


Abstract
Cerebral venous sinus thrombosis (CVST) rarely induces cerebral hemorrhage, and CVST with cerebral hemorrhage during early pregnancy is extremely rare. Upon literature review, we are able to find only one case of CVST with cerebral hemorrhage in early pregnancy. In this paper, we report another case of a 27-year-old patient who developed CVST with cerebral hemorrhage in her fifth week of pregnancy. Although the optimal treatment for this infrequent condition remains controversial, we adopted anticoagulation as the first choice of treatment and obtained favorable results.
Cerebral venous sinus thrombosis (CVST) accounts for 0.5-1.0% of all strokes.1 During late pregnancy and puerperium, CVST is an uncommon but important cause of stroke.2 Hemorrhagic infarction can occur in the acute stage of CVST. However, CVST with cerebral hemorrhage is extremely rare in early pregnancy. Upon literature review, we are able to find only one case of CVST resulting in cerebral hemorrhage in early pregnancy.3 Here, we present another case of CVST with cerebral hemorrhage in early pregnancy, the patient received a favorable outcome by use of anticoagulation therapy. Our objective in presenting this particular case is to discuss its diagnosis, and treatment, and review the related literature.
Case Report
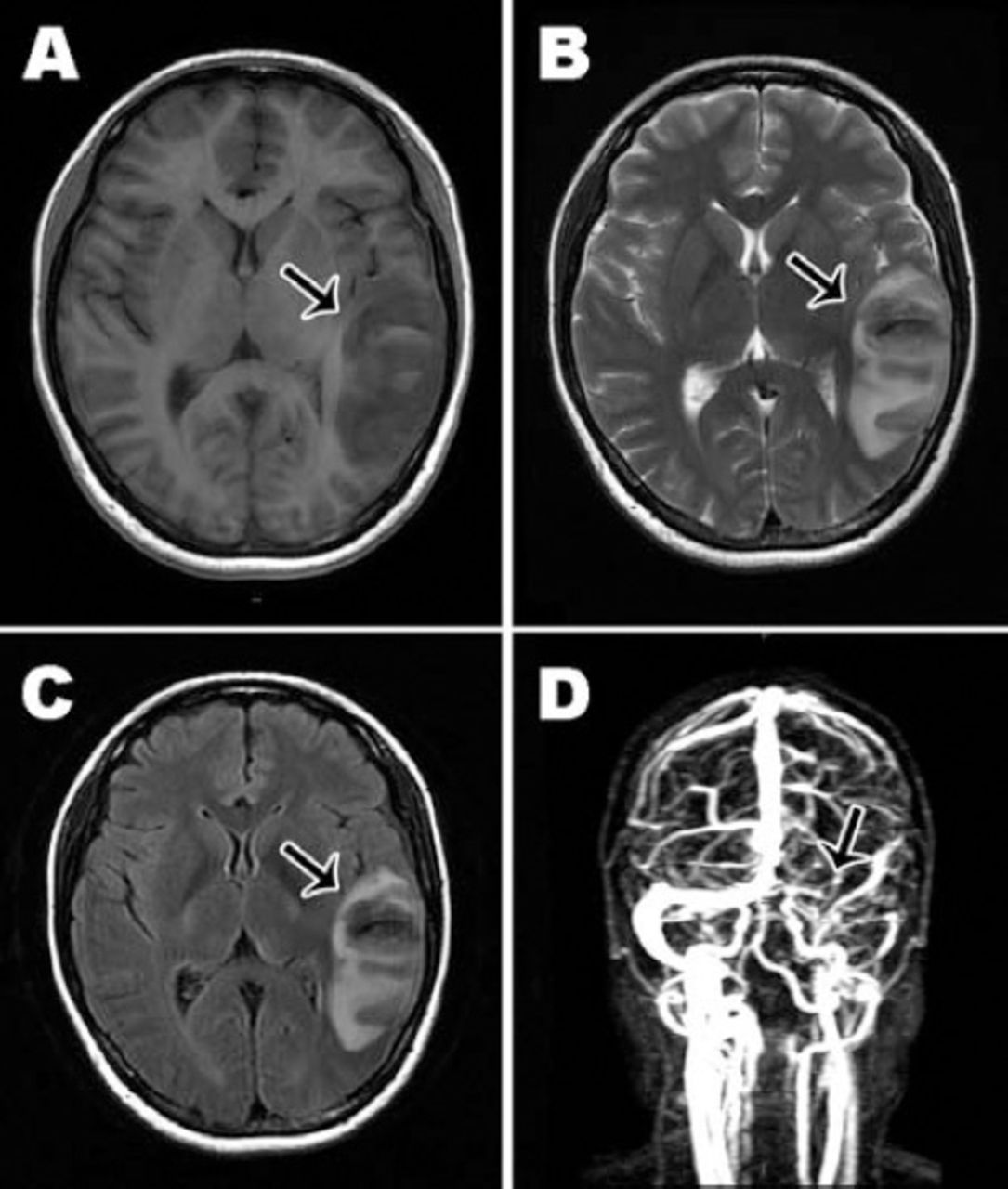
A 27-year-old woman presented with acute onset of severe diffuse headache for one day and slurred speech for 4 hours. She was 5 weeks into her second pregnancy. She had not previously been on contraceptive pills, and did not have any personal or family history of venous thrombosis, autoimmune disease, or hematologic disease. She was fully conscious and afebrile, with no focal neurological deficits. Laboratory examination showed a normal complete blood count and normal renal, hepatic, and coagulation profiles. Urgent brain CT revealed temporal hemorrhage surrounded by an extensive hypodense area (Figure 1). Therefore, tumor apoplexy or cerebrovascular disease was suspected. An MRI using a 3.0 T scanner revealed a hyperintense lesion surrounded by a large hypointense area on T1-weighted images (Figure 2A), and a hypointense lesion surrounded by a large hyperintense area on T2-weighted and fluid-attenuated inversion recovery (FLAIR) images (Figures 2B & 2C). After administration of gadopentetic acid dimeglumine salt, no obvious contrast enhancement was seen on T1-weighted images. Magnetic resonance venography (MRV) showed that the left transverse and sigmoid sinuses were completely occluded (Figure 2D). A brain digital subtraction angiography (DSA) confirmed thrombosis of the left transverse and sigmoid sinuses with engorgement of the superficial veins in the left hemisphere (Figure 3), but was negative for vascular malformations such as aneurysm, arteriovenous malformation (AVM), and dural arteriovenous fistula. Transvaginal sonography revealed an early intrauterine pregnancy, the gestational sac was 5×5×5 mm in size, and the fetal germ, or fetal heart could not be detected. A CVST with cerebral hemorrhage was diagnosed according to clinical data. To control intracranial hypertension, treatment with mannitol was commenced immediately, and dose-adjusted low-molecular-weight heparin (9600 units/day for 10 days) was started 3 days after the onset of CVST to maintain activated partial thromboplastin time between 1.5 and 2.0 times of control value. When a repeat CT showed that the cerebral hemorrhage had regressed, heparin was substituted with oral warfarin. Abortion was also performed 20 days after the onset. Two months later, MRV showed recanalization of the left transverse and sigmoid sinuses (Figure 4), and remained asymptomatic in the following years.

Computed tomography (CT) upon admission. Non-contrast axial scan reveals temporal hemorrhage surrounded by a large hypodense area.
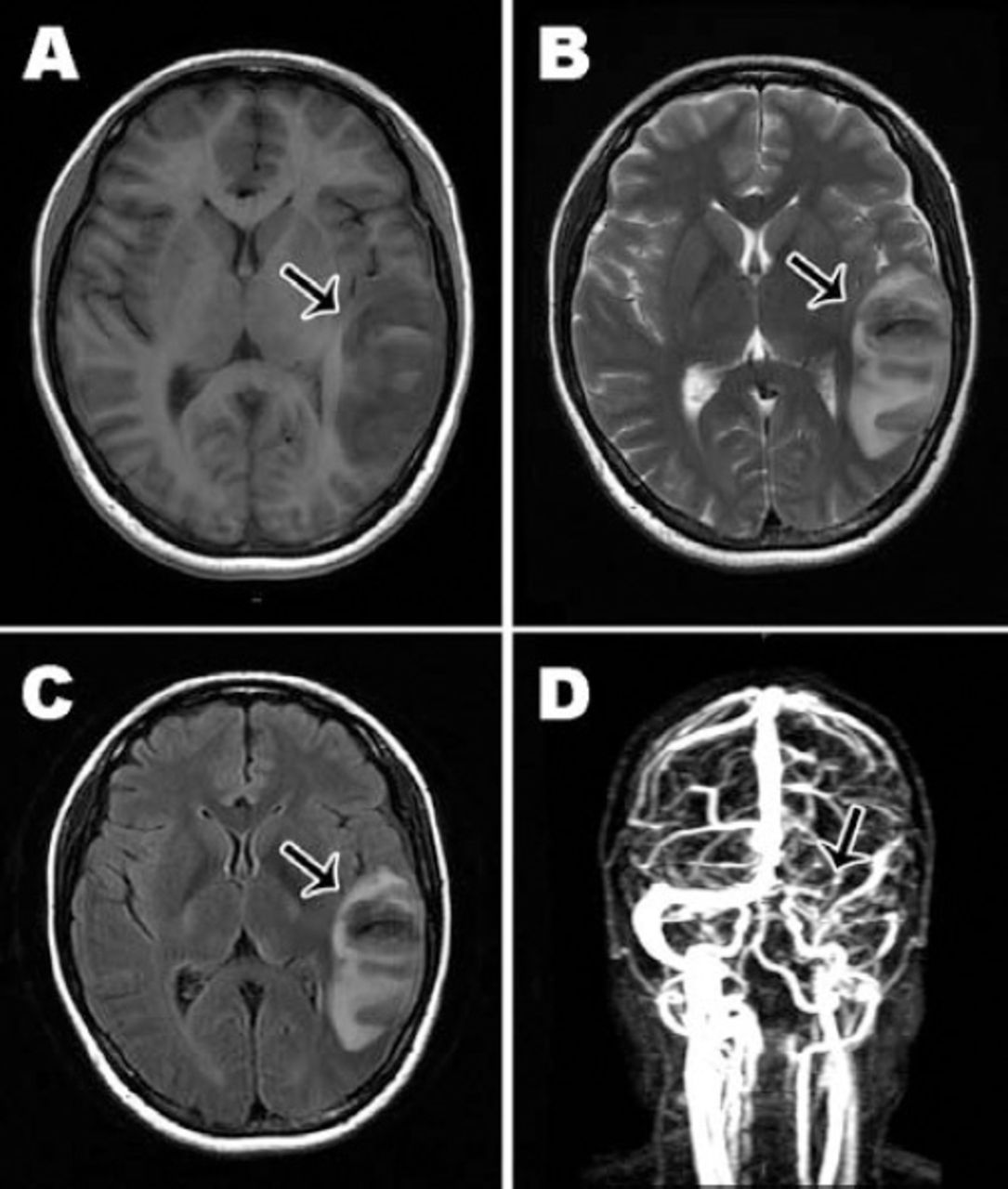
Magnetic resonance imaging (MRI) and magnetic resonance venography (MRV) upon admission showing: A) The lesion appears hyperintense surrounded by a large hypointense area on T1-weighted MRI, B) hypointense surrounded by a large hyperintense area on T2-weighted MRI, C) fluid-attenuated inversion recovery MRI. D) MRV shows complete occlusion of the left transverse and sigmoid sinuses.
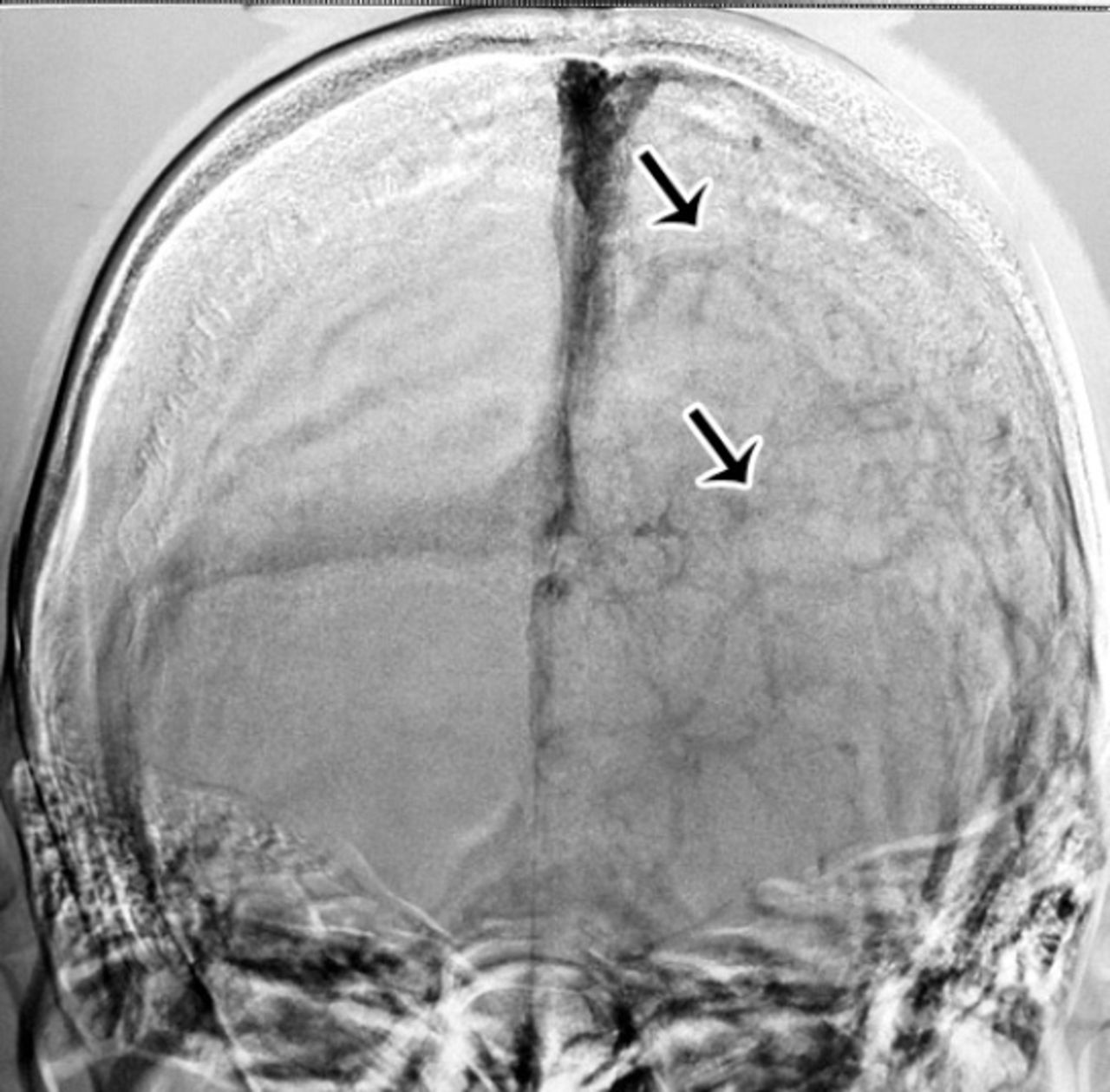
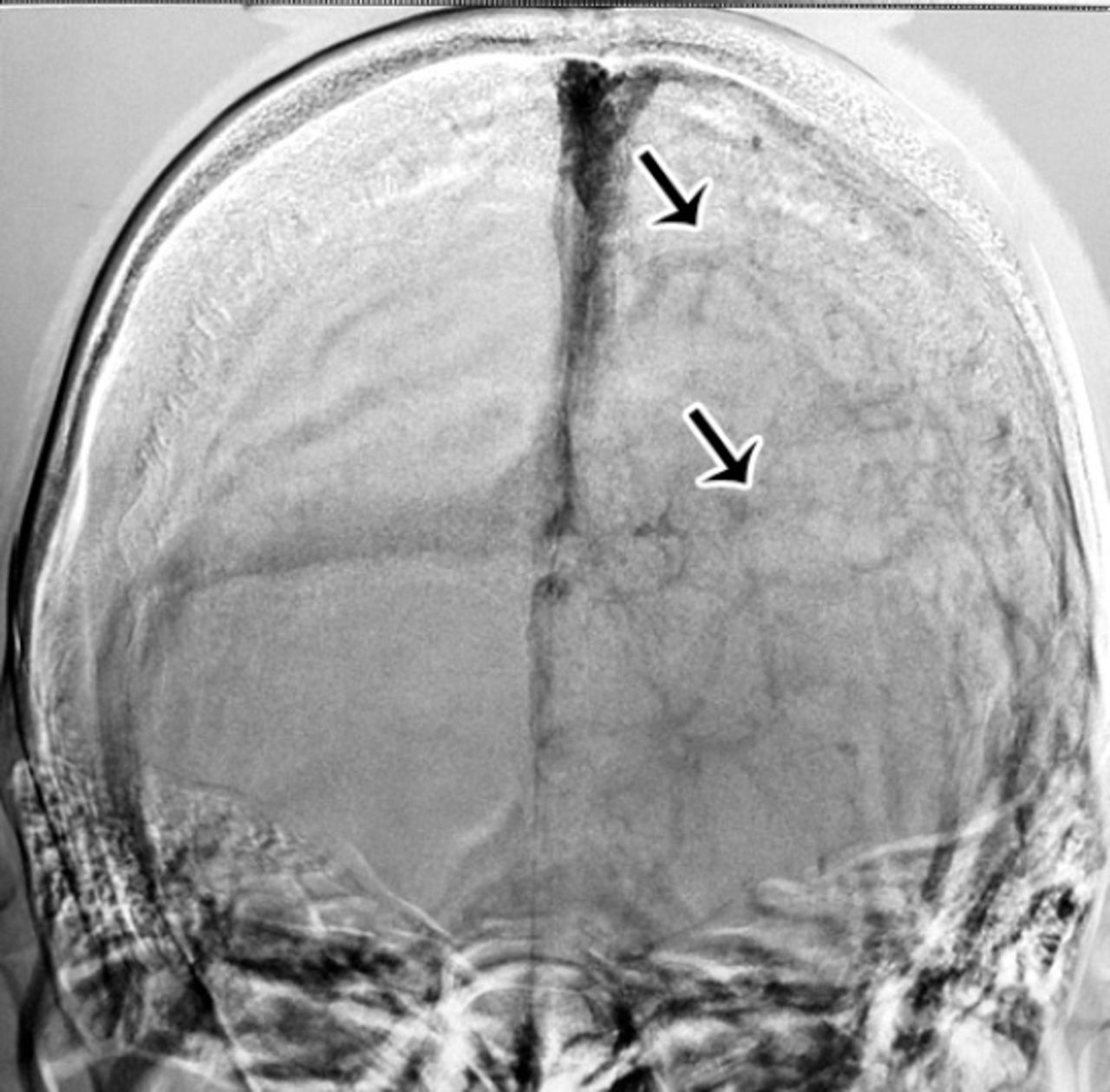
Digital subtraction angiography (DSA) upon admission. Anteroposterior view reveals complete thrombosis of the left transverse and sigmoid sinuses as well as engorgement of the superficial veins in left hemisphere.
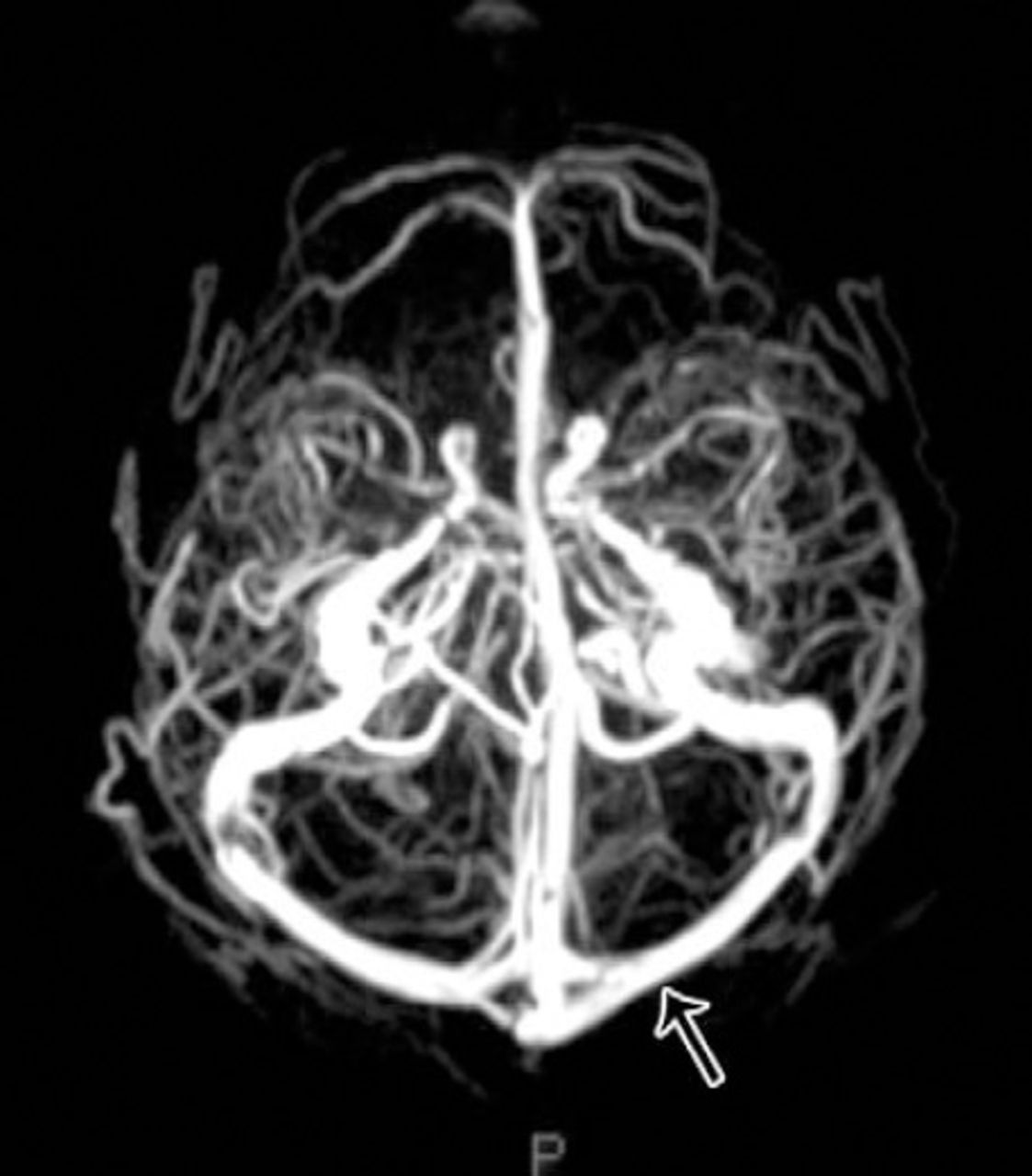
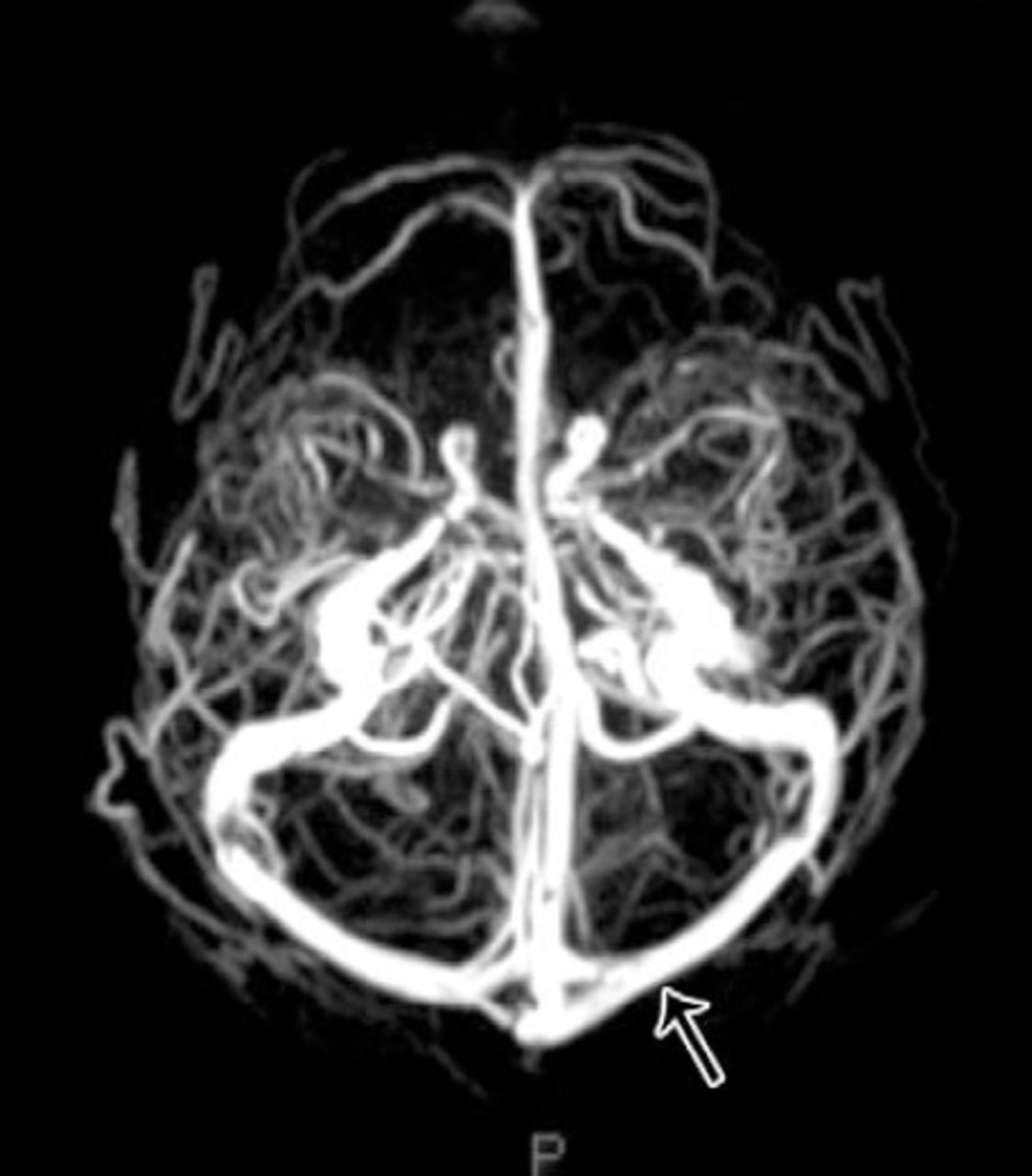
Follow-up magnetic resonance venography (MRV) at 2 months after treatment. Axial view shows recanalization of the left transverse and sigmoid sinuses.
Discussion
A CVST is an uncommon but serious neurological emergency, the overall death, and dependency rate are approximately 10-15%.4 Pregnancy and puerperium induces changes in the coagulation system, increasing the risk of CVST. The period of greatest risk for CVST includes the third trimester of pregnancy, and the first 4 postpartum weeks.5 Only a few cases of CVST in early pregnancy have been reported.3,5,6-8 A CVST with cerebral hemorrhage in early pregnancy is extremely rare, Lavin et al3 reported the first case of CVST with cerebral hemorrhage at 8 weeks of pregnancy, the patient died because of massive cerebral venous infarction with edema.3
The clinical manifestations of CVST are non-specific. The most frequent symptoms are headache, seizures, neurological deficit, and decreased level of consciousness.9 Signs of cerebral hernia can appear in patients with mass effects, such as edema, infarction, and hemorrhage. Because of the wide spectrum of symptoms and signs of CVST, it can be difficult to arrive at the correct diagnosis based on clinical assessment alone.
Imaging findings are very important in the diagnosis of CVST. Hemorrhage, edema, and infarction can be detected on CT, a hyperdense lesion can be found occasionally in the venous sinus indicating thrombosis. However, CT is detrimental for pregnant women due to the radiation involved. An MRI can differentiate CVST from tumor apoplexy, and MRV can reveal sinus occlusion. Cerebral angiography is invasive and involves radiation; however, this method allows the detection of sinus thrombosis. Other vascular abnormalities such as aneurysm, arteriovenous fistula, and AVM can also be excluded by DSA. An MRI and MRV are non-invasive and do not involve radiation, we therefore, consider that the combination of MRI and MRV is the best choice for the investigation of suspected CVST in pregnant women.
The CVST is an increasingly recognized neurological emergency. There have been no large trials of anticoagulation in pregnancy, and recommendations are based on case series and the opinions of experts. Nonetheless, anticoagulation is believed to be beneficial for patients with CVST and hemorrhagic complications. Among 29 patients with intracranial hemorrhage and CVST treated with low-molecular-weight heparin (180 anti-factor Xa units/kg/day for 3 weeks), de Bruijn et al10 reported 6 deaths, none of which were attributable to fresh or exacerbated cerebral hemorrhage. Although the best time to start anticoagulation treatment is not known, repeating CT or MRI to confirm that the intracranial hemorrhage is regressing or at least not progressing is advisable before starting anticoagulation. The use of local thrombolysis for CVST was first reported by Weatherby8 in 2003, who achieved a successful outcome in a patient who developed CVST in early pregnancy. The use of endovascular treatment for CVST should be considered in patients who are resistant to anticoagulation therapy, have worsening symptoms, do not have intracranial hemorrhage, and are not at risk for impending herniation.11 Decompressive hemicraniectomy could be life-saving and even lead to an excellent outcome in CVST patients with impending transtentorial herniation because of large hemorrhagic venous infarcts.12 In patients with CVST in early pregnancy, early management of the embryo to eliminate the triggered spontaneous coagulation might also contribute toward recovery.5
In conclusion, CVST with cerebral hemorrhage can occur in early pregnancy. Its clinical manifestations are non-specific. An MRI combined with MRV may be the best choice for the investigation of a suspected CVST in a pregnant woman. Anticoagulation therapy may be beneficial in curing CVST, even in pregnant patients with intracranial hemorrhage. In our patient, anticoagulation was successful when administered 3 days after the onset of the disease.
Footnotes
Disclosure
The authors declare no conflicting interests, support or funding from any drug company.
- Received February 12, 2014.
- Accepted August 19, 2014.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.