


Abstract
Cervical arterial dissection (CAD) is a common cause of stroke in young people which can be classified as either spontaneous or traumatic. The primary initial symptoms are headache, neck pain, and dizziness. Recently, a 57-year-old woman experienced a severe headache after using a cervical neck traction device. Radiological examination of the head and neck revealed right vertebral artery dissection, which emphasizes the importance of recognizing that using cervical neck traction devices increases the risk of traumatic vertebral artery dissection.
Headache is a frequent cause for people to seek medical attention. While most headaches are benign and caused by primary headache disorders, there is a significant overlap in symptoms with secondary headaches.1 Arterial dissection in the neck is one of the secondary causes of headache and can occur when one or both paired extra-cranial carotid or vertebral arteries are involved.2 Vertebral artery dissection is a rare but potentially dangerous condition that can cause a stroke, it is more commonly seen in patients under the age of 45.3 The initial symptoms include headache, neck pain, and dizziness which are caused by the release of pro-inflammatory neurotransmitters from nerve terminals.4 Other complications include transient ischemic attack or ischemic stroke and partial Horner’s syndrome.2 This condition can be triggered by minor trauma such as neck distortion caused by chiropractic manipulation, bending of the neck, or blunt trauma, although spontaneous dissections have also been reported.3 A crucial part in risk factor detection, early diagnosis, and subsequent care is played by physiotherapists. Physiotherapists play a fundamental role in risk factor identification, early diagnosis, and subsequent management.5
Case Report
Patient information
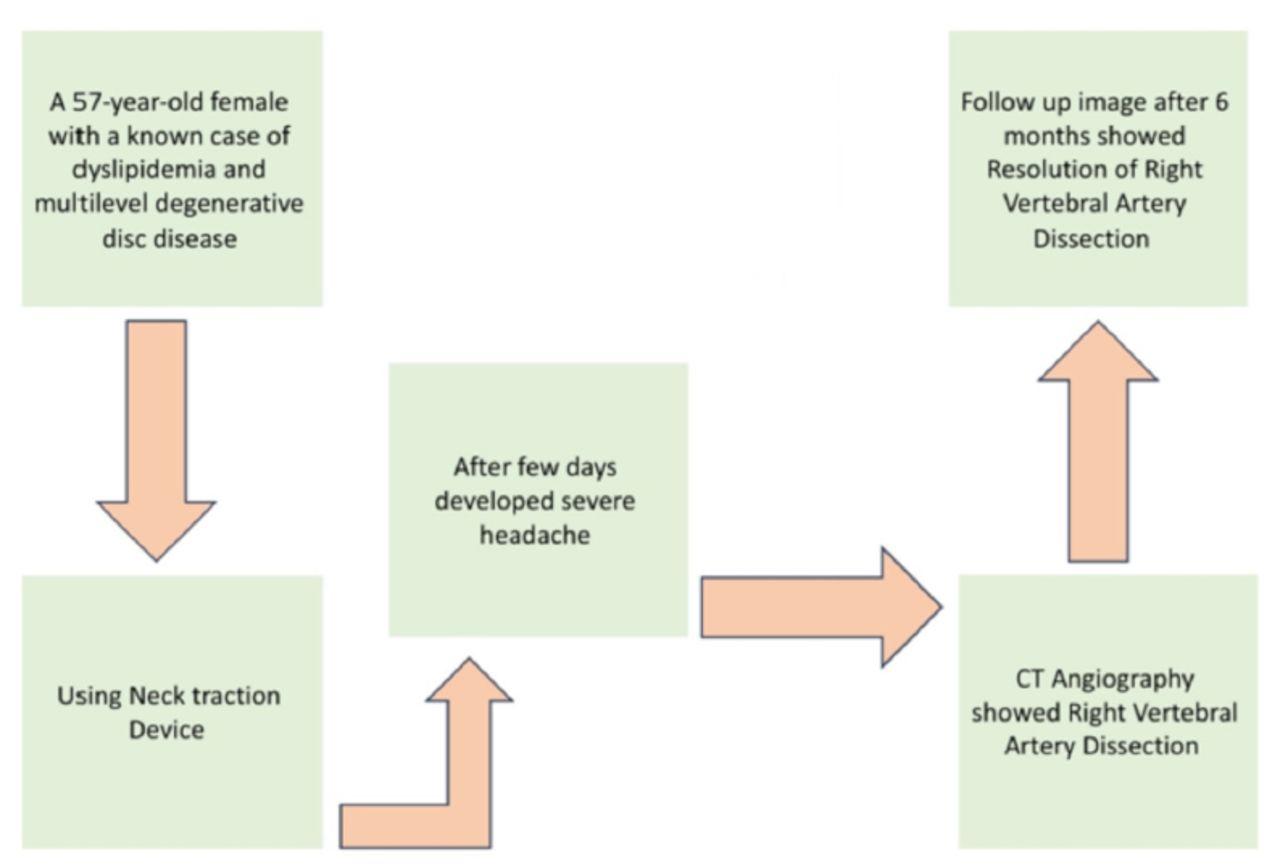
The patient is a 57-year-old female known to have dyslipidemia and multilevel degenerative disc disease C5-C6 and C6-C7; she presented to the emergency department with a one-week history of severe headaches. As the patient had a degenerative disc, she was watching videos on YouTube about some exercises to reduce the pain. There was an advertisement for a neck traction device (Figure 1) as it helps with a neck massage and reduces the pain, so she ordered it from the website and started to use it by lying down and keeping the neck on the device, and perform some maneuvers and exercise for 10–15 minutes, a few days after using the device the patient developed a headache which gets increase over time. She presented to the hospital after one week when it became intolerable. The headache was located on the right side, mainly over the frontal and occipital area, had an insidious onset, was throbbing in nature, radiated to the right side of the neck, and was not associated with any other symptoms. Further, it was severe (9/10), continued the whole day, increased when the patient lay down, lasted 4–5 hours, and was partially relieved by simple analgesia. There was no change in the patient’s level of consciousness, no visual symptoms, no nausea or vomiting, and no photophobia or phonophobia. Moreover, there were no other neurological symptoms (Figure 2, timeline).

- Neck traction device.

- Timeline of a 57-year-old female known to have dyslipidemia and multilevel degenerative disc disease C5-C6 and C6-C7; she presented to the Emergency Department with a one-week history of severe headaches.
Clinical findings
Normal mental functional status. Cranial nerves revealed equal bilateral reactive pupils, with normal extra-ocular movements, visual field, and fundus exam; visual acuity was 20/20, the facial sensation was intact, and there was no facial asymmetry. Motor exam revealed no drift, normal tone with power of 5/5, and +2 reflexes at all extremities. The sensory exam was intact to all modalities (light touch, pinprick, vibration, joint position, and temperature). Coordination and gait were normal.
Diagnostic assessment
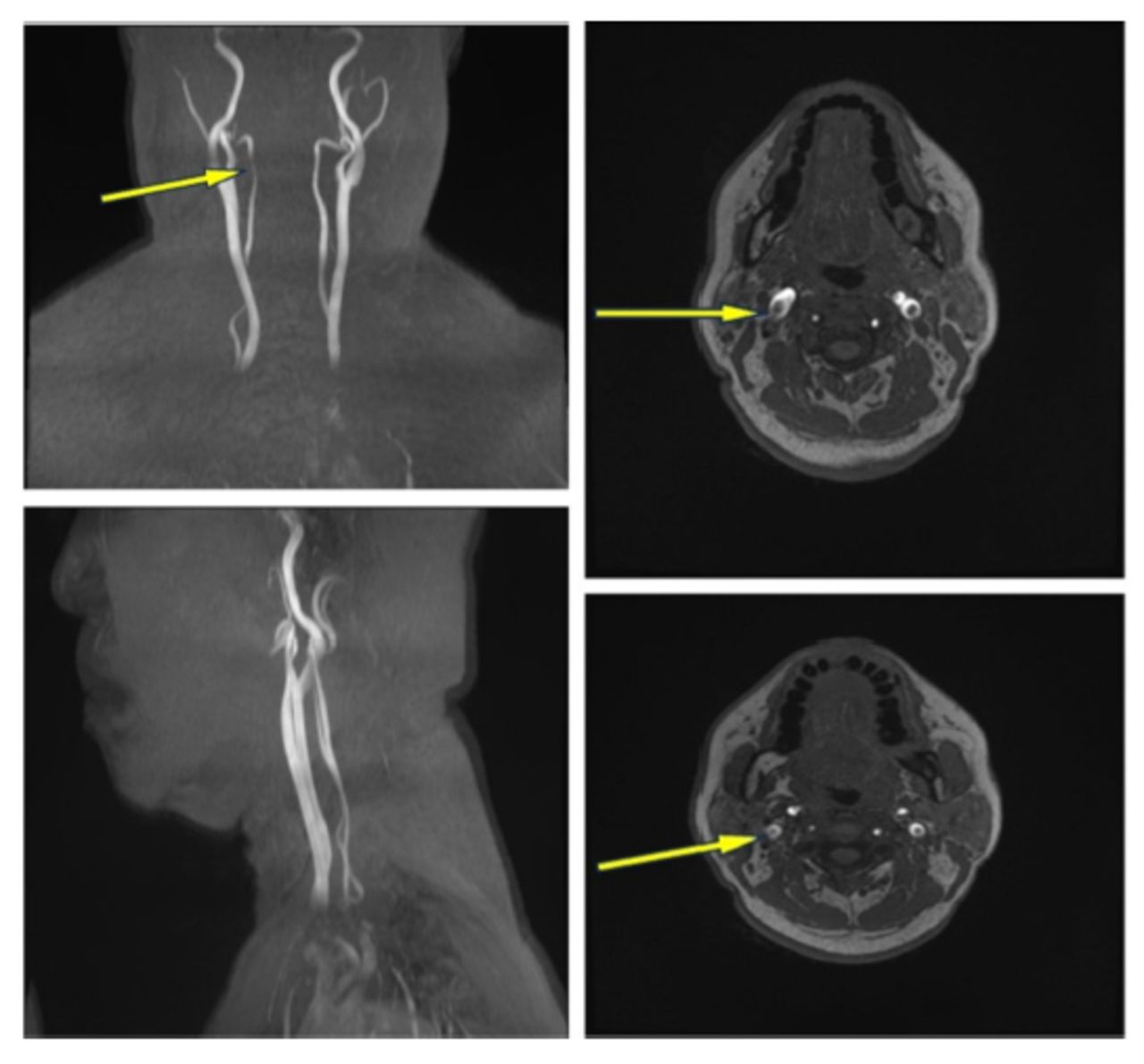
Upon presentation to the emergency department along with a headache, she complained of neck pain, so the patient underwent a brain Computed Tomography (CT) and Computed Tomography Angiography (CTA) to look for secondary causes of the headache; the images showed 2 areas of narrowing separated by a small focal dilatation of the right vertebral artery (possible dissection) (Figure 3-A).

- Shows A) CT angiography, B) MR angiography
On admission, a brain Magnetic Resonance Image (MRI) and Magnetic Resonance Angiography (MRA) were carried out to confirm the diagnosis, and it showed focal narrowing in the V4 segment of the right vertebral artery and an adjacent crescentic area of high T1 and low-to-intermediate T2 signal intensity with blooming on Short Tau Inversion (STIR) stability waiting imaging, this was consistent with the dissection within intramural hematoma (Figure 3B).
Therapeutic intervention
After confirming the diagnosis of right vertebral artery dissection, the patient was started on a single antiplatelet (aspirin 81mg daily) and to control risk factors for secondary stroke prevention.
Follow-up and outcomes
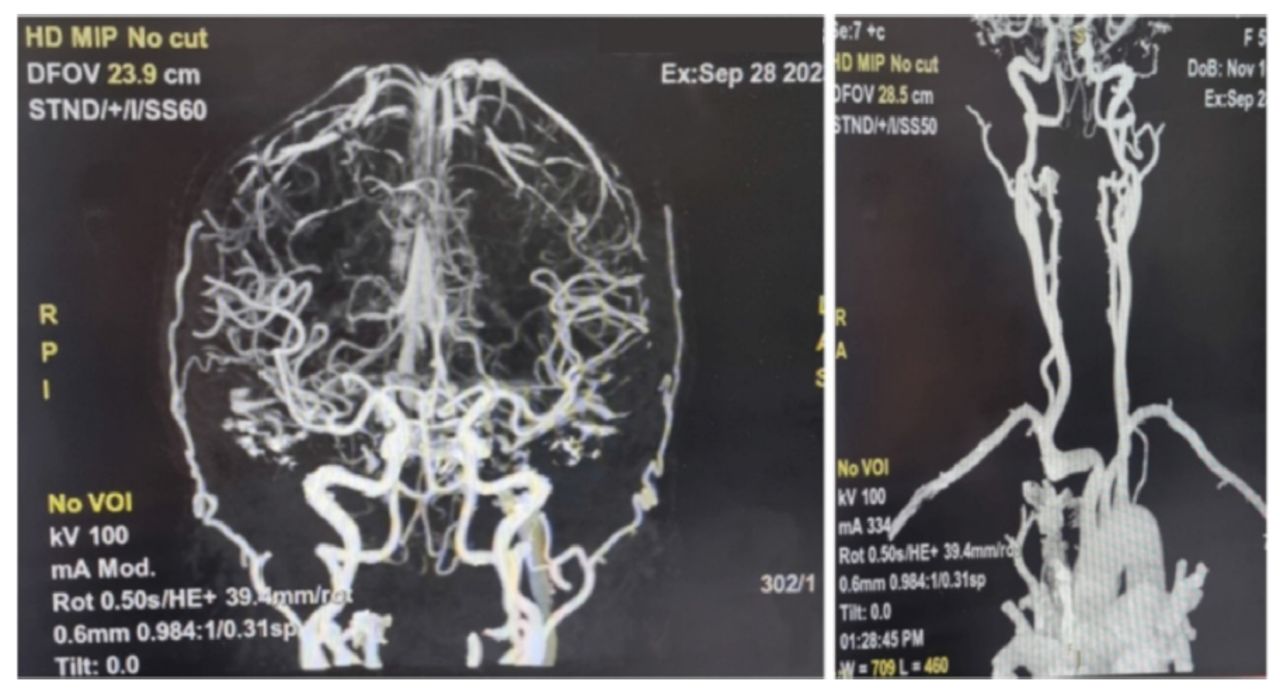
The patient’s condition improved, and her headache decreased as it responded well to analgesia. Moreover, no focal neurological deficits had developed. The follow-up image after 6 months showed no evidence of right vertebral artery dissection, which indicates interval resolution (Figure 4). The patient was instructed to continue antiplatelet and to control risk factors.

- Follow up CT angiography after 6 months (resolution of dissection).
Discussion
We have presented a case report of a patient with vertebral artery dissection, who was experiencing severe headache and neck pain. The dissection was caused by a minor trauma resulting from the use of a cervical neck traction device for neck pain. An old case report published by R. Dickerman in 2005 suggests that vertebral artery dissection can occur as a result of traction in cervical spine surgery.
Arterial dissection is a condition that can affect the carotid or vertebral arteries. It is caused by damage and injury of the arterial wall layers. In some cases, it can occur spontaneously, while in others, a minor head or neck injury may serve as the triggering event.6 Obtaining a detailed history can help identify unusual and rare causes of traumatic vertebral artery dissection, as evidenced by the findings of various case reports and literature reviews.
Dissection occurs due to forceful trauma, chiropractic manipulation, or neck bending, as reported by Britt, T.B.3
According to a case study conducted by Kolberg C.7 a chiropractic session resulted in a significant fracture of the C5-C6 vertebrae. This fracture was found to be associated with serious medical complications, including cerebellar infarction, spinal cord injury, and vertebral artery dissection.
Chiropractic manipulation can cause several neurologic disorders, including acute disk herniation, epidural hematoma, and spinal artery dissection.8
It’s important to be aware that certain physical activities like sports, exercises, maneuvers, massages, and equipment can cause mild damage that may result in vertebral artery dissection.
A case report published by SulkowskI K9 revealed that a 27-year-old woman who had been experiencing headaches, neck pain, and dizziness was diagnosed with vertebral artery dissection. The cause was attributed to repeated usage of a handheld massager.
Cervical artery dissection is characterized by common symptoms such as headache, neck pain, and dizziness. The headache comes on suddenly and is moderate to severe, feeling like a pulsating or throbbing sensation. It is important to differentiate this type of headache from primary headaches and to be aware of headache red flags.
Cervical artery dissection is a significant cause of stroke in younger individuals, and symptoms can manifest several days after the initial dissection. Early detection is critical to prevent stroke and mitigate long-term neurological damage. The current recommendation is to use aspirin to prevent subsequent stroke, which is based on observational studies and available evidence.
When a patient has musculoskeletal pain, such as neck pain, physiotherapists are typically the first medical professionals they see. However, physiotherapists’ thorough assessments performed as part of the triage process may help to uncover any serious neurological pathology that may be hiding, such as cranio-cervical dissection or aneurysm. According to Firas Mourad’s cross-sectional study from Italy,10 just 5% of physiotherapists regularly check for warning signs. The examination of the cranial nerve can provide clues about neurological abnormalities; however, in this cohort study, 57.8% of the participants had not had any special training in this area, and 31% of the untrained participants did not think that the examination of the cranial nerve was a necessary ability for their clinical work. This underlines how critical it is for physiotherapists to have solid knowledge, regardless of their place of employment.
Conclusion
A case report has been presented to raise awareness about the potential risk of using neck traction devices which may lead to traumatic vertebral artery dissection. This injury can result in a stroke and therefore safety measures need to be taken into consideration to prevent such incidents. Recognizing this association can help prevent vertebral artery injury and ensure the safety of individuals using these devices.
Acknowledgement
We would like to thank Paper True Website for English language editing.
Footnotes
Disclosure. The authors declare no conflicting interests, support or funding from any drug company.
- Received September 2, 2023.
- Accepted May 9, 2024.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.