


Abstract
Tumefactive demyelinating lesion is a variant of multiple sclerosis that is a diagnostic challenge. Tumefactive demyelinating lesion requires extensive work-up as its clinical and radiological features are often indistinguishable from other central nervous system lesions, such as tumors. Diagnosis is further complicated by the increasing recognition that tumefactive demyelinating lesions can occur alongside, evolve into, or develop from numerous conditions other than multiple sclerosis, pointing to a possible overlapping etiology. We review herein relevant studies from 2017 onwards to provide a current view on the pathogenesis, clinical and imaging findings, novel diagnostic techniques for differential diagnoses, and management of tumefactive demyelinating lesions.
Tumefactive demyelinating lesions (TDLs) are a rare and distinct variant of the multiple sclerosis (MS) spectrum of diseases.1 As the name suggests, TDLs can morphologically mimic primary brain tumors on magnetic resonance imaging (MRI),2 posing a diagnostic challenge. The high rate of misdiagnosis of TDLs as MS is concerning, especially because some MS therapies may cause TDLs. Accurate diagnosis is often difficult owing to the possible coexistence of TDLs with other syndromes and the scarcity of established information and consensus on diagnostic and management guidelines. However, a large number of TDL case reports, including methods for differentiating TDL from common mimics, as well as new research on risk factors, have been reported over the last few years. In this study, we build on previous knowledge by reviewing the latest findings on TDLs. Our aim was to provide the latest information on the etiology, diagnosis with MRI, novel imaging methods, and management of TDL in a single and accessible article.
Definition
There is no official definition of TDLs or mention of them in the 2017 McDonald criteria.3 However, TDLs are consistently described in the literature as acute, large (>2 cm), demyelinating CNS lesions accompanied by cystic changes or ring enhancement on MRI, with little or no mass effects.2,4,5 A recent review proposed that lesions between 0.5 cm and 2 cm (with or without mass effect) that have MRI characteristics likely to be mistaken for tumors also be added to the common definition to include MS patients exhibiting smaller tumefactive plaques.6 The TDL is often referred to as tumefactive MS in the literature as it can be associated with the relapsing-remitting form of MS (RRMS) and is now recognized as a variant of MS.1,2 However, this name is slightly misleading as TDL may occur as a clinically isolated syndrome or be associated with other conditions such as neuromyelitis optica spectrum disorder (NMOSD), Balo’s concentric sclerosis (BCS), or acute disseminated encephalomyelitis (ADEM).4
Epidemiology
Several reviews have reported that TDL is prevalent in 1-3 per 1000 cases of MS,1,4,6 yet the overall prevalence of TDLs, including isolated cases and those associated with other syndromes, has not yet been assessed. The age at onset commonly ranges between 107 and 66 years,8 but one study reported a mean age at onset of 27 years. A female predominance has also been reported.1,9
Etiology and pathogenesis
The MS may share a common etiology with TDL; they often occur concurrently, exhibit demyelination with possible perivascular edema, show oligoclonal bands (OCBs) in the cerebrospinal fluid (CSF), and respond to plasma exchange (PLEX) and rituximab (anti-CD20) treatments.1,5,10 Although TDLs remain largely unexplored, the pathogenesis and risk factors for MS have been relatively well studied. One model of MS pathology proposes that peripheral B cells escape tolerance checkpoints because of diminished regulation by fatigued or genetically mutated regulatory T cells. The escaped B cells then interact with interferon-producing helper T cells in the lymphoid organs, resulting in the further release of pathogenic cells across the blood–brain barrier. In the CNS, pathogenic B cells and infiltrating killer T cells are activated, initiating the pathology of MS.10 Persistent infections, such as those caused by the Epstein–Barr virus, as well as T-cell genetic variants, may contribute to the onset of pathogenesis.10 Analyses of MS genetics have mapped associations with human leukocyte antigen class II alleles, particularly the DRB1*15 variant that increases the risk by three fold, implicating antigen-presenting cells and CD4+ T-cells.11,12 Several major histocompatibility complex class I alleles are involved in protective effects, implicating CD8+ and natural killer cells.11
Reviews show that 35-62% of TDLs are monophasic and are diagnosed in a clinically isolated form,9 although some may transform to RRMS or take the form of recurrent TDLs.5 Several cases of TDLs forming alongside ADEM have also been documented. Although the underlying mechanisms are still unknown, they may be partially explained by the malresponsive T-cells associated with both disorders.13
Additionally, a relationship among TDLs, MS, BCS, and NMOSD has also been observed,14,15 where one disorder may evolve into another, several BCS lesions can coalesce to form a TDL, and the TDL may also develop into BCS. As with TDLS, BCS can also progress into MS or NMOSD, and BSC-type lesions are found in both MS and NMOSD. This relationship points to a common etiology; however, apart from demyelination being a common factor in all 4 disorders, the mechanisms underlying this interdependency are currently unknown.14 A small proportion of cases may be explained by an initial misdiagnosis of BCS as a TDL, which can occur if a concentric ring pattern is not discernible.14
Despite the large female predominance observed in most studies (e.g., F/M sex ratio of 2.3:1),8 some found only slight or no differences between the sexes, and one study even found male predominance.7 Although the reason for the female predominance in TDL is unclear, there have been associations between sex hormones and MS: decreased risk of relapse during pregnancy attributed to increased Th2 response and estriol; low testosterone levels in many male and female patients with MS; and the effect of sex hormones on T cells, B cells, and remyelination.16 Further research may provide alternative therapeutic options.
Over the last decade, there has been a steady accumulation of cases linking the onset of TDLs and worsening of neurological status (WNS) to the cessation of fingolimod therapy (FTY) or switching from other therapies to FTY.17–22,23 Fingolimod binds to sphingosine-1-phosphate receptors on a subset of lymphocytes and prevents their exit from the lymph nodes, thereby reducing their concentration in the peripheral blood and CNS.24 In one retrospective study, 4 of 8 MS patients who had stopped FTY developed WNS within a mean of 4±0.9 months and reached Expanded Disability Status Scale (EDSS) scores of up to 9.5, and 1 patient died. Of the 4 patients with WNS, three showed TDL on MRI, and one showed a punctuated pattern.22 A Japanese study reinforced these findings, reporting that 52.6% of patients with MS experienced WNS after FTY cessation.20 Patients with high disease activity before starting FTY or those who respond well to FTY may be at highest risk of severe relapse after FTY cessation.25 The TDLs are relatively rare in patients who have had MS for several years; however, FTY-induced TDLs often occur in patients with established MS, indicating a medication-induced redistribution of peripheral lymphocytes.20,24,25
Numerous similar rebound effects have been observed after the discontinuation of natalizumab therapy (a monoclonal antibody against α4-integrin) for MS24 and in one case of TDL development during natalizumab therapy.26 Cases of TDL occurring after the cessation of alemtuzumab treatment, although much rarer, have also been reported. Even though the mechanism of action of alemtuzumab (an anti-CD52 monoclonal antibody) is different from that of FTY, it also appears to alter peripheral lymphocyte populations.27 A case of TDL emerging during treatment with ocrelizumab, an intravenously infused humanized anti-CD20 monoclonal antibody, was recently reported.28 The patient’s pre-infusion CD19 level was approximately 0.7%, suggesting limited reconstitution of B cells. However, it was unclear whether reconstitution led to an exaggerated immune response.28 No similar cases have been previously reported for ocrelizumab or rituximab, but other CD-20 monoclonal antibodies are often used to treat MS.
Lastly, cocaine users may be at an increased risk of levamisole-induced multifocal inflammatory leukoencephalopathy, which was recently associated with the development of TDLs masquerading as BCS in three separate cases.29
Clinical presentation
The presentation of TDL is variable and depends on the location and size of the lesion; however, the most common presenting symptoms are hemiparesis, hemisensory deficits, visual field deficits, headaches, aphasia/dysphasia, apraxia, cognitive abnormalities, confusion, and changes in consciousness.1,5,30,31 A recent retrospective study of 87 cases in which the first clinical event showed one or more TDLs provided valuable data on the frequency of presenting symptoms in patients with TDL.8 Overall, 67% of the patients had hemiparesis or hemiplegia, 38% had sensory disorders, 26% experienced dizziness, and 24% had optic neuritis.
Aphasia, headache, and cognitive disturbances were observed in 15%, 18%, and 15% of the patients, respectively.8 Conversely, one case of “silent” TDL has been reported, in which the only symptom over 2 years was a mild tremor of the hands despite a large TDL in the left frontal area and smaller lesions in the subcortical white matter.31 Lesions mainly occur at the supratentorial level, centered in the white matter, with possible extension into the cortical gray matter.1,5,14 Lesions in the brainstem30 and spinal cord5 have also been reported, although rarely. In the study by Tremblay et al.4 TDL was the first neurological event in 62% of the patients, while approximately 7% had a prior diagnosis of MS and 3.5% had optic neuritis. Other studies have also reported progression to MS in 46-78% of TDL cases.1
Imaging findings
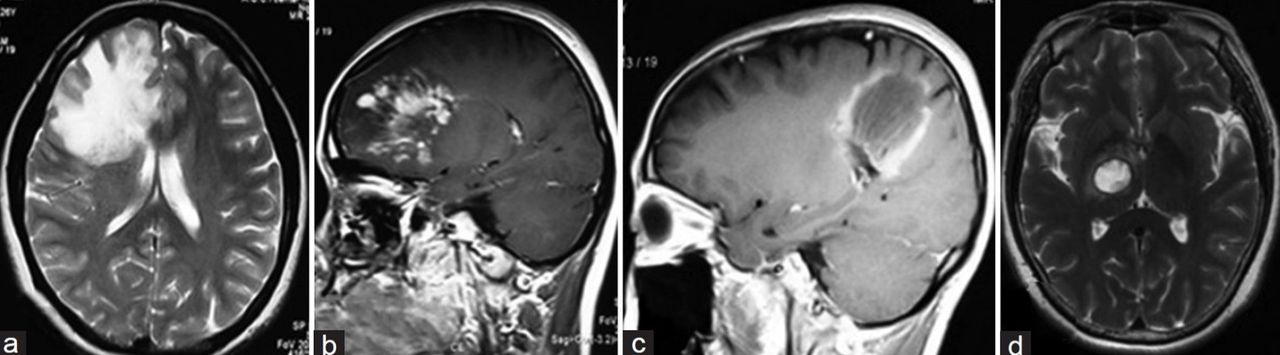
The TDL lesions are classified into 3 types according to their MRI features: (1) infiltrating: T2-weighted images (T2WI) show a diffuse, infiltrating growth pattern with indistinct margins and heterogeneous enhancement (Figure 2, a and b);5 this is present in approximately 50% of the cases;18 (2) ring-shaped: are round or oval and have either a closed-ring or open-ring enhancement on T1-weighted images (T1WI) (Figure 2 c);5 combined prevalence of open and closed rings is 53%;9 and (3) megacystic: hypointense on T1WI and hyperintense on T2WI with distinct margins and ring enhancement (Figure 2 d).5 A fourth type of lesion, that is, balo-like, was described in one study.9

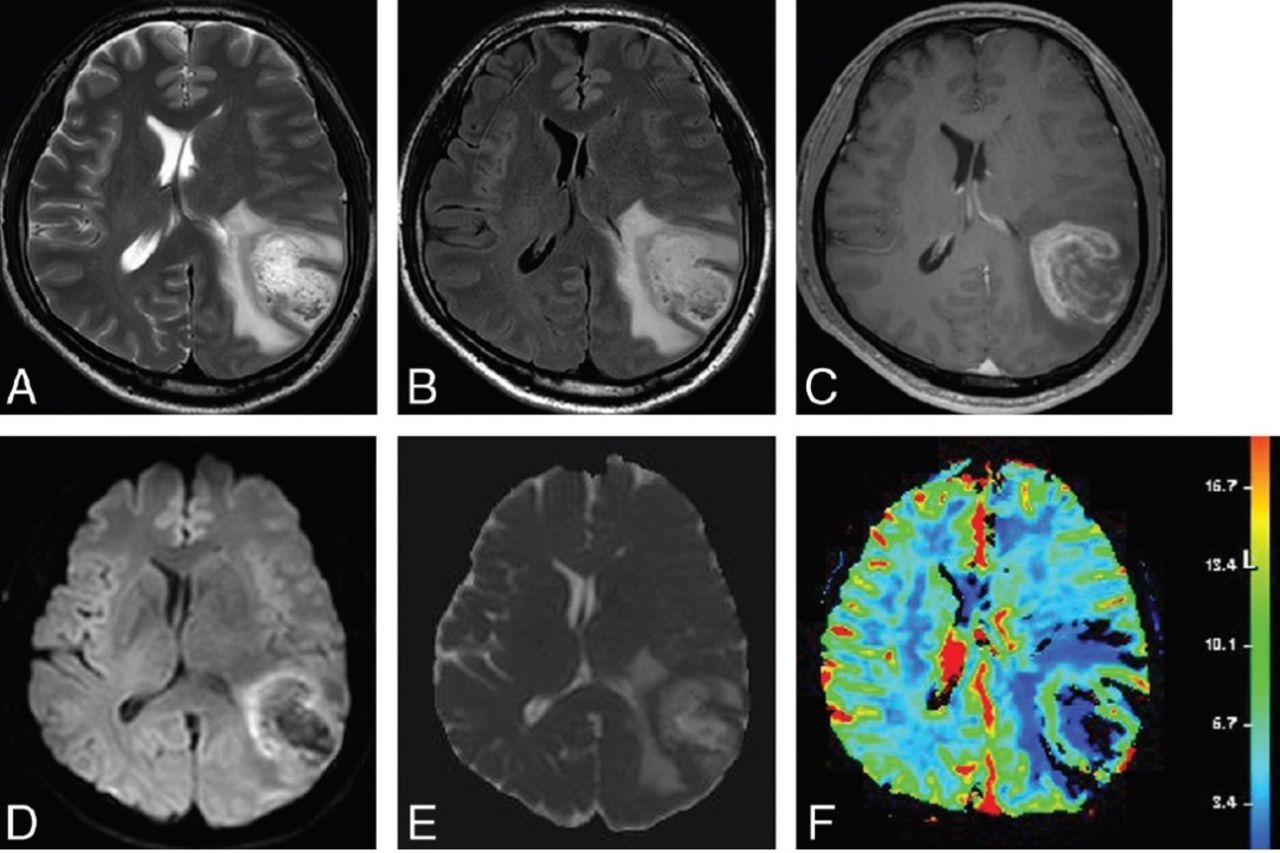
- Magnetic resonance images from a male patient with biopsy-confirmed TDL. A) Axial T2-weighted and (B) axial FLAIR images show a well-defined hyperintense lesion in the left cerebral hemisphere with mild perilesional edema. (C) Contrast-enhanced axial T1WI shows open ring enhancement. (D) Axial DWI and (E) the corresponding ADC map reveal high ADC in the lesion and peripheral restricted diffusion. (F) DSC demonstrates low cerebral blood volume. Adapted from Suh et al.9

- Three cases of TDLs showing the three different types of morphology on MRI: (a) Axial T2-weighted image showing diffuse, infiltrating lesion with indistinct margins. (b) Sagittal T1-weighted image with contrast highlighting infiltrating lesion heterogeneous enhancement. (c) Sagittal T1-weighted image with contrast showing ring-shaped enhancement. (d) Axial T2-weighted image demonstrating megacystic lesion with distinct margins.5
A meta-analysis of MRI images from 19 studies involving 476 patients with TDLs calculated a 35% incidence rate of open-ring or incomplete rim enhancement—significantly higher than the incidence of closed-ring or complete rim enhancement at 18%.9 Additionally, the incidence of a T2 hypointense rim was 48%; absent or mild mass effect, 67%; and absent or mild perilesional edema, 57% (Figure 1).9 Another study reported an open ring in up to 75.9% of pathologically confirmed TDL cases.4
The mean lesion size is 26.9 mm (range, 20-55 mm).8 Analyses of lesion topography from 30 patients revealed parietal lobe location in 73%, frontal lobe location in 30%, and cerebellar lobe location in 17% of the patients. On T1WI, 81% showed gadolinium enhancement, and 51% showed ring formation. Further, in contrast to a previous review, only 9% had an open ring. Moreover, 25% of the cases had a homogeneous surface, 10% were heterogeneous, 8% were punctiform, and 6% were strata.8 However, the study had a much smaller sample size.
Advanced imaging for differential diagnosis
A limitation of conventional MRI is the poor resolution of the microtissue structure and often inconclusive results; hence, several advanced or alternative imaging techniques have been explored to aid in the diagnosis of TDLs. Dynamic susceptibility contrast (DSC) is the most commonly used technique to distinguish neoplastic from non-neoplastic lesions using relative cerebral blood volume (rCBV) as an indicator of neovascularization.32 The TDLs have shown significantly lower rCBVs than high-grade gliomas (HGGs), with a mean rCBV of 2.11±1.12 and 3.77±1.65, respectively.32 However, other studies have measured mean rCBVs much higher than 2 and up to 6,33 pointing to some neovascularization or vasodilation. Although a low rCBV favors a diagnosis of TDL over HGG, a high rCBV does not rule out TDL (Table 1). In such cases, the combination of DSC with diffuse tensor imaging (DTI) can increase the sensitivity of distinguishing TDLs from HGGs.32
- Common differential diagnoses of TDL and their main distinguishing laboratory and imaging features.
The DTI allows the visualization of neuronal tracts and is especially sensitive to disruptions in the white matter by analyzing water diffusion.34 Compared to HGGs in which diffusion is normal or only slightly restricted, TDLs show restricted apparent diffusion coefficient (ADC) values and anisotropic diffusion (q) in DTI owing to myelin degradation and the presence of infiltrates.32 Additionally, DTI fiber tracking can differentiate between pathologies: in tumors, pyramidal tracts appear visibly distorted as they divert around the mass and may show a slight reduction in the representation of fibers; conversely, in demyelinating diseases, tracts are in their normal locations but appear truncated, with a severe reduction in fiber representation and low FA values.35 This technique can also differentiate between primary CNS lymphoma (PCNSL) and TDL.35
One interesting solution to the diagnostic challenge of TDLs is histogram profile analysis of specific ring characteristics from conventional MRI T1WI and T2WI images. This results in the identification of 4 distinct patterns that are subsequently used to distinguish TDL-MS from glioblastomas, with a specificity of 93.3%.36 This method can be used when advanced imaging options are unavailable.
Arterial spin-labeling perfusion has also been successfully used to compare the CBVs between neoplastic and non-neoplastic cases. Considerably higher CBVs were measured in neoplastic lesions than in non-neoplastic lesions both from inside lesions (6.65±4.07 vs 1.68±0.80, p<0.001) and in perilesional edema (1.86±1.43 vs 0.74±0.21, p<0.001).37 There are emerging clinical indications for brain positron emission tomography (PET) in the differential diagnosis of suspected TDLs from primary tumors. Radiolabeled amino acid imaging relies on increased uptake by tumor cells, in contrast to the low background uptake in the CNS, whereas TDLs show mild or absent tracer uptake.38 The TDLs mimicking glioblastoma multiforme or astrocytoma have been distinguished using [11C] methionine PET (MET-PET) and 18F-fluorodeoxyglucose PET,39 wherein TDLs show very little or no uptake of the marker ion, unlike tumors that show high uptake.40,41 Single-voxel proton magnetic resonance spectroscopy (MRS), if available, can also be a sensitive method for differentiating between gliomas and TDLs based on the Cho/NAA ratio. Ikeguchi et al42 calculated the maximum cutoff value for TDLs such that HGGs rather than TDLS were indicated for Cho/NAA ratios >1.72.
Laboratory and histopathological features
The CSF tests are essential for the differential diagnosis of demyelinating autoimmune diseases. Although lumbar puncture is intrusive, it may prevent the need for a biopsy. Glucose levels are usually normal, and white blood cell counts may be slightly elevated, but they have been shown to be significantly higher in TDL patients than those in MS patients. Myelin basic protein levels are moderately elevated.43 A normal to slightly elevated Ig index is expected,5 and positive OCBs have been reported in approximately 30% of biopsy-confirmed TDLs.44 In a retrospective review of clinical features from 17 TDL cases, the median interleukin (IL)-10 and soluble interleukin-2R levels were normal (≤2 pg/mL and <54U/mL, respectively), but IL-6 levels varied and were significantly higher in the TDL and NMOSD groups than in the MS group (5.3 pg/mL and 6.1 pg/mL vs 1.8 pg/mL).43
Negative serum aquaporin 4 antibody (AQP4) has been reported,4,44,45 but Chinese guidelines consider positive serum AQP4 as a supportive criterion for the diagnosis of TDLs.5 We could not find any data to support this criterion, such as the proportion of TDL cases that tested positive for AQP4. However, it may be possible that TDL patients test positive for AQP4 (e.g., when TDL is associated with NMOSD), although this would be an exception rather than the rule. We only found one study that assessed the presence of anti-myelin oligodendrocyte glycoprotein (anti-MOG) antibody Ig in patients with TDL, which was negative in all cases.45 Data from other retrospective studies revealed that anti-MOG testing was rarely performed, despite its association with ADEM, MS, and NMOSD.46 However, MOG testing would be helpful as a positive result would favor an alternative diagnosis to TDL. Histopathological findings include demyelination, active myelin breakdown along the margins, dense inflammatory infiltrates, and activated macrophages.9
Diagnosis
The diagnosis of TDLs is not straightforward, as the clinical and radiological features are often indistinguishable from those of other lesions, such as brain tumors, and there are no internationally accepted consensus criteria. However, Chinese guidelines for the diagnosis and management of TDLs have recently been published.5 These guidelines stipulate that in the absence of a definite histopathological confirmation, all the following criteria should be satisfied for the diagnosis of clinically definite or clinically probable TDL: (1) symptoms persist longer than 24 hours and show progression; (2) MRI (≥1.5 T) shows one or more brain lesions, with at least one of these exhibiting mass effect (although most other studies do not consider mass effect a defining feature of TDLs), with or without edema, and ≥ 2 cm in one direction; (3) predominantly white matter involvement; (4) hypodense or isodense lesion; and (5) clinical, laboratory, and neuroimaging findings cannot be explained by any other CNS lesions or syndromes.5 In situations where a definitive or clinically probable diagnosis of TDL cannot be determined through clinical evaluation and radiological findings, a pathological examination may be required. This is especially true when there is uncertainty in treatment response.
Differential diagnosis
The NMOSD can also be indistinguishable from or occur alongside TDL.14 The presence of optic neuritis, often bilaterally; longitudinally extensive/transverse myelitis; non-specific white matter lesions located in the dorsal medulla, brainstem, and diencephalon; a non-progressive or non-persistent course; and a positive serum AQP4 all indicate NMOSD rather than TDL.47 The ADEM can have the same clinical and MRI features as TDLs, and there have been cases of TDL coexisting with MOG-positive ADEM.13,48,49 The main differences to look for are lesions in the gray matter (thalamus, basal ganglia), bi-hemispheric and simultaneously enhancing lesions, positivity for anti-MOG antibodies, high white blood cell count (>50/μL, but unspecific) in the CSF, and increased albumin levels, all of which favor a diagnosis of ADEM.13 Additionally, the rare condition BCS can easily be misdiagnosed as TDL, especially if the concentric rings of demyelination and myelin are not clearly evident on conventional T1/T2 MRI images15 or if the rings merge to form large plaque-like lesions, as seen in older lesions.50 Typically, in BCS, the ADC values in the center of the lesion are high, with restricted diffusion in the outermost ring occurring over time.51 The visibility of concentric rings is more apparent on DWI and diffusion coefficient maps, where areas of active demyelination show high intensity (restricted diffusion) and normal myelinated areas show low intensity (facilitated diffusion).50,52 This could be a reliable, noninvasive characteristic for distinguishing BCS from TDL, at least during the acute stage.
Treatment and prognosis
The first-line treatment for TDLs is corticosteroids (e.g., methylprednisolone, 1000 mg/day) administered intravenously for 3-5 days and thereafter tapered orally.5,6,53 Corticosteroids are generally effective and decrease the lesion size in 45%6 to 80%54 of cases, with a corresponding decrease in the EDSS score. However, not all patients respond well to corticosteroids, and some are left with partially resolved lesions, possibly because of large lesion size combined with a relatively short course of therapy. To support a more complete lesion resolution and reduce the risk of relapse, the Chinese guidelines recommend a very slow tapering-off regimen as follows: a 50% reduction in the dose at each step, administered for 2-3 days (i.e., 500 mg for 2-3 days, followed by 250 mg for another 2-3 days, and so on), switching to oral prednisolone at a dosage of 40 mg, and continuing a very gradual weekly reduction (from 40 mg to 32 mg, then 28 mg, and so on).5
If steroids are contraindicated or ineffective, other commonly prescribed alternative medications for acute TDLs are PLEX, cyclophosphamide, and rituximab.6,18 The PLEX can be beneficial for any steroid-resistant demyelinating disorder of the CNS, but it is particularly effective in resolving NMO.55 Interestingly, an association was found between ring enhancement of the largest lesion, associated with mass effect and edema (as is often seen in TDLs), and the PLEX response.55 The PLEX was effective in treating particularly aggressive multiple TDLs in a patient who was unresponsive to 10 days of IV steroids.56 A PLEX response is more likely when there is a short disease duration, RRMS (compared to other IDDs), negative NMO Ig in NMOSD,55 and preserved tendon reflexes.57
In a study comparing treatment options for TDLs, glatiramer acetate was the only treatment, apart from steroids, associated with a decrease in lesion size in 57% of patients; however, the improvement in EDSS score was transient, and there was no long-term follow-up over 1 year.6 Cyclophosphamide has been successful in treating TDL in a few cases, but there is currently a lack of evidence supporting its use for TDLs. Natalizumab has also been reported as a potential therapy.6 However, because of recent cases in which natalizumab treatment for MS was followed by the formation of TDLs,24,26 its use may be contradictory. Fingolimod use is contraindicated in cases of tumefactive-MS because of the cases of TDLs associated with fingolimod use..17,19–25
In a study of 57 cases of MS with atypical presentation, the overall risk of conversion to MS after an isolated TDL was approximately 30% at 5 years;46 however, other studies have reported much higher proportions of conversion at 67%18 and 81%.54 Interestingly, cases of TDLs that later converted to MS showed good prognosis, with a median EDSS score of 1.46 Positive OCBs on TDL may be associated with a higher probability of conversion to MS.54
Conclusions
Diagnosis of TDL remains challenging despite an increase in available information and advances in imaging not only because of the nonspecific clinical and radiological findings in TDL, but also because TDL can co-exist with one of several other disease entities (e.g., ADEM, BCS, and NMOSD).5,14,15,48 The pathogenesis of TDL may share a common underlying cause with MS and other conditions.14 Misdiagnoses of MS spectrum disorders are common, and one multicenter study confirmed that approximately 30% of misdiagnosed patients experience unnecessary morbidity.58
Compared with other MRI features, open ring rim enhancement for the diagnosis of TDLs has considerable variation in sensitivity (27%–71%) but has the highest specificity (98%–100%).9 Conventional MRI for differentiating TDL from primary brain tumors has a sensitivity of 89% and a specificity of 94%.9 The use of DSC with MRI is highly recommended for the diagnosis of TDL.9,32,33 When findings from MRI and rCBV values are inconclusive, DSC combined with DTI can increase the sensitivity for distinguishing TDLs from tumors owing to their differing effects on nerve fiber pathways and their representation.32 Cases that require differentiation between TDLs and HGG/PCNSL may benefit from the use of MET-PET, FDG-PET, or proton MRS.39–42
Randomized controlled trials comparing commonly used treatments for TDLs with dosages and durations consistent with the most favorable outcomes in patients, with a long-term follow-up are needed. Corticosteroids, PLEX, glatiramer acetate, and cyclophosphamide are beneficial in TDL,6,18 but the use of the MS therapies natalizumab and fingolimod is contradicted because of the potential for worsening or development of new TDLs.24,26 Regular follow-ups are necessary during the diagnostic work-up owing to the possibility of one MS spectrum disorder evolving into another.
Acknowledgments
We would like to thank Editage (www.editage.com) for English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.