


Subacute sclerosing panencephalitis (SSPE) is a progressive neurological disorder manifesting in school going children with cognitive decline and myoclonic jerks. It results from persistent infection of immune resistant measles virus infection. Most of the patients of SSPE have a primary measles infection at an early age, before 2 years. It usually develops from 6-8 years after the primary measles infection but can range from 2 years to more than 30 years. It is considered that measles immunization protects against SSPE and the measles vaccine virus itself does not cause SSPE.1 There are discrete case reports of development of SSPE following vaccination or in a fully immunized child.2
Age at onset of symptoms could range from 3-31 years. Onset as early as 27 months has also been reported in medical literature.2 We are presenting an interesting case of fulminant SSPE in a young 20 month Indian boy who was fully vaccinated for measles and did not have any prior exposure to measles. This case is presented with the intent to consider the clinical possibility of SSPE based on clinical phenotype irrespective of age at onset and presence or absence of natural measles infection in the past.
A 20-month-boy presented with complaints of weakness on the left half of the body and progressive decline in cognition for the duration of one month. He also developed multiple episodes of myoclonic jerks in the body. He was a product of non consanguineous marriage with an uneventful perinatal period. He had attained age-appropriate milestones. There was no definitive past history of measles. He was immunized for age as per national immunization schedule including measles vaccine at 9 months and Measles, Mumps, Rubella vaccine at 16 months of age. There was no neurological illness in any of the family members.
On examination, he was restless, irritable with lack of alertness or interest in surroundings. There was no cranial nerve palsy. Fundus evaluation suggested primary optic atrophy. On motor examination, power across joints of the left upper and lower limb was 3/5 against preserved antigravity movement (>3/5) on the right side. He had frequent myoclonic jerks involving the head, trunk, and all 4 limbs. In addition, he had dyskinesia of all 4 limbs with near continuous distal writhing movement of both hands. Deep tendon reflexes were difficult to elicit and plantar response was equivocal with evidence of striatal toe. Rest of the systemic examination was unremarkable.
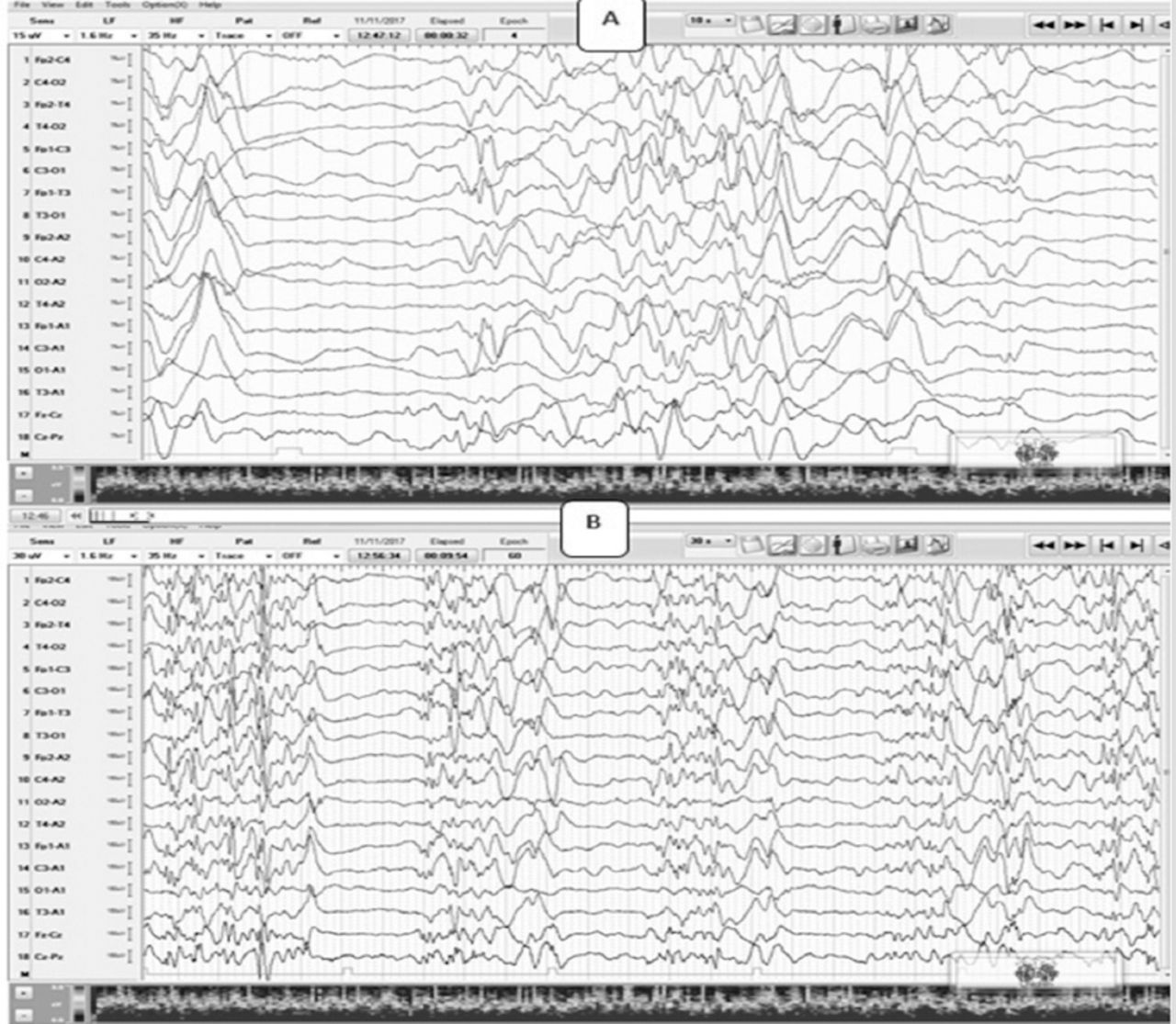
In view of early-onset neuroregression with predominant extrapyramidal features, myoclonic jerks, cognitive decline and evidence of optic atrophy, possibilities of neuronal ceroid lipofuscinosis and mitochondrial disorders were kept. Magnetic resonance imaging (MRI) of the brian did not reveal any significant abnormalities except for small discrete asymmetric periventricular and subcortical white matter changes. Electroencephalogram (EEG) revealed a slow background with a paucity of sleep markers. There were high amplitude (300-350 µV, 1-1.5 Hz) slow wave complexes in the pseudoperiodic interval. (Figure 1)

Electroencephalograph (EEG) shows slowing (1-2 Hz, 20-30 uV) of sleep background with paucity of sleep markers. There are interspersed high amplitude (300-350 uV, 1-1.5 Hz) slow waves (A) that have a pseudoperiodic pattern (B) evident on decreasing the paper speed (B).
Cerebrospinal fluid (CSF) examination showed normal cytology, normal lactate (1.1 mmol/l), normal protein (35 mg/dl) and sugars (59 mg/dl) against venous sugar of (74 mg/dl). Cerebrospinal fluid: serum antimeasles IgG antibody ratio by Enzyme-linked immune sorbent assay was one: 625 suggesting a clinical diagnosis of subacute sclerosing panencephalitis. He subsequently started on oral Isoprinosine. Owing to financial constraints, he could not afford the medication. There was a progressive clinical deterioration to the current vegetative state within 2 months of onset of illness depicting a fulminant course of the illness.
The typical latency period of SSPE after measles infection is 6-10 year but it can occur as early as 2 years of age. The present case had a latency of 4 months from the last vaccination. Few authors have reported a short latency of 3-4 months following measles infection in young toddlers diagnosed with SSPE.3 Children who got infected with measles under the age of one year old have a higher risk of SSPE than those infected at age 5 year old or later. An immunized 27-month-old baby was reported with the fulminant course of SSPE from North India. Aulakh et al,3 have reported a case of SSPE in 2 and a half-year-old child with cognitive decline and myoclonic jerks who had measles 4 months prior to the onset of symptoms.
Subacute sclerosing panencephalitis of short latency is usually associated with congenital and neonatal measles infection. Perinatal infection of the infant, by maternal measles infection during delivery, may develop to SSPE with a short latency and devasting course of illness. Measles vaccine does not accelerate the course of SSPE, trigger SSPE or cause SSPE. This upsurge of SSPE cases in early childhood raises concerns about inadequate vaccination and need for the second dose of measles vaccine.4 New Papua Guinea has witnessed a series of cases of SSPE subsequent to inadequate measles coverage.5
The most common ocular findings in SSPE include macular retinitis and macular pigment disturbance. Considering the onset of cognitive decline and myoclonic seizures, clinical possibilities of neuronal ceroid lipofuscinosis (NCL) and mitochondrial disorders were entertained. However, the absence of pigmentary retinal changes and cerebellar atrophy on neuroimaging makes NCL less likely. Similarly, normal CSF lactate with non specific neuroimaging findings disfavors the clinical differential of mitochondrial disorders.
Presence of cognitive decline, myoclonic jerks in a child aged more than 5 years old with past history of measles, lack of complete immunization, poor socioeconomic background with EEG showing pseudoperiodic high amplitude discharges is considered SSPE unless proven otherwise. There were 3 atypical features of SSPE in our case: early age at onset, fulminant clinical course, and occurrence in a previously immunized child with the absence of a natural history of measles infection. It is difficult to attribute the present diagnosis of SSPE to vaccination received at 9 months and 16 months of age. We rather believe in the possibility of subclinical measles infection probably overlooked by parents.
In conclusion, we believe that despite effective coverage of measles immunization in our country, a fatal disease like SSPE continues to haunt fully vaccinated children. This report alerts the clinician to consider a possibility of SSPE even in younger and fully vaccinated children with cognitive decline and myoclonus.
Illustrations, Figures, Photographs
All figures or photographs should be submitted in a high resolution (minimum 300 DPI) electronic version saved in jpeg or tiff format. Original hard copies of all figures may be requested when necessary. Photographs will be accepted at the discretion of the Editorial Board. All lettering, arrows, or other artwork must be done by an artist or draftsman. If arrows are used please ensure they appear in a different color to the background color, preferably black with a white border, or white with a black border. If arrows distinguish different items on the figure then different arrow styles should be used ie. long, short, wide, narrow. Written informed consent for publication must accompany any photograph in which the subject can be identified. Written copyright permission, from the publishers, must accompany any illustration that has been previously published.
Footnotes
Disclosure. The authors declare no conflicting interests, support or funding from any drug company.
- Received April 22, 2018.
- Accepted August 8, 2018.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue




{kind=link}
Related Articles
Cited By...
- No citing articles found.