


Abstract
Pseudogout, also known as calcium pyrophosphate deposition disease, is an inflammatory arthropathy that primarily occurs in the peripheral joints, such as the knee or elbow. Spinal pseudogout is uncommon, and neck pain is its most common clinical manifestation. However, cervical myeloradiculopathy as an initial presentation of pseudogout attack of the ligamentum flavum has rarely been reported in the literature. We report a case of a 65-year-old woman who presented with neck pain, bilateral finger numbness, and left-sided upper extremity weakness. Magnetic resonance images showed an epidural mass at the C4–5 level, compressing the spinal cord. Following laminectomy with removal of the calcified mass, the profound neurologic deficits gradually recovered. A pathological examination confirmed the diagnosis of cervical pseudogout.
Pseudogout, referred to as calcium pyrophosphate deposition (CPPD) disease, is a form of gout-like arthritis that is resistant to digestion by uricase and has no presence of gout.1 Cartilage is the major tissue affected by pseudogout, and the knee is the most commonly involved joint, followed by the wrist.1,2 However, cord compression caused by a calcified ligamentum flavum from pseudogout attack in the cervical spine has rarely been reported in the literature.2-6 We report a case of cervical myeloradiculopathy caused by a calcified ligamentum flavum as an initial presentation of pseudogout.
Case Report
Patient information
This case report was approved by the Institutional Review Board of Chia-Yi Christian Hospital in Taiwan (IRB Number: 2020046). The timeline for this case report was summarized in Table 1. A 65-year-old woman presented with neck pain, bilateral finger numbness, and left-sided upper extremity weakness for 6 months before admission. Her medical history only included hypertension, and her past surgical history only included neurolysis for bilateral carpal tunnel syndrome.
Clinical findings
A neurological examination revealed bilateral hypoesthesia of all digits of the hands and arms, in addition to grade-4 (of 5) muscle power in the left upper extremity. The biceps, triceps, and brachioradialis deep tendon reflexes were all slightly greater than normal. Bilateral Hoffmann signs were present. Laboratory examination showed white blood cell count of 5900/μL and uric acid level of 4.3 mg/μL (normal range: 2.5 to 6.0 mg/dl).
Diagnostic assessment
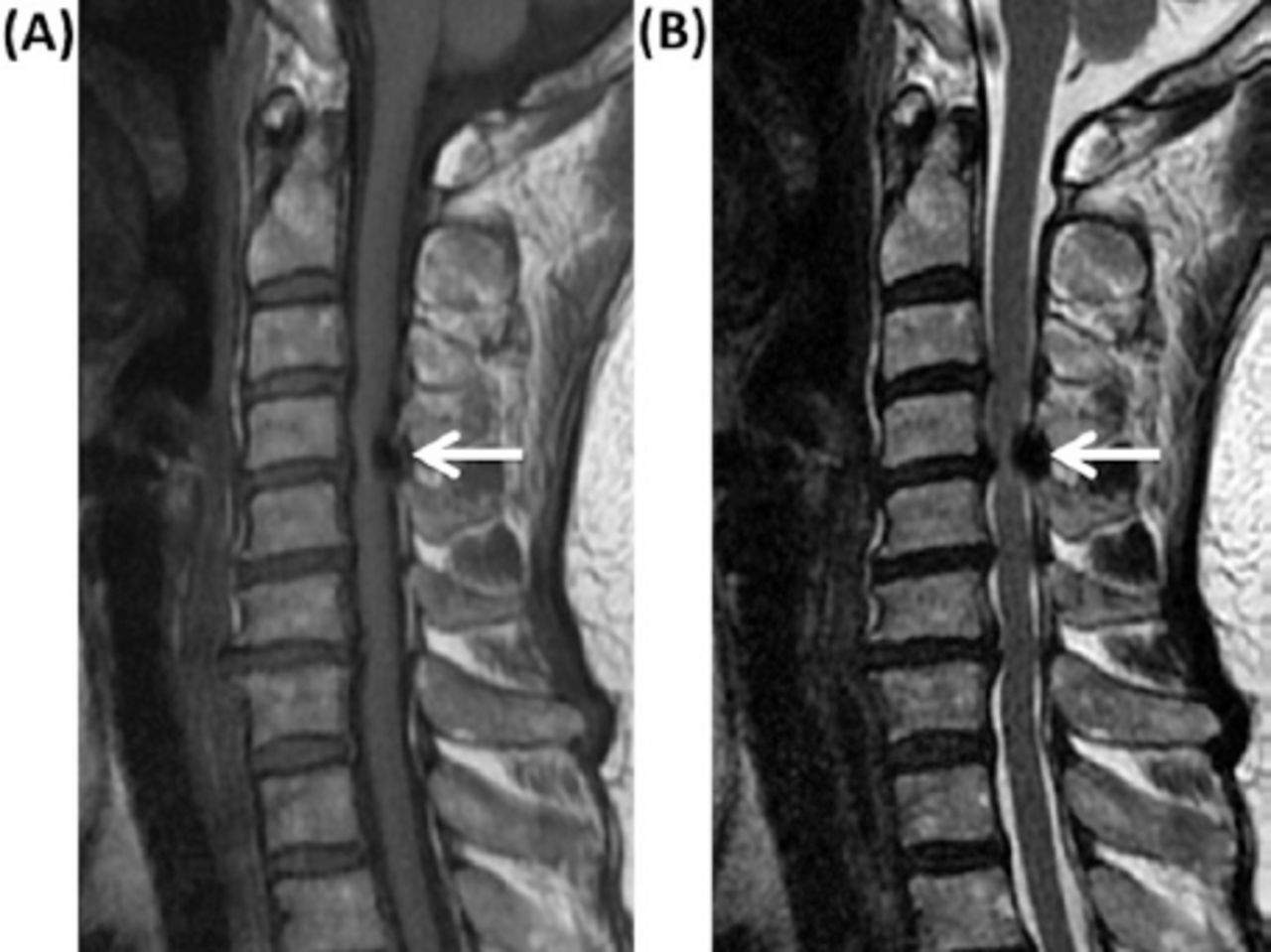
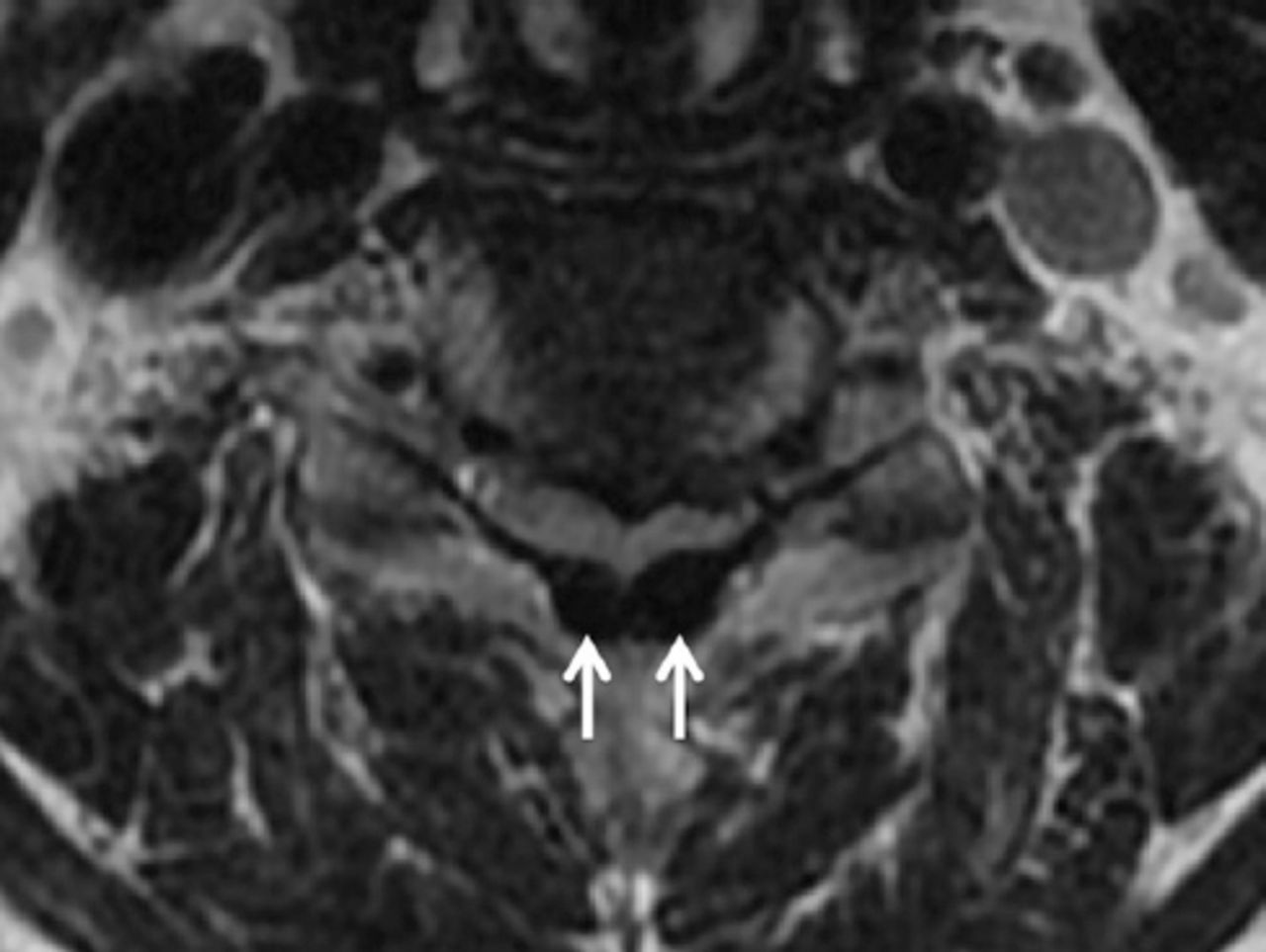
Radiographs of the cervical spine revealed spondylotic spur formations from the C5 to C7 levels (Figure 1). Magnetic resonance imaging (MRI) of the cervical spine revealed multiple herniated discs at C3 to C7 and an epidural mass at the C4–5 level, which was severely compressing the spinal cord. This epidural mass appeared as hypointensity on T1- and T2-weighted images (Figure 2), mainly located in the posterior aspect of the spinal canal (Figure 3).

Lateral view of a cervical radiograph showing marginal spur formation at the C5–6 and C6–7 levels.
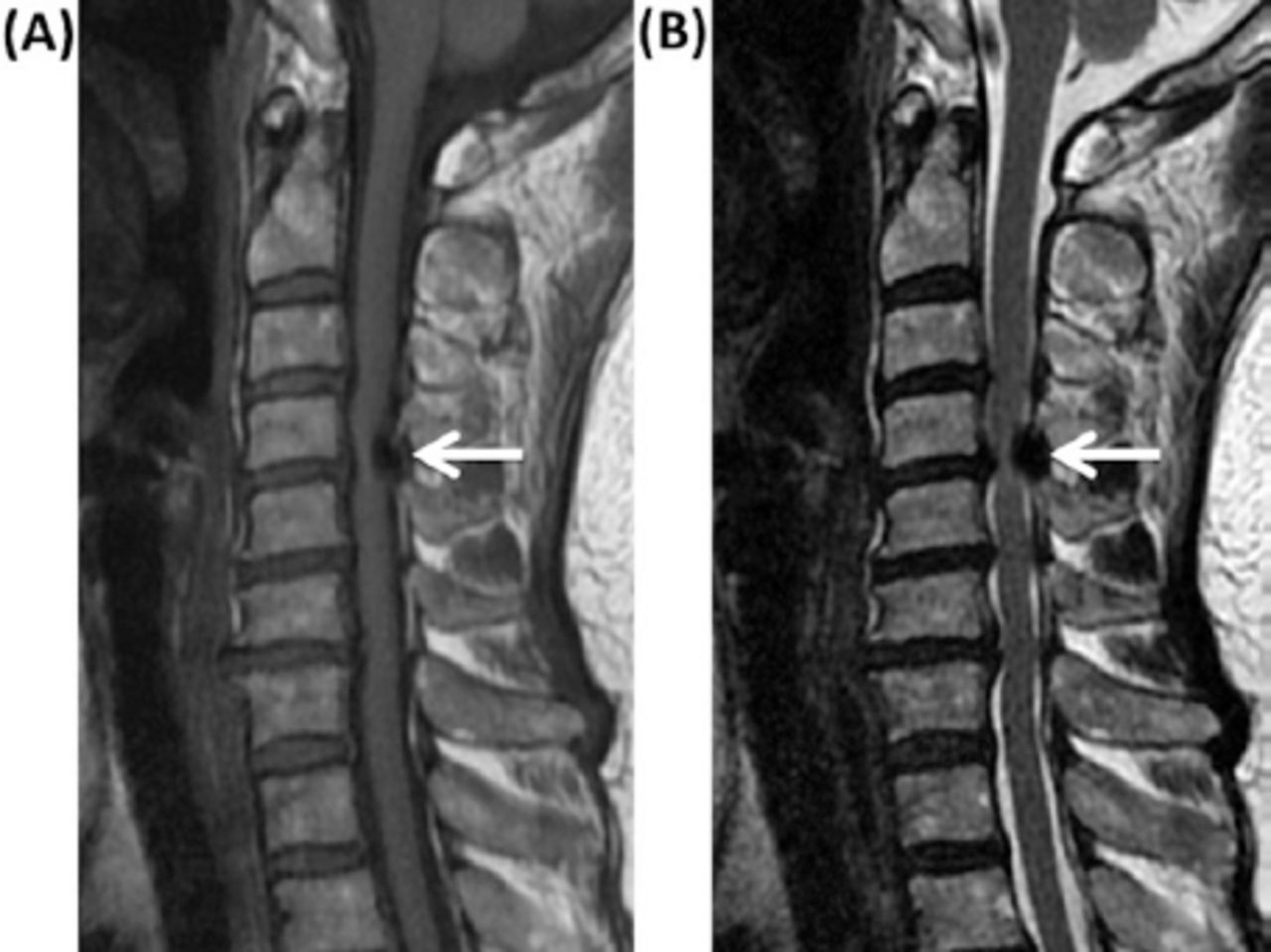
Sagittal views of magnetic resonance images showing the epidural mass (white arrow), located at the C4–5 level, appearing as hypointensity on the A) T1- and B) T2-weighted images.
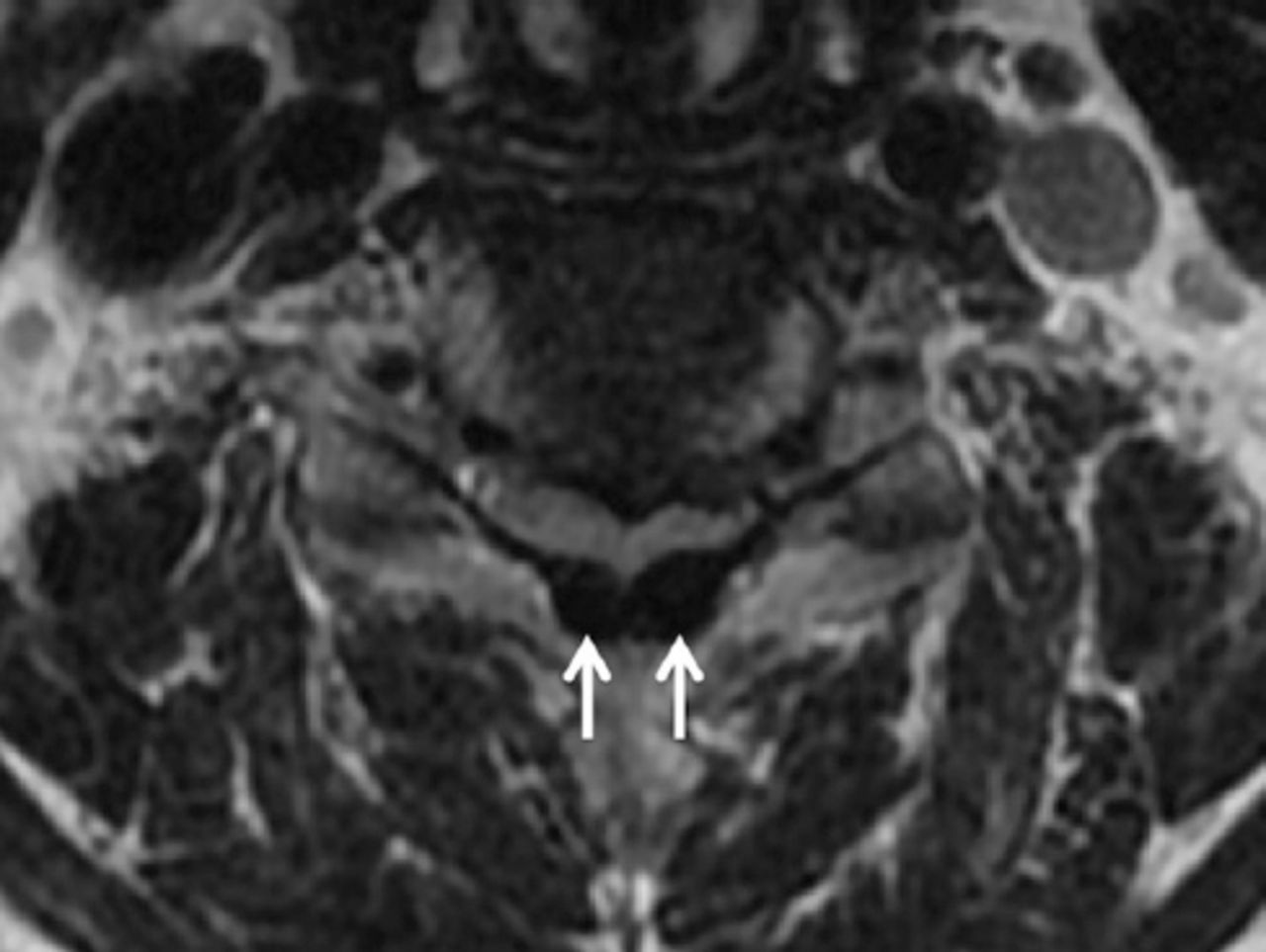
Axial view of a T2-weighted magnetic resonance image showing the epidural mass (white arrows), which was mainly located in the posterior aspect of the spinal canal around the ligamentum flavum.
Therapeutic intervention
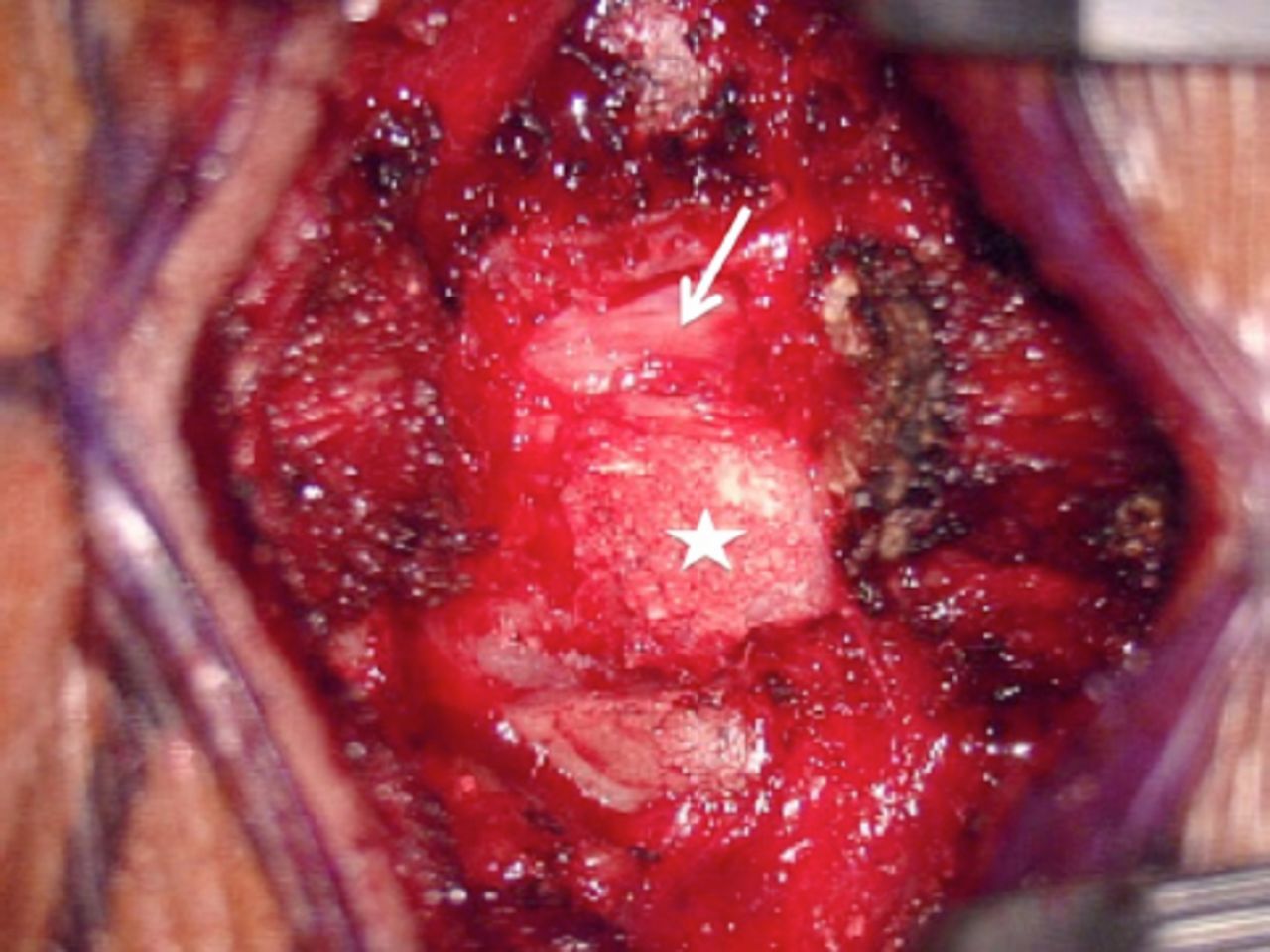
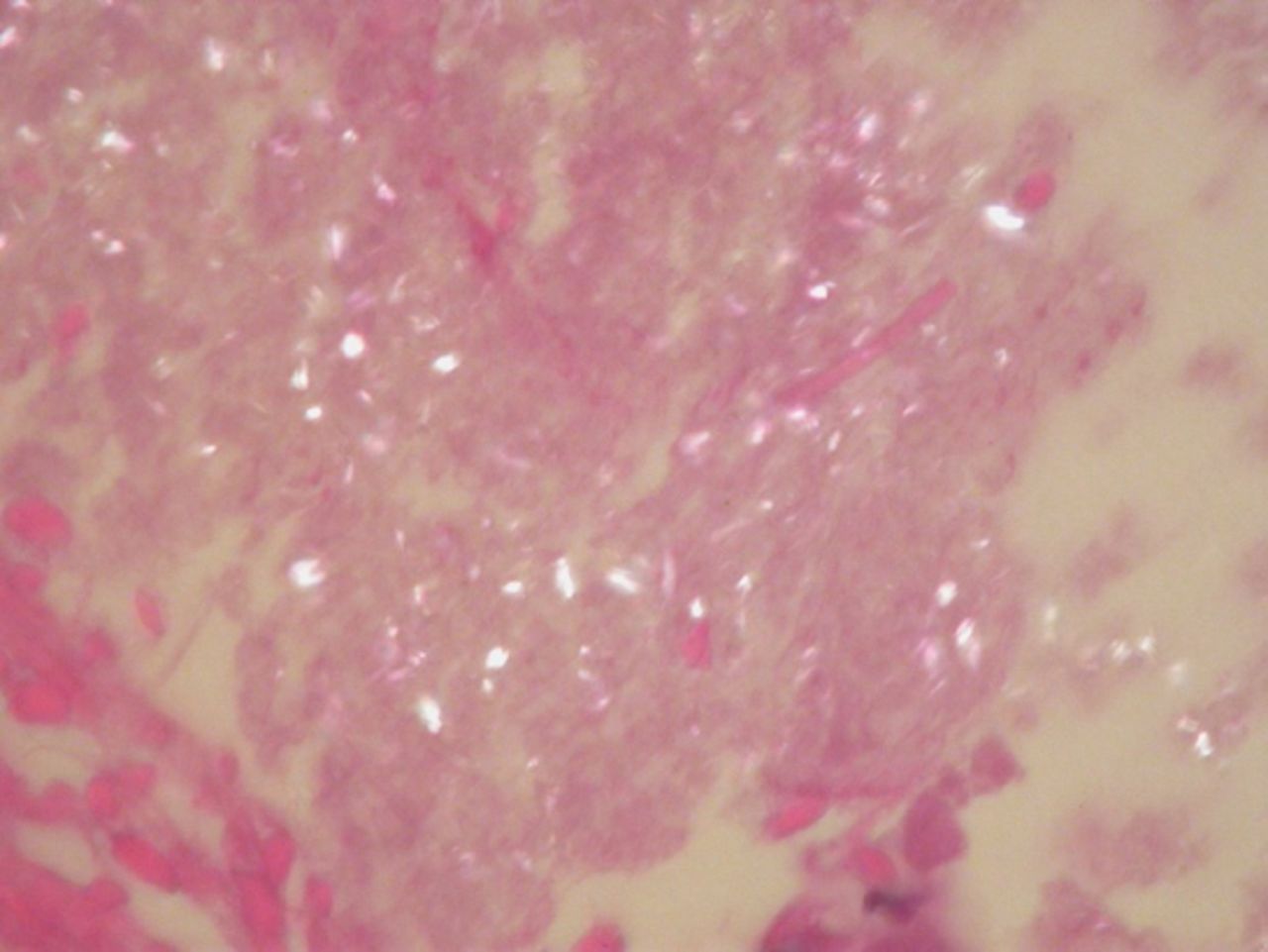
Upon receiving a diagnosis of cervical myeloradiculopathy associated with an epidural mass, the patient underwent posterior laminectomy of the C4 level to remove the epidural mass and decompress the spinal cord. At operation, a white and calcified substance intertwined with the ligamentum flavum at the C4 level was totally removed (Figure 4). This mass did not involve the dura mater or facet joint. Pathological examination with a polarized light microscope revealed deposits of short, rhomboid crystals (calcium pyrophosphate) in fibrous tissue in addition to surrounding fibroblasts and calcified spots, which were compatible with the diagnosis of pseudogout (Figure 5).
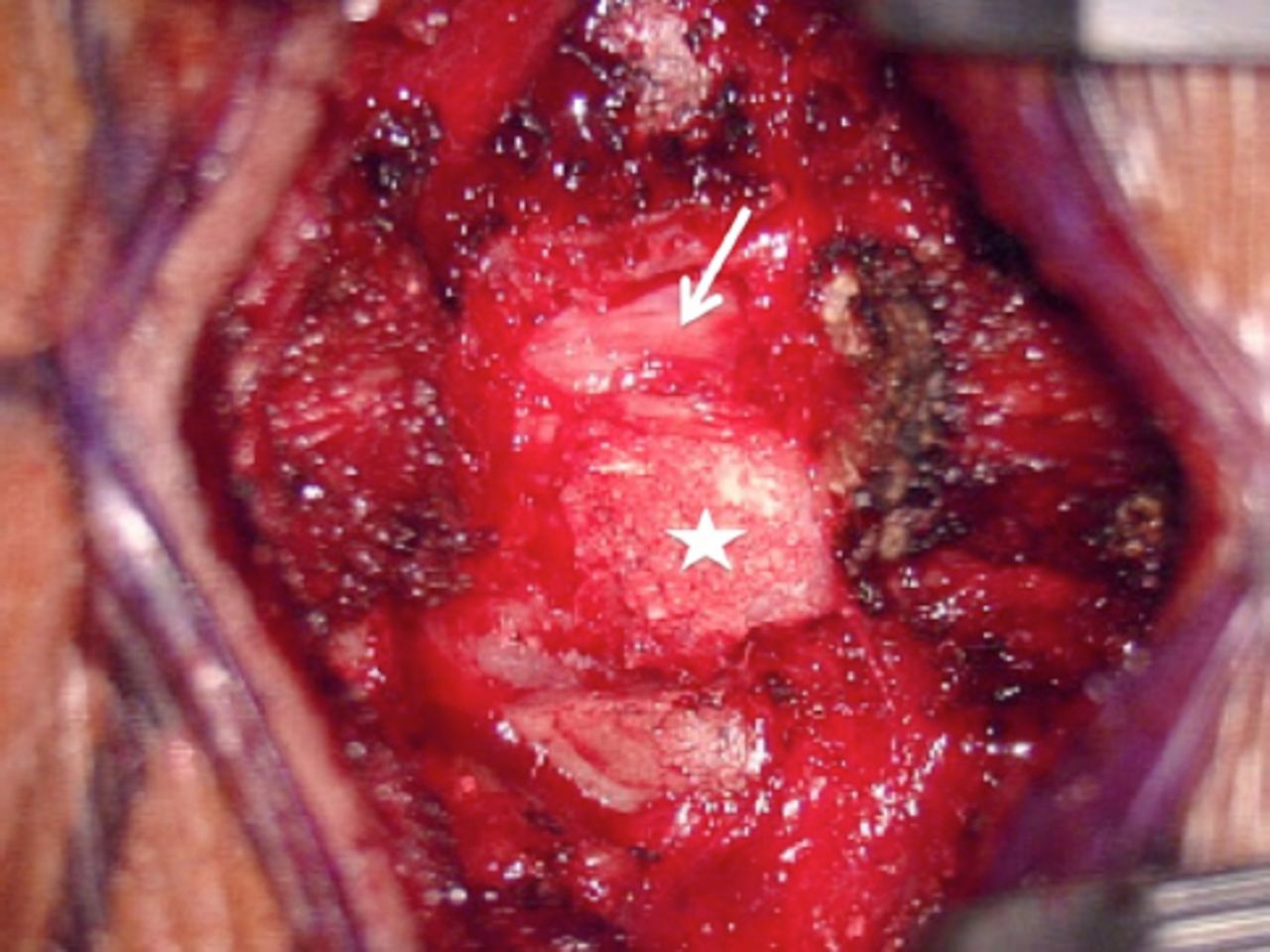
Intraoperative view showing that the spinal cord (white arrow) was severely compressed by the white and calcified substance that was intertwined with the ligamentum flavum (white asterisk) following laminectomy.

Polarized light-microscopy view showing deposits of short and rhomboid crystals (calcium pyrophosphate), which were compatible with the diagnosis of pseudogout.
Follow-up and outcomes
Postoperatively, the motor strength of the left upper extremity fully recovered. Only bilateral fingertip numbness was observed during the patient’s visits to a regular outpatient department.
Discussion
The CPPD disease, also known as pseudogout, is an inflammatory arthropathy caused by the deposition of calcium pyrophosphate dehydrate crystals, which are associated with dysfunctions in several transporter and phosphatases.1 The prevalence of CPPD disease increases with age, and it is rare in patients aged younger than 50 years.7,8 Risk factors for CPPD disease include hyperparathyroidism, osteoarthritis, and loop diuretic use.9 CPPD disease tends to be considered a disorder of the peripheral joints, and phosphate crystallization can occur in the articular cartilage, tendons, and ligaments.10 However, spinal pseudogout is uncommon, and it has been found to involve the intervertebral disc, synovial joint, articular cartilage, or ligaments.7 Most instances of pseudogout occur in the transverse ligament of the atlas, leading to the development of crowned dens syndrome.11 At present, spinal cord compression caused by pseudogout of the ligamentum flavum in the cervical spine, as in our case, has rarely been reported in the literature.2-6
The CPPD disease may affect only the spine, but its involvement is commonly asymptomatic.10 The clinical manifestation of pseudogout in the cervical spine depends on the severity of affected neural structures. In a prevalent case-control study of the cervical spine in CPPD disease, Finckh et al8 reported neck pain and discomfort to be the most common symptoms in patients with spinal pseudogout. Furthermore, in a retrospective study of 14 patients with cervical pseudogout, Sekijima et al12 noted acute posterior neck pain and fever to be the chief symptoms. In one study, the severity of pain was significantly and positively correlated with the extent of cervical calcified deposits.8 Radiculopathy, myelopathy, or myeloradiculopathy may develop when those calcified ligaments formed by pseudogout collectively result in a large compression of the nerve roots or spinal cord.7 However, cervical myeloradiculopathy caused by a calcified ligamentum flavum from pseudogout attack has rarely been reported.2-6 In a literature review of 26 published cases of compressive cervical myelopathy from pseudogout involving the ligamentum flavum, Fye et al2 reported that 80% of cases of the disease were in women (mean age: 71.4 years; mean duration between onset of symptoms of cervical myelopathy and diagnosis: 7.7 months). Our present case also involved an old woman (age: 65 years) who had symptoms of cervical myeloradiculopathy for 6 months.
Chondrocalcinosis, the deposition of CPPD crystals into the fibrous or hyaline cartilage, is a common finding in radiographic studies, including those employing X-ray or computed tomography (CT) scans.10 Pseudogout can occur with no radiological indication of chondrocalcinosis.1 Among patients with CPPD disease, 70% exhibit calcified deposits in their upper cervical spine, especially in the transverse ligament of the atlas.8 For the diagnosis of calcified ligamentum flavum with cord compression, the use of CT and MRI is crucial for confirming which areas are calcified and which neural structures are affected.7,13 The differential diagnosis of epidural calcification include those for pseudogout, gout, ossification of the ligamentum flavum, amyloidosis, and hyperparathyroidism associated with chronic renal failure or tuberculosis.14 However, the diagnosis of calcium pyrophosphate crystals only can be confirmed through findings from a light microscope, compensated polarized light microscope, or phase contrast microscope—specifically through indications of a characteristic parallepipedic form and intracellular predominance with absent or weak positive birefringence.1,10
Surgical decompression is the gold standard treatment for patients with cord compression from a calcified cervical ligamentum flavum.2 Laminectomy alone with the removal of the calcified mass has been the common procedure in published cases, and most patients have had a positive outcome, as with our case.2-6 If these crystals involve the cervical facet joint, posterior fusion is required to prevent spinal instability. The calcified ligamentum flavum may tend to adhere to the dura mater, and postoperative cerebrospinal fluid leaks are likely to be troublesome during the separation of the ossified lesion from the dura. In our case, because the calcified ligamentum flavum did not adhere to the dura, the ossified lesion could be removed with the en bloc method.
In conclusion, although CPPD disease is a common aging-related disorder, cervical myeloradiculopathy may be an initial presentation of a calcified ligamentum flavum from pseudogout attack. Early surgical decompression and microscopic examinations can mitigate the profound neurological deficits induced by the disease and provide an accurate diagnosis.
Footnotes
Disclosure. The authors declare no conflicting interests, support or funding from any drug company.
- Received July 21, 2021.
- Accepted August 18, 2020.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.