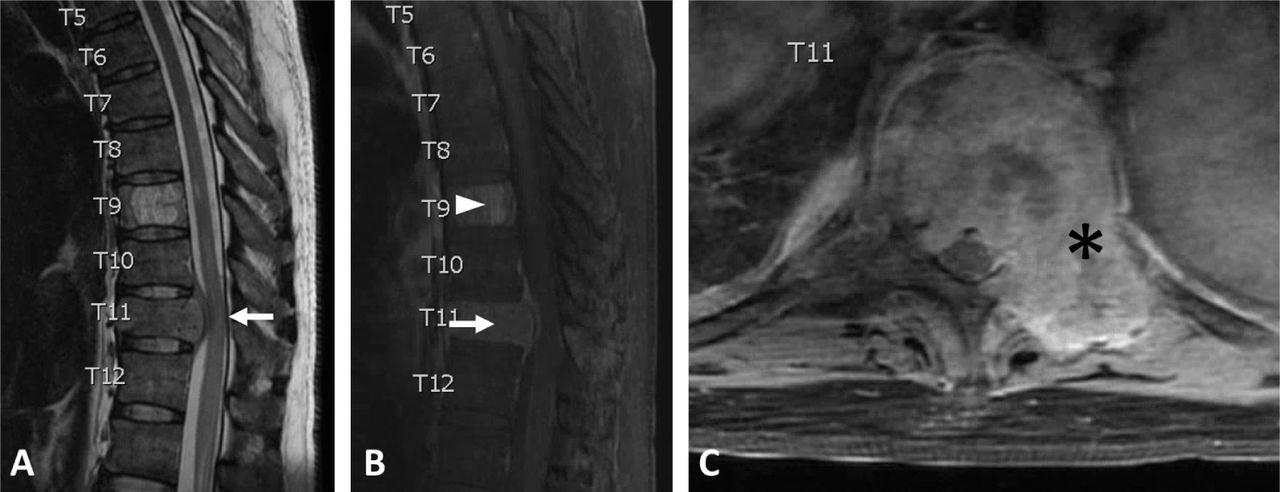
Thoracic spine MRI showing osseous metastasis of T11. A) T2-weighted sagittal image showing height loss and posterior cortical bowing of the vertebral body causing severe spinal canal stenosis with cord compression (white arrow). B, C)T1-weighted contrast-enhanced sagittal and axial images showing involvement of the entire T11 vertebral body (white arrow) extending into ventral epidural space as well as the left T11 pedicle, posterior bony elements, costovertebral junction, proximal left rib, and paraspinal muscles (black asterisk). An incidental T9 vertebral body hemangioma (white arrowhead) is also noted.

Microcatheter (white arrow) in the descending aorta, with selective catherization of the left T11 intercostal artery pedicle showing prominent blush of tumor vasculature (white arrowhead) via multiple small proximal racemose feeders. The artery of Adamkiewicz (black arrows) arises distally and ascends approximately two vertebral levels before making a hairpin turn and descending in the midline. The continuation of the left intercostal artery (black arrowhead) is also noted.
Questions:
1. What is the primary arterial blood supply to the thoracolumbar spinal cord?
2. Where does the AKA most commonly originate?
3. What is the importance of circumferential surgical decompression of the spinal cord in the setting of metastatic lesions?
4. What are the risks of preoperative embolization of spinal metastases?
5. Should embolization be attempted if the AKA origin is at the same level of the tumor?
Answers & Discussion
1. The arterial blood supply to the spine comprises a complex network of vessels with considerable variability and extensive anastomoses. At each spinal level from T4 to the sacrum, paired segmental spinal arteries arise directly from the aorta. As they course posteriorly, the segmental arteries typically give rise to vessels supplying the vertebral bodies and bones of the spine (via the pretransverse/paravertebral arterial system); the rib cage (via the intercostal arteries); and the neural elements, including bony and soft tissue posterior to the transverse processes (via the dorsal spinal arteries).
The dorsal spinal artery splits into many small branches, most notably a radicular branch that penetrates the nerve root sheath and further subdivides into anterior and posterior branches. The anterior (radiculomedullary) branches contribute to the anterior spinal artery (ASA), while the posterior (radiculopial) branches contribute to the paired posterior spinal arteries (PSAs). The ASA supplies the anterior aspect of the cord, which includes the corticospinal and spinothalamic tracts. The PSAs supply the posterior aspect of the cord, most notably the dorsal columns. At their origins in the cervical spine, the ASA and PSAs typically arise from fused spinal branches of the vertebral arteries and inferior thyroid arteries. As they descend, the vessels are joined by the radiculomedullary and radiculopial branches to continue supplying the thoracic and lumbar cord. The ASA and PSAs terminate in an anastomotic ‘basket’ under the conus medullaris.
Of note, the aforementioned major arteries and their branches extending down to the cord surface comprise the angiographically visible macro-circulation; the deeper branches within the cord substance are known as the micro-circulation and are not typically visible even in high-resolution angiograms.
2. The AKA, or great anterior radiculomedullary artery, typically originates from posterior intercostal arteries and ascends several levels into the subarachnoid space of the ventral cord. It then makes a characteristic inferior hairpin turn to join the ASA at the midline spinal cord surface and supply the cord from the mid/lower thoracic region until the conus medullaris. Localization of the AKA before surgical and interventional radiologic procedures involving the thoracic and lumbar spine is imperative to reduce the risk of spinal ischemia and paraplegia; indeed, iatrogenic causes remain the most frequent cause of injury to the AKA.1 The AKA is present in approximately 85% of the population, predominantly as a single vessel (87.4%) on the left side of the body (76.6%), originating between T8 and L1 (89%) but most frequently originating at the level of T9. Detection of the AKA is difficult due to its small diameter (average 1.09 mm), variable levels of origin, and extensive anastomoses.1 Thus, complete visualization of the AKA course requires catheterization of vessels from the mid-thoracic down to the lumbar region. Digital subtraction angiography remains the gold standard to identify the presence of the AKA and its characteristic hairpin loop when joining the anterior spinal artery.
3. Metastatic spread of cancer to the spine is a common finding at the initial diagnosis of renal cell carcinomas (RCC) as well as other common diseases such as breast, lung, and prostate malignancies. Compression of the spinal cord and cauda equina is a major cause of morbidity in these patients. The RCC is the most common cancer to cause neurologic deficit due to an undetected primary malignancy, often due to metastasis to the thoracic spine.2 Due to the high incidence of radiation failure in RCC, treatment of metastatic lesions often involves surgical resection followed by immunotherapy. Surgical treatment of extradural spinal metastases is guided by established criteria that incorporate mechanical stability, radiographic features, neurological deficit, and symptoms such as pain. Aggressive circumferential decompression and multilevel stabilization is associated with good neurological and oncologic outcomes, but carries the risks attendant with larger surgeries in a morbid patient population.3
4. Up to 33% of patients undergoing surgery for spinal metastases of kidney cancer may experience excessive blood loss requiring large volume transfusions, due to the hypervascular nature of these lesions. Preoperative embolization has been shown to reduce adverse effects of blood loss such as hypotension and anemia, as well as transfusion-related complications. Risks of embolization include abscess formation, embolization particle reflux, and off-target embolization causing spinal cord ischemia.4
5. Embolization of tumor pedicles in proximity to the AKA remains technically challenging and controversial. One retrospective study found that there was no statistically significant association between spinal levels of hypervascular tumors and radiculomedullary arteries, such as the AKA. The same study found that embolization of tumor feeder arteries at the same level of the AKA is possible if the origin is distal to the origin of the AKA.5 This should only be attempted after super selective catheterization of distal tumor feeder vessels, and even then, there is still a risk of embolization particle reflux into the AKA. If the tumor feeder origin is proximal to the origin of the AKA, then embolization is contraindicated due to the risk of spinal cord stroke. In the case presented here, preoperative embolization was deemed unsafe due to the concomitant and distal origin of the AKA to the tumor feeders at the T11 vertebral level.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.