


Neurological manifestations of acute leukemia are due to direct involvement by meningeal infiltration and myeloid sarcoma; and indirect involvement by immunosuppression and treatment related side effects. It is rare for myeloid sarcoma to present without bone marrow involvement (isolated myeloid sarcoma or primary granulocytic sarcoma).1 It is even rarer for an isolated myeloid sarcoma to present in the epidural space. We evaluated a case of paraplegia admitted to our department. He had several atypical features that we would like to present in this report.
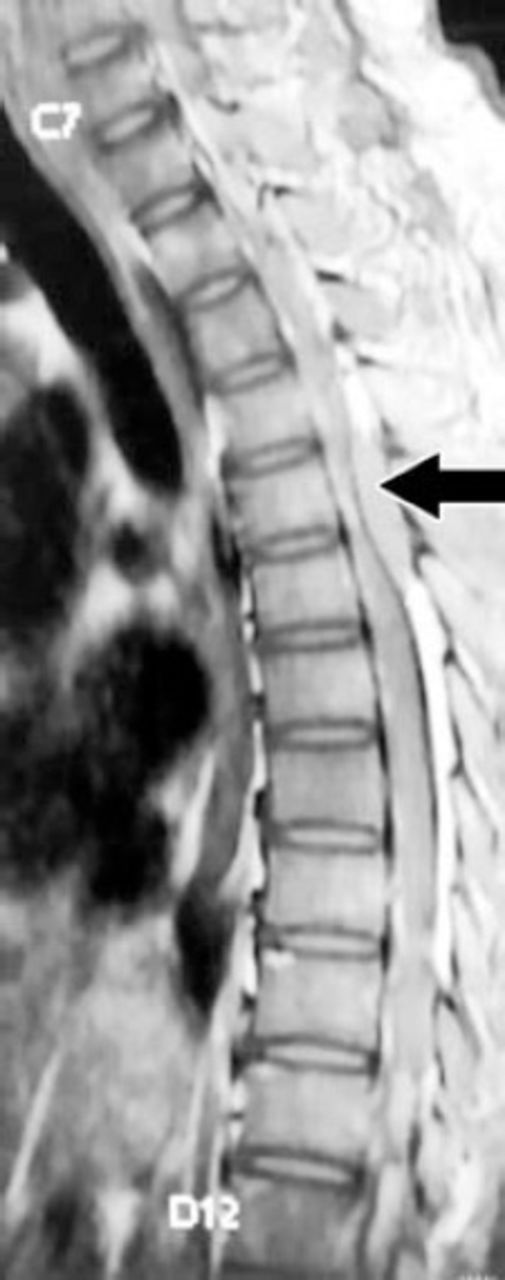
A 39-year-old gentleman with a body weight of 58 kg presented with paresthesia and heaviness of both lower limbs of 4 days duration. He was found to have spastic paraplegia with bladder involvement and sensory level at T6. The clinical diagnosis of acute transverse myelitis was made. Table 1 summarizes the laboratory investigations. The MRI study of the dorsal spine (Figure 1) shows that a moderate sized enhancing posterior epidural component was compressing the thecal sac and spinal cord. Further work-up was carried out suspecting multiple myeloma/plasmacytoma. The peripheral blood picture showed dimorphic anemia, occasional large cells with granular cytoplasm and nucleus with condensed chromatin, and no blast cells. Ultrasound of the abdomen showed mild splenomegaly. Urine Bence Jones protein was absent. No M band was seen on serum protein electrophoresis. Bone marrow aspirate showed many large cells with abundant granular cytoplasm and some of them had multilobed nucleus probably mast cells. Bone marrow trephine biopsy showed normal cellularity, no plasmacytosis, or excessive blast cells. Clusters of cells were seen with abundant granular cytoplasm and vesicular nucleus. Immunohistochemistry showed 2 clusters of cells (20-22 cells per cluster), densely positive for CD117, with similar cells diffusely infiltrating the marrow. The cells tested negative for myeloperoxidase (MPO). Bone marrow findings were suggestive of mastocytosis and no evidence of leukemia or myeloma. He was started on steroids, and antihistamines. He was referred to neurosurgery for management of the extradural space occupying lesion. A T4-T9 laminectomy was carried out, and the epidural mass removed. The histopathology report showed myeloid sarcoma, possibly myelomonocytic type with mast cell proliferation (MPO positive, CD 117 positive in large cells, CD 68 positive, CD 34 negative, CD 56 negative, CD 33 inconclusive). A final diagnosis of compressive myelopathy due to isolated epidural myeloid sarcoma and systemic mastocytosis with associated clonal hematological non mast cell lineage disease (SM – AHNMD) was made. After removal of the epidural mass he showed minimal improvement of muscle power in the lower limbs from Medical Research Council grade 1 to 2. He was started on chemotherapy for acute leukemia with cytarabine and daunorubicin. After completing the first course of chemotherapy for one week, his blood counts dropped and he continued to have fever. He was started on antibiotics; but succumbed to illness probably secondary to sepsis on the fourteenth day after starting chemotherapy.
Laboratory investigations in a patient with the clinical diagnosis of acute transverse myelitis.

Magnetic resonance imaging of thoracic spine T1W sagittal view, arrow showing extradural mass at T6 level.
Mastocytosis is a rare disorder characterized by excessive mast cell accumulation in one or multiple tissues. Mastocytosis is subdivided into 2 groups – cutaneous mastocytosis (CM) and SM. Systemic mastocytosis describes forms of mastocytosis in which mast cells infiltrate extracutaneous organs, with or without skin involvement. It includes 4 distinct disorders – indolent systemic mastocytosis, SM-AHNMD, aggressive systemic mastocytosis, and mast cell leukemia. Our patient was detected to have SM-AHNMD. It is the second most common variant of SM (around 30% cases).2 The prognosis is determined by the nature of the associated disorder.
Myeloid sarcoma is a tumor mass consisting of myeloid blasts with or without maturation, occurring at an anatomical site other than bone marrow. It can occur de novo or may precede or coincide with acute myeloid leukemia (AML); common sites being lymph nodes, skin, leptomeninges and subperiosteal bone structures of the skull, paranasal sinuses, sternum, ribs, vertebrae, and pelvis.3 The pancreas, heart, brain, mouth, breast, gastrointestinal and biliary tract, prostate, urinary bladder, and gynecologic tract are the other sites reported, though rare. Detection of myeloid sarcoma should be considered equivalent to a diagnosis of AML.4 The definitive diagnosis of myeloid sarcoma was made by immunohistochemistry. Though many antibodies can be positive in myeloid sarcoma, MPO, CD117, and CD68 are present in common variants of myeloid sarcoma. Other common markers are lysozyme, CD34, CD45, and CD43. The common mutation associated with myeloid sarcoma is t (8; 21) (q22; q22) and there are reports that SM is associated with this mutation.5 The immunohistochemistry was suggestive of myeloid sarcoma in our patient, and karyotyping of patient was not carried out. Treatments include relieving compression by removal of mass, chemotherapy for AML, and general measures to prevent allergic reactions and anaphylaxis due to mast cell degranulation; antihistamines, anti-leukotriene agents, and tyrosine kinase inhibitors.
Our patient presented with acute paraplegia. He was found to have SM and an extradural mass that turned out to be myeloid sarcoma without features of AML. We performed a MEDLINE search using the words “myeloid sarcoma, systemic mastocytosis with an associated hematologic non-mast cell lineage disorder, systemic mastocytosis, isolated epidural myeloid sarcoma, and primary granulocytic sarcoma”. Case series and case reports of isolated myeloid sarcoma were found - a recent case series of isolated myeloid sarcoma showed 15 cases over a period of 5 years in a single hematology centre;1 only 11 cases of isolated epidural myeloid sarcoma were reported in the last 10 years; but there was no result showing a combination of isolated myeloid sarcoma with SM.
In conclusion, this case is reported to highlight 2 facts: 1) Myeloid sarcoma can present without bone marrow involvement, and it may occur in the epidural space causing compressive myelopathy. 2) Isolated myeloid sarcoma can be associated with SM and the association is very rare. This is an unusual presentation of a rare disease.
Acknowledgments
We thank the Department of Neurosurgery and Department of Radiotherapy, Government Medical College, Thrissur for their valuable assistance. We also thank Dr. Brahmadathan, Professor of Radiodiagnosis, Government Medical College, Thrissur for reviewing the MRI figure for its clarity and correctness.
Footnotes
Disclosure
The authors declare no conflicting interests, support or funding from any drug company.
- Received February 27, 2014.
- Accepted May 29, 2014.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.