


ABSTRACT
Objectives: To rank the cognitive tasks commonly used in clinical practices based on their difficulties in healthy adults while walking. Dual tasks have been widely used in clinical settings for different purposes such as detecting early cognitive impairments and identifying fall risk factors among the population of neurological diseases.
Methods: This cross-sectional study, conducted from January to March 2021, included a sample of 26 healthy adults who were asked to demonstrate six different cognitive tasks at random while performing a gait speed test. An accelerometer positioned on the lower back at the umbilical level was used to measure participants’ sway. After each task, participants rated the task’s difficulty using the perceived difficulty scale.
Results: (1) The cognitive tasks showed no significant effect on sway (p> 0.05). (2) A statistically significant effect was observed for the cognitive tasks on perceived difficulty scale rating. (3) Statistically significant correlations were found between the perceived difficulty scale and the acceleration measures.
Conclusion: This study was able to rank the cognitive tasks based on the participants’ perceived difficulty scale. Furthermore, significant correlations were identified between the perceived difficulty and the sway measurements.
Dual-task (DT) describe the ability to perform two-tasks concurrently, however, each task measured independently and having distinct goals.1 The DTs illustrate the interaction between cognitive and motor systems that is essential for everyday activities, such as walking and talking.2 It is important to clarify that the definition of DT is still debated, as is the distinction between DTs and complex single-tasks (ST). Many researchers characterize tasks based on their purposes and functionality; in these cases, the term DT refers to motor-cognitive tasks and the term complex ST refers to motor-motor tasks.1–3
Gait is one of the most important motor tasks included in dual-tasking clinical practice.4,5 Gait disorders commonly occur in neurological disease conditions and elevate the risk of causing disability and falls.6 A large percentage of fall accidents among the elderly happen during ambulation.7 Gait speed is an available and feasible assessment tool that is used to describe the functional capacity, ability, and safety of patients.7,8 The 6-Meter Timed Walk (6MTW) is considered to be an assessment tool for measuring gait speed and has been utilized in clinics.9
Postural sway is used as an assessment tool for balance, indicating and predicting a high risk of falls, and it correlates with the number of falls in patients.10 Additionally, there is a correlation between postural sway and certain clinical balance assessments.11 Therefore, the accelerometer has been used to quantify postural sway for measuring balance purposes during walking by measuring a reference point’s acceleration that is near to the centre of the body’s mass (CoM).12 For instance, the accelerometer was measured using an inertial measurement unit (IMU) placed over the lower part of the back of the studies’ participants, specifically between the third and fifth vertebrae.11 Recently, smartphones have been used to measure accelerometer data through applications, providing a practical solution for lowering costs and demonstrating validity and reliability in assessing postural adjustments and gait in clinical practice.13 Furthermore, the perceived difficulty scale is a modified version that has been developed based on perceived exertion scales for resistance and aerobic exercises.14 The scale ranges from 0 to 10, with lower scores meaning that the exercise was ‘extremely easy’ and higher scores meaning that the exercise was ‘extremely hard’.15 A recent study found a moderate to strong positive correlation between trunk postural sway measurements from accelerometers and perceived difficulty ratings.15 The study recommends using these measurements in rehabilitation programs to help balance exercise intensity and to serve as a tool for measuring progress.15
Based on different cognitive functions and purposes, cognitive tasks have been used in lab-based or clinical assessments, such as visual and auditory Stroop, obstacle avoidance, and visual tasks.2 However, due to limited resources, as well as the time and cost involved, not all dual tasks (DTs) are suitable for clinical use. Therefore, simple cognitive tasks, such as reciting months in reverse order, subtracting serial threes from 100, verbal fluency exercises, spelling five-letter words backward, and engaging in structured conversation through questions and answers, have been adapted from cognitive assessment tools like the Mini-Mental State Examination and are increasingly utilized in clinical settings.2,16 However, there is no evidence within the current studies that ranked the current cognitive tasks based on difficulty.
It is necessary to rank the cognitive tasks based on their complexity and difficulty to help the rehabilitation specialists progress their exercises during the rehabilitation phases. This study aims to compare the difficulty of some of the most used cognitive tasks in rehabilitation clinics during walking among healthy subjects. We hypothesized that there would be 1) a statistically significant effect of the cognitive tasks on sway, 2) a Statistically significant difference between the cognitive tasks based on difficulty on the Perceived difficulty scale, and self-report rated difficulty from the participants, there will be a significant correlation between the perceived difficulty scale and sway.
Methods
Participants
This cross-sectional study was carried out between January and March 2021. The study recruited healthy volunteer participants. The study setting was at Buraydah Central Hospital in Buraydah City. The physiotherapy gym area was the location to conduct the study. Inclusion criteria included healthy adults from both genders who can walk normally without assistive devices. Exclusion criteria included having any neurological deficits or active medical disease, having a surgical intervention in their lower limbs, and wheelchair users or any assistive devices for ambulation. The local research ethics committee, Qassim Province, approved this research (registration No. H-04-Q-001) and followed the Helsinki Declaration.
Dual tasks (DTs)
The DTs involved a combination of a motor task and one of 6 distinct cognitive tasks. The motor task involved a gait speed test, where participants were instructed to walk at a comfortable pace over a 10-meter distance. However, just the intermediate 6 meters were measured, allowing for the first two-meters to allow the acceleration and the last two meters for deceleration. Participants were required to complete three trials to calculate an average speed. The equipment needed for the gait speed test included a measuring tape, sufficient space, and a stopwatch.9 The cognitive tasks were chosen based on the literature review and from experience, the 1st author selected 6 cognitive tasks which have been revised and agreed upon by the 2nd, and 3rd authors. The features of the cognitive tasks that have been selected were that they should be simple and easy to implement in any clinical setting and preferably based on standardized assessment tools. The cognitive tasks were reciting months backwards (Dm), verbal fluency (Df), regular conversation based on questions and answers (DQA), and counting backwards by subtracting three numbers starting from 100 (D100), reverse spelling of five-letter words (Ds). The sixth cognitive task, combines two single-digit numbers and determines if the number is bigger or smaller than 50 (D50).
Procedure
Initially, participants were asked to perform an ST, which was the gait speed test without any cognitive task. The gait speed test demonstrated a straight 10-meter distance that was marked on the ground using tapes. Time was recorded using a stopwatch to time the participants’ walking of the middle 6 meters while allowing for 2 meters at the beginning of the walking for acceleration, and 2 meters at the end for deceleration. The demonstrator informed the participants to walk at a comfortable speed. After that, cognitive tasks were added randomly while performing gait speed. Before starting any DT test, the participants were oriented and instructed about the tasks to be tested. Participants were not directed to prioritize either the cognitive task or the motor task.
Perceived difficulty rating
Participants were requested to rate the difficulty of the cognitive tasks according to their perceived difficulty using the perceived difficulty scale that includes a range of 0 to 10, where 0 means “extremely easy,” 2 means “easy,” 4 means “somewhat easy,” 6 means “somewhat hard,” 8 means “hard,” and 10 means “extremely hard”.15
Sway
Participants’ mediolateral (ML) and anteroposterior (AP) accelerations were measured to determine the trunk postural sway while walking using a built-in accelerometer of a smartphone.13 Acceleration data were sampled using a commercially available application (SensorLog App Version 3.7.1). The rationale for using the smartphone is due to the lack of the recourses, easy to implement, and it was validated and reliable to measure the postural sway.13 The rationale for considering the postural sway as it was clinically used as an assessment tool to assess balance.10 The rationale for using the acceleration as it has been used to quantify the postural sway.12
The smartphone was attached to a custom-made belt via Velcro and placed on the participants’ lower back at the lumber 3-4 vertebrae level, as it was mostly placed within the current evidence.12 The accelerometer measured in units of G (9.81 m/s²) with a sampling rate of 100 Hz. The acceleration was recorded for 15 seconds;17 the intermediate 10 seconds were used for analysis, allowing 2.5 seconds at the beginning and 2.5 seconds at the end for acceleration and deceleration.
Data analysis
Row acceleration data were analyzed by conducting the MATLAB program (MATLAB version: 9.13.0 (R2022b). Acceleration data were filtered using a second-order Butterworth low-pass filter with a cut-off frequency of 2 Hz. Following that, data was plotted for visual inspection.
The Root Mean Square (RMS) of acceleration was computed for the ML and the AP directions of sway separately (equation 1). Additionally, the acceleration Normalized Path Length (NPL) acceleration was computed for the ML and the AP directions of sway separately (equation 2).
Equation 1: Root Mean Square
 (1)
(1)N=number of sway samples
Sway [n]: individual sway sample – mean of all sway samples
Equation 2: The Normalized Path Length (NPL) of acceleration
 (2)
(2)N = number of sway samples
Sway [n]: individual sway sample – mean of all sway samples
Statistical analysis
The Statistical Package for Social Sciences, IBM SPSS version 24 (SPSS Inc., Chicago, IL, USA) was used to perform all statistical analyses. The Shapiro-Wilk test was used to assess the normality of the data. Demographic characteristics were reported using means and standard deviations. The subjects’ sway was compared using one-way repeated measures ANOVA, sphericity assumption was tested using Mauchly’s test and the Greenhouse-Geisser correction was applied to adjust the degree of freedom when the assumption was violated. Perceived difficulty rating was compared by the use of the Friedman test with a post-hoc analysis using the Holm-Bonferroni test. Correlations between perceived difficulty scale measures and acceleration measures were calculated using Spearman’s rank-order correlation. Sample size determination was based on data from a previously published work.17 The sample size was estimated using the G*Power program with a Cohen’s d of 0.53 determining that 26 subjects were needed. Sphericity assumption was tested using Mauchly’s test and the Greenhouse-Geisser correction was applied to adjust the degree of freedom when the sphericity assumption was violated.
Results
Twenty-six healthy adult individuals (13 male and 13 female) with ages ranging between 18-49 years (M=29.4, SD 7.5 years) participated in the study (Figure 1) (Table 1).

- Flow chart of participants’ enrolment.
- Participant’s demographic characteristics.
- One-way repeated measures (within-subjects) ANOVA of sway measures.
Perceived difficulty scale
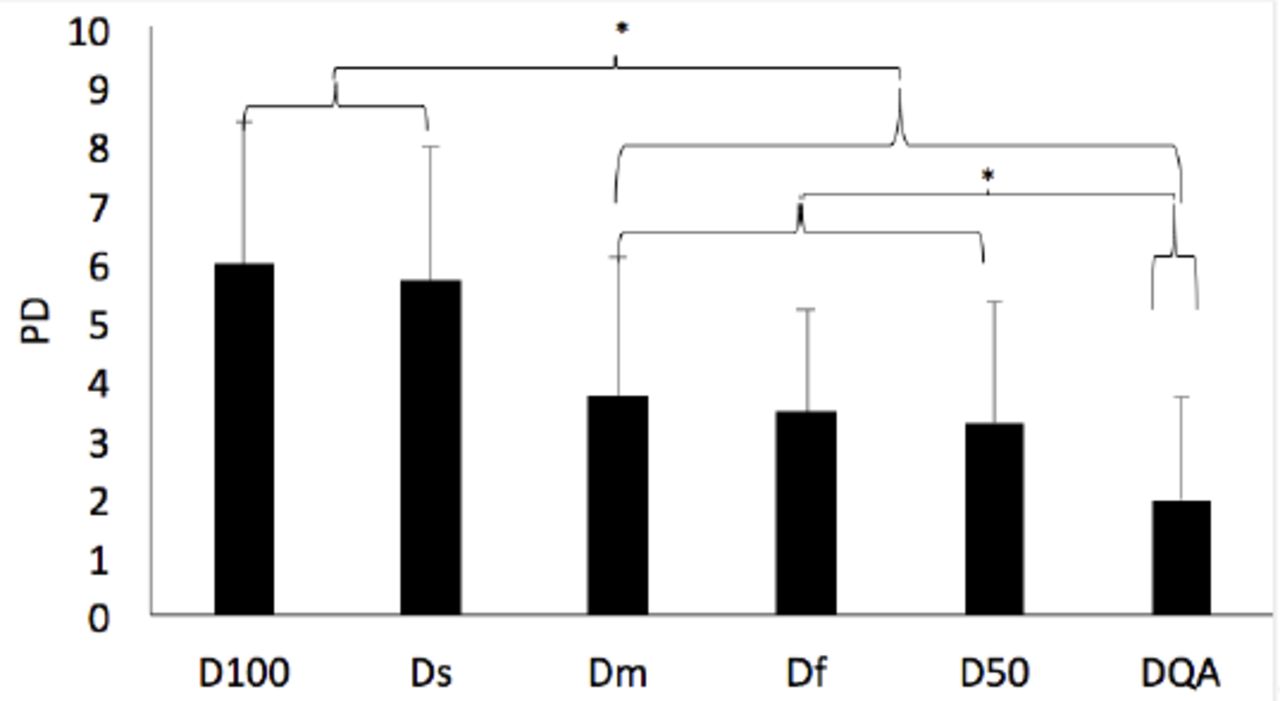
The Friedman test was conducted to compare the perceived difficulty of the cognitive tasks, indicating an effect of the cognitive tasks on the perceived difficulty rating (χ2(5) = 60.847, p<0.001). Post-hoc comparisons identified several statistically significant differences between the tasks (Figure 2).

- The post hoc analysis’s results of perceived difficulty using the Holm-Bonferroni test. D100 - counting backwards, Ds- reverse spelling, Dm- reciting months backwards, Df- verbal fluency, D50- 2-digit determination, DQA-regular conversation, PD- Perceive Difficulty, *- Statistically significant difference at p< 0.05.
Correlation of perceived difficulty with sway
There were significant correlations between the perceived difficulty of tasks and sway measures (Table 3).
- Results of correlation between perceived difficulty and sway using Spearman’s test.
Discussion
The study aimed to provide an evidence-based ranking of the cognitive tasks’ difficulty that is most frequently used in rehabilitation clinics. The main results of our study were: (1) the perceived difficulty scale revealed a statistically significant difference between the cognitive tasks; (2) significant moderate correlations were found between some of the perceived difficulty measures and the acceleration measures.
According to this research’s findings, we assumed that the lack of the cognitive tasks’ effect on sway measures was likely due to our recruitment of healthy participants. Similarly, a study measuring attentional demands and postural control within healthy adults found that DT did not significantly impact postural sway during walking.18 Moreover, regardless of the walking task, the attentional demands needed to maintain standing stability while adding a cognitive task were not affected by changing the sensory contexts in the same participants.18 Furthermore, we assumed that the lack of significant effect of the DTs on sway measures was due to our participants being young (Mean age: 29.4±7.5). Similarly, a study involving healthy older participants with an average age of 73.8 years (±6.0) showed that they experienced greater postural sway when performing dual tasks while standing, compared to younger participants aged between 20 and 40 years.19 Additionally, the healthy young participants were less influenced by the cognitive tasks while maintaining dynamic stability.19
Our results may also be influenced by our use of a simple motor task, such as normal walking, combined with simple cognitive tasks as well. Research has shown that a more complex motor activity, such as walking with a narrow base of support, is more challenging than normal walking when it is combined with an auditory Stroop task.20 Other studies using more sophisticated cognitive tasks, such as visual and auditory Stroop, were able to demonstrate the effects of DTs on motor tasks.21,22 Patel et al22 used four different cognitive tasks and measured their effect on gait speed in healthy adults. The cognitive tasks consisted of visual-motor reaction time, serial subtraction, generating words that start with a certain letter, and color Stroop.22 They found that the walking speed was higher in the visual-motor reaction time task compared to the serial subtraction and generating words that start with a certain letter task, while the lowest walking speed occurred during the color Stroop task.22 Nevertheless, the inconsistency between our results and previous studies can be justified that we aimed to include the most common cognitive tasks that are easy and most appropriate for use in rehabilitation clinics.22,23
Consistent with previous studies, the difficulty of the cognitive tasks (except for reciting months backwards and regular conversation) was found to be correlated with sway acceleration.20,24 Capacity sharing theory could justify the results of our study.25,26 According to capacity sharing theory, there is a limitation in the central processing capacity which means that when two tasks relying on similar neural circuits are performed concurrently, processing speed will decrease.25,26
Additionally, there was no difference between the difficulty of counting backwards and reverse spelling, nor between rating the difficulty of reciting months backwards, verbal fluency, and two-digit determination. We assume that the reason for these findings is either that they are similar in difficulty level or that our simple motor task was not sufficient to elicit differences.
In our study, participants were not directed to prioritize either task. In contrast, Kelly et al20 evaluated the effect of directing focus and the task difficulty on walking in healthy adults.20 Kelly et al20 found that cognitive and motor tasks were influenced by instructed focus tasks. Cognitive response speed was found to be faster when participants were directed to prioritize the cognitive task, and gait speed was faster when participants were informed to focus only on the motor task. Therefore, not instructing the participants to prioritize either the cognitive or the motor tasks might influence the study results.
Limitations
This study included only 26 healthy participants in order to rank the cognitive task based on difficulties. However, further studies that implement these cognitive tasks on larger samples are required. Additionally, the study setting was in the physiotherapy gym where participants walked in a straight walk and even surfaces. A further that is considering a normal daily walk in a multidirectional way and on uneven surfaces might be useful.
Conclusion
In healthy adults, we found differences in the perceived difficulty ratings of the cognitive tasks, but no difference was found in sway between the cognitive tasks. However, the cognitive tasks perceived difficulty was significantly correlated with sway.
Clinical implications
Understanding the progression in difficulty of common DTs is crucial to help rehabilitation specialists design appropriate care plans for their patients. Based on our findings, beginning rehabilitation with DQA would be the easiest cognitive task to combine with a motor task. The next step can be Ds, Df, or D50. Finally, Dm and Df were shown to be the most difficult cognitive tasks that rehabilitation specialists can choose to increase DT difficulty.
Acknowledgments
We would like tothank the Deanship of Scientific Research at Majmaah University for supporting this work under Project Number (R-2024-1490). We would like also to thank SCRIBENDI (www.scribendi.com) for English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received September 22, 2024.
- Accepted December 29, 2024.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.