


Abstract
Objective: To evaluate the role of posterior fixation including the fractured vertebra (PFFV) for the treatment of thoracolumbar vertebral fractures.
Methods: Sixty-seven patients that sustained a single-level thoracolumbar fracture were included in this retrospective study carried out in the Wuxi People’s Hospital, Wuxi, China between August 2010 and June 2013. Thirty-two cases were treated with PFFV, and 35 cases were treated with traditional short-segment fixation (TSSF). All patients were periodically followed-up with clinical and radiologic evaluation. Cobb’s angle and vertebral body height were analyzed and compared, and the operational time, intra-operational blood loss, and the Denis pain scale scores were also compared.
Results: Compared with preoperative angles, the Cobb’s angles were reduced and the vertebral body height of the fractured vertebra was increased after operation at a statistically significant level. Twelve months post-operative, the loss of Cobb’s angle and vertebral body height in the PFFV group was significantly less than that in the TSSF group. There was no statistical significance in the Denis pain scale score 12 months post-operatively between the 2 groups.
Conclusion: Selective adoption of PFFV is helpful not only for stabilization of fractures and restoration of anatomy, but also maintaining the effectiveness of the restoration with good functional outcome.
Thoracolumbar fractures are among the most common type of traumatic spine fractures. Surgical treatment is necessary if stability or neurological function is impaired.1 Restoration of the vertebral column stability and decompression of the spinal canal are the main goals of surgical treatment.2 Posterior short-segment fixation has the advantage of using a less extensive approach with less blood loss and complications without compromising the quality of stabilization, and spares healthy mobile segments in fusion, and thus preserves mobility.3 Traditional short-segment fixation (TSSF) is a widely used technique in the treatment of unstable thoracolumbar fractures. It not only provides distraction and compression forces that facilitate 3-dimensional correction and firm fixation, but it also preserves motion segments.4 It can offer several advantages: immediate stability, restoration of the vertebral height and deformity angle, and prevention of late neurological injury.5 However, TSSF has been associated with a high rate of failure.6 The latter is usually associated with implant failure and loss of reduction of kyphosis. Posterior fixation including the fractured vertebra (PFFV) is a novel idea used to overcome the shortcomings of TSSF. The technique avoids the suspension effect and quadrilateral effect, dispensing the internal fixing load and reducing the correction degree losses and internal fixation fractures, and it shows good efficacy in clinical application.7 However, there are still only a few randomized controlled studies7 and the relevant theory requires further investigation. The purpose of this study is to compare the clinical effectiveness of PFFV and TSSF in the treatment of thoracolumbar fracture.
Methods
This retrospective study was conducted in Wuxi People’s Hospital affiliated to Nanjing Medical University, Wuxi, China between August 2010 and June 2013. The study included 32 patients, (20 males and 12 females), with an average age of 43.6 years (range 25-63) who underwent PFFV, and 35 patients, (24 males and 11 females), with an average age of 45.8 years (range 23-62) who underwent PFFV. All patients had a single level traumatic A3.1 and A3.2 fracture of thoracolumbar spine. Inclusion criteria were: single-level A3.1 and A3.2 fracture, age range between 18 and 65 years, no neurological involvement, and fracture level between T11 and L5. Exclusion criteria were: pathological or osteoporotic fracture, multilevel fracture, and previous surgery at site of fracture.
Our institutional review board approved the study, and written informed consent was obtained from each patient. All the patients received frontal and lateral x-ray imaging (Siemens Healthcare, Bavaria, Munich, Germany) to learn the type of fracture and the height of the Cobb angle and vertebral anterior edge. Computed tomography scans (Siemens, Bavaria, Munich, Germany) were conducted to ensure that the pedicle of at least one side of the fractured vertebra was intact. If feasible, the patients underwent an MRI to obtain the compression condition of the spinal cord, and the injury condition of the anterior and posterior longitudinal ligaments and the intervertebral disc.
Surgical procedure
The approach was midline posterior in all patients. Pedicle screws were used bilaterally. For the TSSF, pedicle screws were placed at one level above and below the fracture site. For the PFFV, additionally, pedicle screws were inserted at the level of the fracture. After performing successful screws placement, indirect reduction was achieved by inserting a contoured rod. The reduction procedure included the following steps: correction of kyphosis, lordotic distraction for further reduction of the vertebral height and intra-canal fragment, and rigid locking of all the nuts. The same surgeon removed the pedicle screws after 12 - 18 months.
All patients were periodically followed-up with clinical and radiologic evaluation. Contrast analysis was performed on Cobb’s angle changes, and vertebral body height in postoperative week one, and at one, 3, 6, and 12 months. The vertebral body height was determined by the ratio of the mean of the fractured vertebral body and anterior heights of the adjacent 2 vertebral bodies. The Cobb’s angle was determined by the angle formed by the perpendiculars of the extension lines of the upper endplate of the upper fractured vertebra and the lower endplate of the lower fractured vertebra.
Statistical analysis
The Statistical Package for Social Sciences, version 16.0 (SPSS Inc., Chicago, IL, USA) was used for statistical analysis. We compared the following parameters: the Cobb angle, and the vertebral body height treated with either TSSF or PFFV. The comparisons included the data compiled at the preoperative and postoperative stages. Clinical parameters were also compared during the one-year follow-up period. In addition, blood loss and operation time were compared. Student’s t test was used for statistical analyses; and p-values <0.05 were considered to be statistically significant.
Results
There were no statistical differences between the 2 groups for age, gender, fractured segment, fracture type, preoperative Denis pain scale scores, and kyphotic angle. No patient in either group experienced neurologic system exacerbation or died. Excessive wound exudation was found in one patient in the PFFV group and was healed by re-debridement, drainage, and pressure bandaging. Incision infection in superficial skin occurred in one patient in the TSSF group and was resolved by dressing change. No deep infection was found in either group. All of the patients acquired significant pain relief in their lower back.
The average operation duration was 115.68±12.83 minutes (93-136) in the PFFV group versus 93.08±10.98 (75-116) in the TSSF group, and there was significant difference between the 2 groups in the duration of the operation (p=0.021). The average blood loss was: 229.06±28.32 ml (185-265) in PFFV group versus 218.88±20.39 (180-250) in TSSF group; there was no significant difference in blood loss (Table 1). In the PFFV group, the preoperative Cobb’s angle improved from 19.78±7.31° to 7.06±3.26° after surgery, and there was significant difference (p=0.026). In the TSSF group, the preoperative Cobb’s angle improved from 20.51±6.06° to 8.03±3.61° after surgery, and there was also a significant difference (p=0.039). At the last follow-up of after one year, the loss of correction of the Cobb’s angle in the PFFV group (2.63±1.95°) was significantly less than the TSSF group (5.51±3.28°) (p=0.032) (Figures 1 & 2, Table 2). In the PFFV group, the preoperative vertebral body height improved from 62.69±10.83% to 93.72±6.75% postoperatively, there was significant difference (p=0.016). In the TSSF group, the preoperative vertebral body height significantly improved from 60.57±10.12% to 91.97±8.26% postoperatively (p=0.029). During the last follow-up of after one year, the loss of correction of vertebral body height in the PFFV group (3.78±2.28%) was significantly less than in the TSSF group (8.31±5.33%) (p=0.038) (Figures 1 & 2, Table 2). Up to 12 months post operation, no loose screws were found in the PFFV group, but screw breakage were found in 2 patients in the TSSF group. There was no significant difference in Denis pain scale scores 12 month after operation between the 2 groups (p=0.093) (Table 3).
Comparison of operational duration and blood loss between the 2 groups of Chinese patients treated for a single-level thoraco-lumbar fracture.

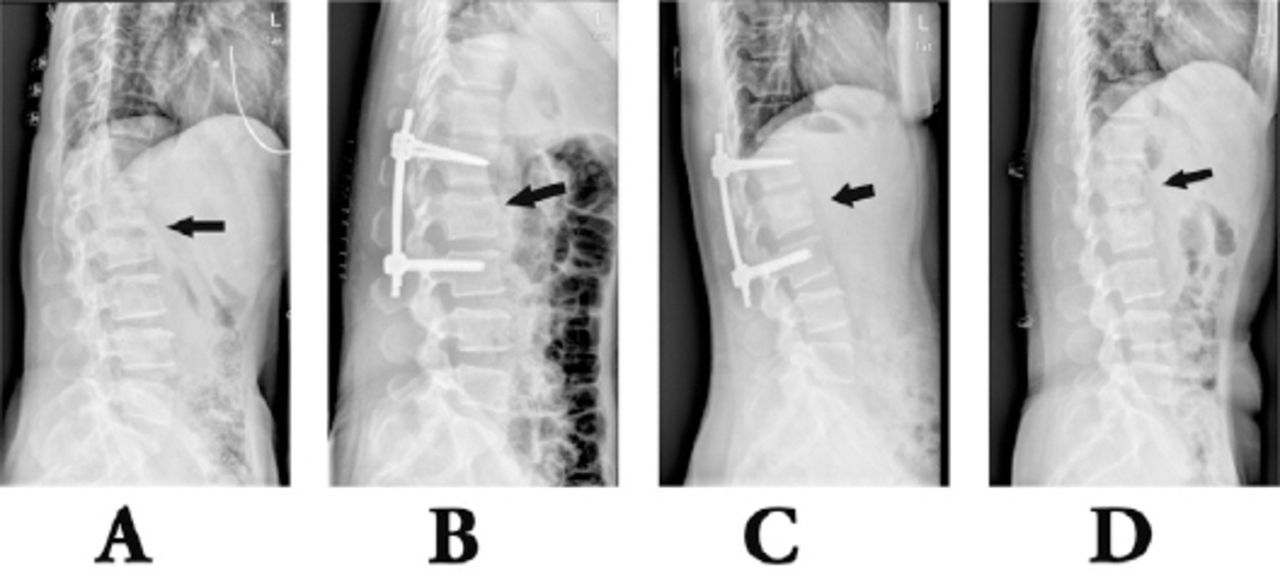
Lateral radiograph of dual-plane fixation of an L2 fracture. A) preoperative; B) one week after operation; C) 3 months after operation; D) one year after operation.

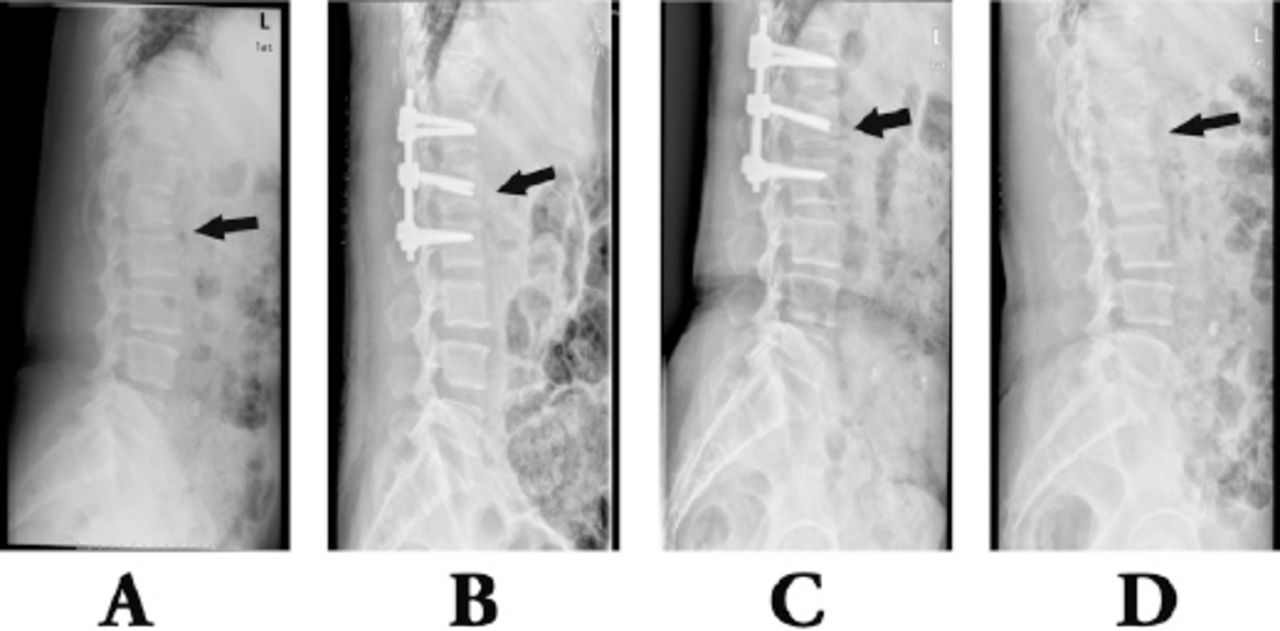
Lateral radiograph of triplane fixation of an L1 fracture. A) preoperative; B) one week after operation; C) 3 months after operation; D) one year after operation.
Comparison of the Cobb angle and vertebral body height between 2 groups of Chinese patients treated for a single-level thoracolumbar fracture (mean±SD).
Comparison between Denis pain scale scores one year postoperation in 2 groups of Chinese patients treated for a single-level thoracolumbar fracture.
Discussion
Traditional short-segment fixation, which involves one vertebra above and one vertebra below the fracture level has become the most common method in the treatment of thoracolumbar burst fractures. It provides the benefit of decreased involvement of motion segments than fixation with longer instrumentation. However, there is still controversy as far as the results of TSSF are concerned. Some studies report a high rate of failure because of proximal screw pullout, screw breakage, and loss of correction even if material failure does not always affect the clinical outcome.6 In addition, TSSF distracts the anterior columns indirectly by distracting the posterior columns, which results in a poor posterior column distraction effect, leading to prolongation of posterior column, and increasing the compressing force in the posterior column, resulting in the failure of internal fixation.8,9
McClain et al10 carried out a prospective study and found that 55% of the patients receiving posterior short-segment TSSF fixation had 10° sagittal collapse during the facture healing period. It was considered that the reason for this complication is that the 4-screw fixation approach is an indirect TSSF inter-joint restoration and fixation procedure, and store the fractured vertebra by anterior and posterior ligaments traction. Vertebra fractures were usually complicated with significant anterior and posterior longitudinal ligaments injuries and intervertebral tears, leading to poor restoring efficacy rates. The reason for these problems might be the following facts: suspension effect: the vertebral anterior edges of adjacent vertebras advanced forward and the fractured vertebra retroceded backward after the TSSF fixation, leading to kyphoplasty and spinal correction degree loss, thereby increasing the internal fixing load and internal fixation failure rate; “quadrilateral effect”: not able to provide 3-point fixation, leading to lateral instability and poor rotation resistance, hampering healing of fracture and restoration of ligaments and vertebral disc; or high internal fixing load: there was a long distance between TSSF fixing screws, leading to high bearing force on the connection rod and screws; in addition, the TSSF fixed spinal cord could not bend and all bending movement was conducted by the screw-rod internal fixing system, which was prone to looseness or fracture of the internal fixing materials. In this study, 35 patients were studied, among which, 3 patients achieved no improvement in fractured vertebra height and poor restoring effect and 2 patients suffered from an internal fixation fracture.
Compared with TSSF, PFFV can provide higher biomechanical stability. Firstly, a fractured screw-setting can exert a pressure stress toward the abdomen on the fractured vertebra, which can resist the “suspension effect”.11 Secondly, this procedure could improve the lateral stability of fixation. In addition, the additional fixation could reduce micro-movements on the bone-metal interface and provide higher screw pullout force.12 Anekstein et al13 carried out a biomechanical experiment on swine lumbar vertebra and demonstrated that the rigidity of the spinal segments along the directions of flexion-extension, lateroflexion, and axial rotation increased significantly when applied with additional fractured vertebra screws. Mahar et al14 found that a fractured vertebra screw-setting can improve the stability of normal TSSF segment fixation and provide additional fixing points to facilitate the fracture restoration and kyphoplasty correction, thus offering significantly better results than the TSSF group. Dick et al15 performed 6-screw and 4-screw fixation in a bovine lumbar vertebra model to compare their biomechanical difference, and they found that the 6-screw method that requires placing pedicle screws in the middle vertebra had obvious advantages: the axial bearing capacity increased by 160%, the bucking resistance increased by 48%, and torsion resistance increased by 38%. Baaj et al16 studied corpse specimens and found that short-segment fixation combined with fractured vertebra screw-setting could significantly improve the fixing stability.
In the present study, vertebral height, and Cobb’s angle were measured and recorded preoperatively and at one week follow-up. Average preoperative vertebral heights were 62.69±10.83% in PFFV and 60.57±10.12% in TSSF, whereas average postoperative vertebral heights were 93.72±6.75% and 91.97±8.26%. Preoperative Cobb’s angles were 19.78±7.31° in PFFV and 20.51±6.06° in TSSF, whereas postoperative Cobb’s angles were 7.06±3.26° and 8.03±3.61°. These changes demonstrated that the 2 methods could effectively restore the anterior column height of the fractured vertebra and correct the kyphoplasty caused by fracture. More importantly, the loss of correction of vertebral height after one year was 3.78±2.28% in PFFV and 8.31±5.33% in TSSF. Loss of correction of Cobb’s angle was 2.63±1.95° in PFFV and 5.51±3.28° in TSSF (Figures 1 & 2, Table 2). The PFFV group had fewer losses in fractured vertebral height and Cobb’s angle than the TSSF group, which indicated that PFFV is able to generate greater stability and avoid the “suspension effect,” and better share the pressure stress from the anterior column.
The Denis pain scale score showed that at the follow-up visit 12 months post-operatively, most patients in both groups occasionally had mild pain in their lower back, with no statistically significant difference (Table 3), suggesting that PFFV would at least not further aggravate the post-operative long-term lower back pain. In addition, the blood loss was 229.06±28.32 (185-265) in the PFFV group and 218.88±20.39 (180-250) in the TSSF group (Table 1), and there was no significant difference. Therefore, additional pedicle screws did not increase the damage of soft tissue.
Although PFFV showed favorable performances in the restoration process, fixing strength, and stability maintenance, the surgical procedure should be strictly controlled. Based on our experience, the applicable indications include a thoracolumbar fracture in a single vertebra of type A or B1, with an intact pedicle on the fracture’s side or both sides and without bursting in the lower part of the vertebra or in the endplate, which should be fitted for fractured vertebra fixation. The decision whether to perform fractured vertebra fixation should be made considering the following factors: intraspinal occupation <50% and vertebra height loss <70%; at least one side of the fractured vertebra’s pedicle is intact; the load dispensing condition in the fractured vertebra; and the integrity of the fibrous ring and posterior longitudinal ligaments. McCormack et al17 thought that the anatomical features of the fracture itself were more important than the category of the fixing materials. The selection of surgical approach for thoracolumbar fracture should be made based on the loading dispensing condition in the vertebra. If the vertebra is poor in load dispensing performance, the failure risk of internal fixation will increase. For bursting fractures, fibrous ring and posterior longitudinal ligaments play a key role in the restoring the fragment. When the 2 are both intact, the PFFV pedicle internal fixation can achieve satisfactory restoration; if only one is intact, the restoration efficacy will be still quite favorable; when both of them are injured, fractured vertebra’s pedicle internal fixation is not recommended.
Using PFFV to treat a thoracolumbar fracture may effectively reduce the secondary losses in post-operative vertebra height and correction degree and reduce the post-operative failure rate of internal fixation. With the increase in the number of screws and fixed segments, the mobility of the flexion-extensional, torsional and lateral bending mobility of fixed segments will be compromised. According to the stress concentration theory proposed by Shono et al,18 the movement range of adjacent segments will increase to compensate, leading to stress concentration; the redundant stress will cause an accelerated degradation of the intervertebral disc between the adjacent segments.19 The PFFV is obviously superior to TSSF; however, it still cannot completely avoid fractured vertebra’s shell-like change, the secondary losses in fractured vertebra’s height and correction degree, or the failure of internal fixation. To cope with the aforementioned problems of PFFV, some scholars recently proposed some new approaches, such as PFFV combined with pedicle’s vertebra grafting, PFFV combined with fractured vertebra’s vertebroplasty, and PFFV single-segment fixation.20,21
In conclusion, compared with TSSF, PFFV can avoid post-operative kyphoplasty correction loss and better maintain the vertebral body height. It is a feasible approach for treating thoracolumbar fractures clinically.
Acknowledgments
The authors thank Dr. Qi-Hua Yin for her help with radiological evaluation.
Footnotes
Disclosure
This study was supported by a grant from Wuxi Hospital Management Center (No. YGZXM1536), Jiangsu, China.
- Received May 7, 2015.
- Accepted July 8, 2015.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.