


Abstract
Objective: To study clinical and radiological factors that may correlate with independent walking (IW) following advanced cervical spondylotic myelopathy (CSM) surgery.
Methods: A retrospective case series including all advanced CSM patients (Nurick 4 and 5) who underwent surgery from 2003-2010 in the Division of Neurosurgery, Department of Surgery, College of Medicine, King Saud University and King Khalid University Hospital, Riyadh, Saudi Arabia. Only patients with 6 months or more follow-up were included. A neuroradiologist who was blinded to the clinical data reviewed all MRI studies.
Results: Forty-three patients were included (83% males, mean follow-up 29 months). A better preoperative neurological status was a positive predictor of IW after surgery (85.7% Nurick 4 versus 36.4% Nurick 5, p=0.001). Independent walking was less likely in patients with the following MRI features: longer T2-weighted image (T2WI) signal changes (p=0.001), well-circumscribed T2WI signal changes (p=0.028), T1WI hypointensity (p=0.001), and narrow spinal canal diameter (p=0.048). Multivariate regression revealed that both an increased T2WI signal change length and T1WI hypointensity were independent predictors. The risk of dependent walking increased by 1.35 times as the T2WI signal intensity length increased by one mm, and by 14-times with T1WI hypointensity.
Conclusions: Regaining IW after surgery in patients with advanced CSM was less likely for cases showing MRI features of longer T2WI signal changes and T1WI hypointensity. Better baseline walking, less defined T2WI signal change, and a wider spinal canal were good prognostic factors.
Cervical spondylotic myelopathy (CSM) may lead to significant disability.1-3 Progressive compression of the spinal cord causes chronic ischemia, local inflammatory response, and endothelial cell loss that may result in permanent spinal cord damage.4 In addition, there is an enhanced permeability in the blood-spinal cord barrier, leading to contact between the peripheral immune system and the spinal cord. Subsequently, there is an increased inflammatory reaction, resulting in more adverse effects on the spinal cord.5 Eventually, the spinal cord develops cystic cavitation, gliosis, degeneration of the central grey and medial white matter, Wallerian degeneration of the posterior columns and posterolateral tracts, and a loss of anterior horn cells. These changes are reflected on the clinical presentation and MRI features of the patients. The ability to detect changes related to spinal cord compression plays an important role in predicting clinical and functional outcomes. Several clinical and radiological factors have been studied as potential predictors for functional outcome. Relevant clinical predictors include the patient’s age at diagnosis, the duration of symptoms prior to surgery, medical comorbidities, the preoperative neurological status, and the surgical procedure performed.6,7
The MRI predictors of unfavorable outcome include hypointensity on T1-weighted images (T1WI), the type of signal intensity on T2-weighted images (T2WI), and a reduction of the spinal canal diameter.6,8-12 The correlation between the length of signal change on T2WI MRI sequences and clinical outcome after surgery has not been established. Changes in the internal structure of the spinal cord could appear as alterations in the signal intensity on T1- and T2-weighted MRI sequences.8,13 Hyperintensity on T2WI corresponds to focal gliosis, myelomalacia, vascular ischemia, and edema. Therefore, it is possible that patients with longer MRI signals experience less favorable clinical recoveries after surgery, particularly if the changes correspond to hypointensity on T1WI. In the current study, our objective was to assess the correlation between clinical and MRI features and independent walking (IW) after surgery in an attempt to predict functional recovery. Only patients with advanced myelopathy were included to avoid any bias that may result from involvement of patients with different disease severity.
Methods
Study design
The present study is a retrospective case series conducted in the Division of Neurosurgery, Department of Surgery, College of Medicine, King Saud University and King Khalid University Hospital, Riyadh, Saudi Arabia. Approval was obtained from the King Saud University Research Ethics board prior to the start of the study. All consecutive cases with advanced CSM (Nurick 4 and 5) who underwent a decompressive surgical procedure with or without stabilization between January 2003 and January 2010 were included. Only patients with follow-up of 6 months or more were included. The exclusion criteria were cervical myelopathy secondary to a non-degenerative etiology (for example, demyelination, trauma, tumor, and infection) and patients with a lower limb pathology that interferes with the ability to walk (for example, advanced osteoarthritis of the hips and knees). A detailed review of the medical files of all included patients was performed. A single neuroradiologist who was blinded to the clinical data reviewed all of the MRI studies using pre-established criteria.
The Nurick scale was first introduced in 1972 for the assessment of walking ability in CSM patients. This scale consists of 6 grades corresponding to the patient’s disability (Table 1). Several studies have utilized the Nurick classification in CSM patients due to its validity and reliability.7,14,15 Based on Nurick grading, CSM patients were considered advanced if they were grades 4 or 5. However, patients who were able to walk independently were given Nurick grades of 0-3.
Nurick classification of disability in cervical spondylotic myelopathy.
Data variables and outcome.Clinical variables
Descriptive data, including age, gender, body mass index, duration of neurological symptoms, preoperative disability status (according to the Nurick grade), comorbidities, and the type of surgical procedure performed (namely, anterior versus posterior), were obtained. A phone follow-up was achieved for 38% of patients. For all cases, including patients with phone re-assessment, the mean follow-up period was 29 months (range of 6-96 months).
Radiological variables
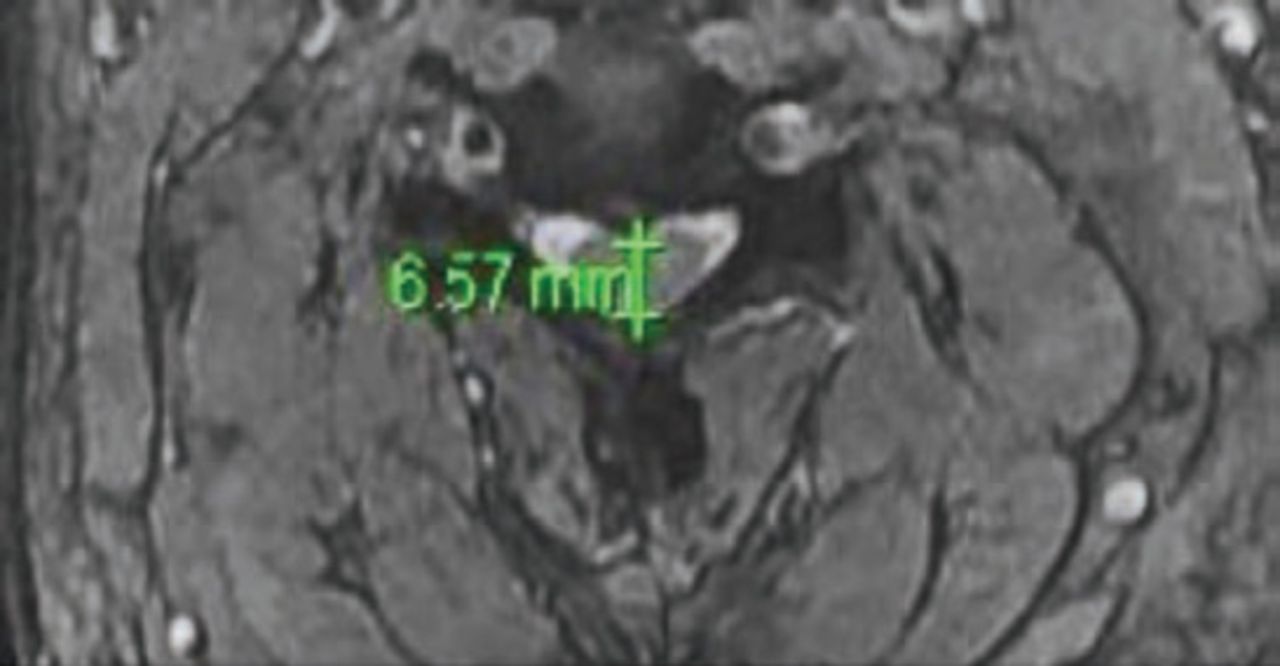
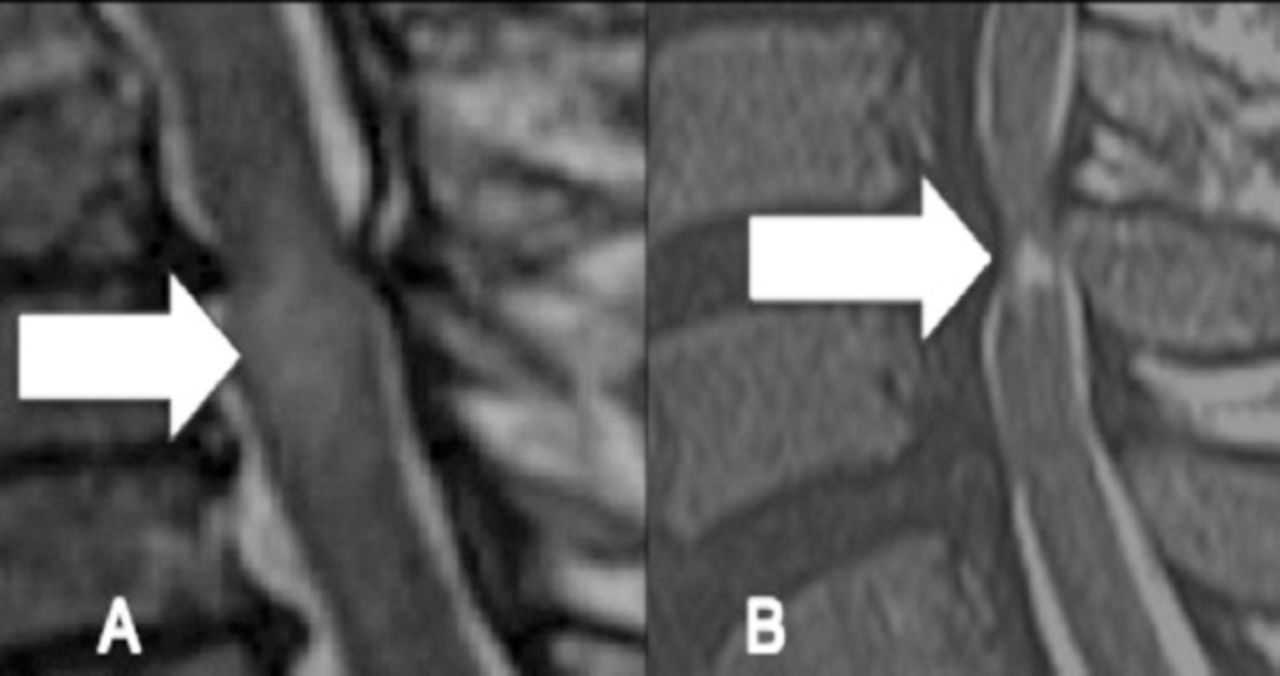
The MRI variables included the antero-posterior (AP) measurement of the cervical spinal canal at the area of maximum spinal cord compression (Figure 1), the presence of a signal change on the T1WI MRI sequence, and the length of the signal intensity change on T2WI. If there were non-contiguous regions of signal intensity change in a single cervical spine MRI study, their lengths were added and the total length was used for the analysis. Additionally, the type of signal change on the T2WI was classified into 3 types according to previous reports (Figure 2):9-11 Type 0: no signal change; Type 1: hyperintensity with fuzzy borders; and Type 2: hyperintensity with sharp borders. The present study used a 1.5 Tesla MRI scanner, which acquired 3.5 mm thick slices on spin echo T1WI (TR 430 msec, TE 12 msec) and turbo spin echo T2WI (TR 3600 msec, TE 110 msec).
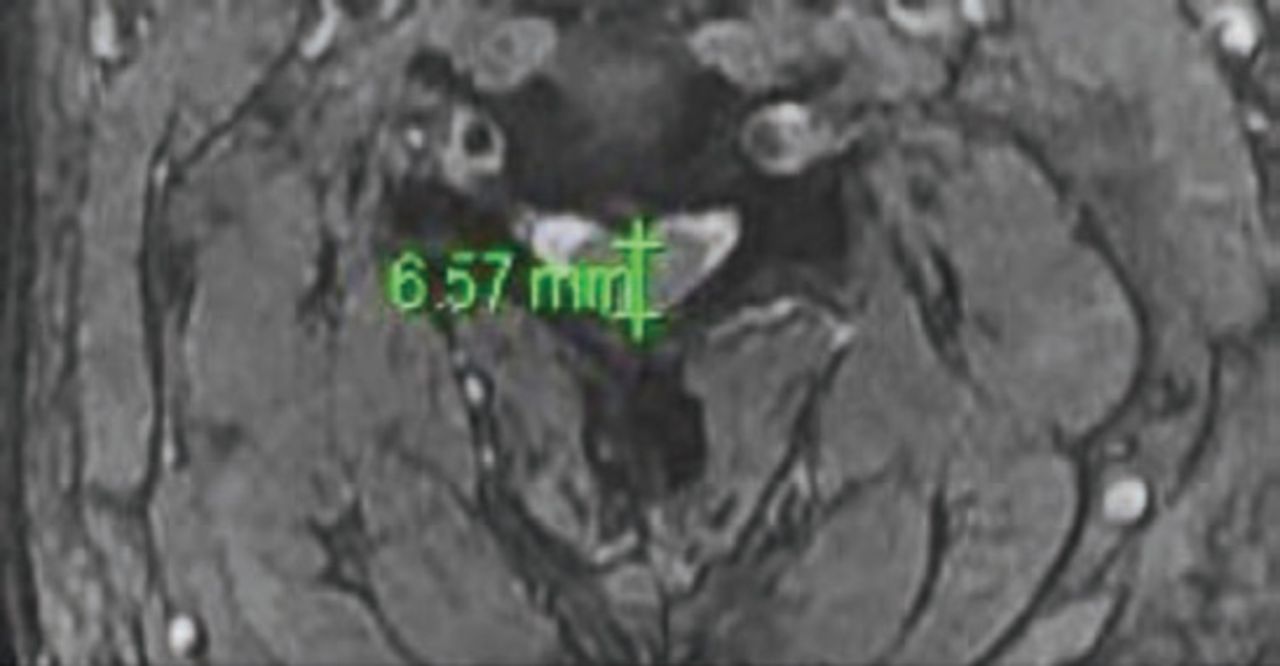
Measurements for the anterior posterior diameter of the cervical spinal canal.
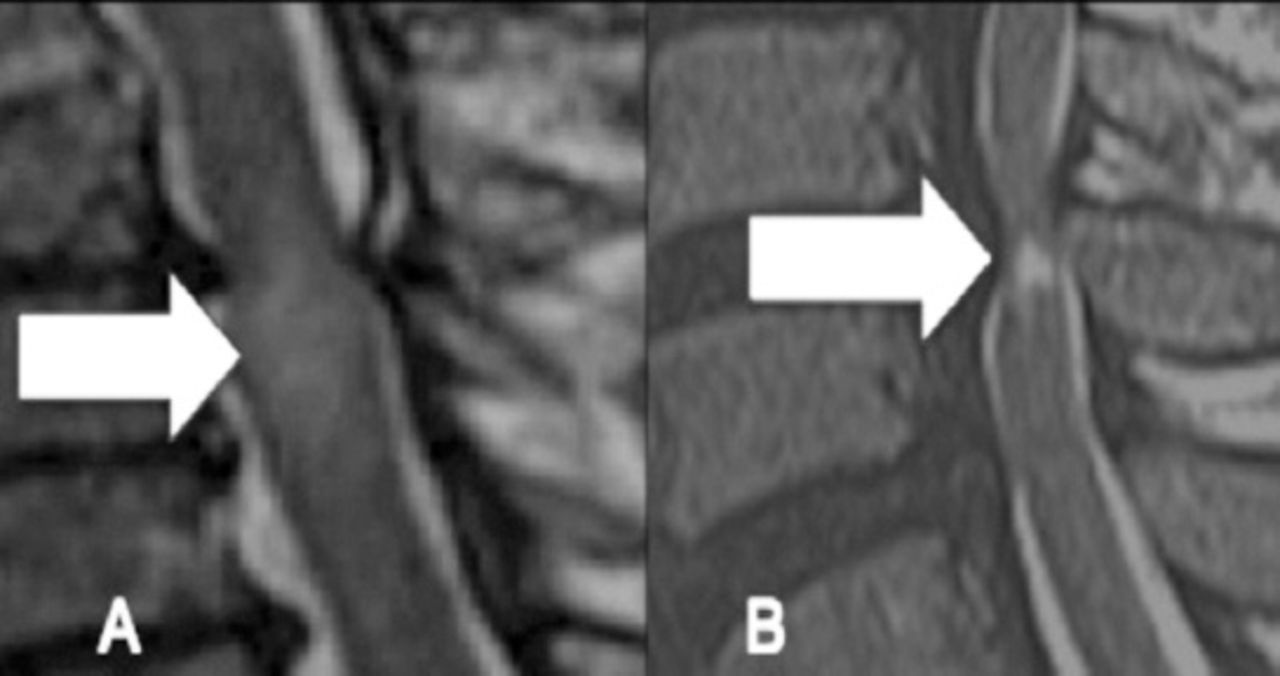
Preoperative T2WI sagittal MRI showing increased signal intensity (ISI). A) Type 1: faint ISI with fuzzy border (arrow). B) Type 2: intense ISI with well-defined border (arrow).
The main outcome was IW at the latest follow-up. The IW was assessed as a score of 0-3 using the Nurick grading system.
Statistical analysis
Statistical analysis was performed using the Statistical Package for Social Science, version 17.0 (SPSS Inc., Chicago, IL, USA). Descriptive statistics (mean, standard deviation, proportion, median, and inter-quartile range [IQR]) were used to describe the quantitative and categorical variables. Student t-test was utilized for continuous variables. Chi-square test was used for categorical variables. For the nonparametric data, the Mann-Whitney U-test was used for analyzing differences between 2 independent variables that were related to the binary outcome variable (postoperative ability to walk independently). Adjusted odds ratios with 95% confidence intervals were calculated. A p-value of <0.05 was considered to be statistically significant. A forward multivariate logistic regression was used to identify predictors of IW.
Results
Demographic and clinical information
Forty-three patients underwent surgery during the study period: 21 with Nurick grade 4 (48.8%) and 22 with Nurick grade 5 (51.2%). The demographic and clinical data for these patients are presented in Table 2. The average age for the study group was 61.8 years (59.3 years for Nurick 4, and 64.3 years for Nurick 5 groups). There were more males in the study group (p=0.054). A shorter duration of symptoms in patients with Nurick grade 5 compared with Nurick grade 4 (4.23 months versus. 6.7 months) was observed. This observation may have been due to a rapid deterioration in their condition, or it could also have been a result of recall bias, leading to inaccuracy in determining the onset of the symptoms. It is also possible that patients with Nurick grade 5 may have not included the period of walking with aid when considering their answers regarding their period of functional disability.
Characteristics of advanced cervical spondylotic myelopathy patients (N=43).
Clinical status following surgery
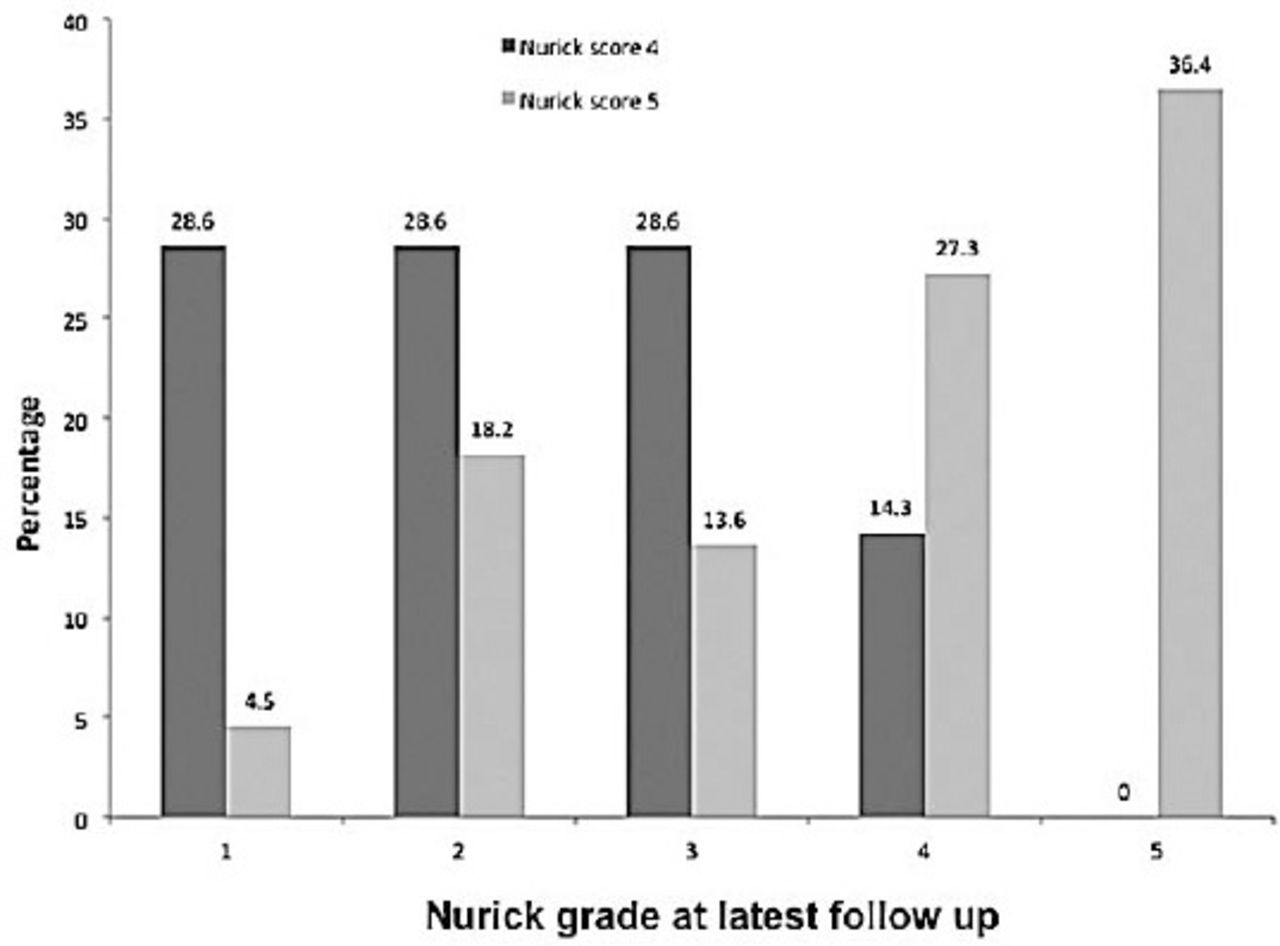
Eighteen patients (85.7%) with Nurick grade 4 walked independently after surgery; however, only 8 patients (36.4%) with Nurick grade 5 regained IW postoperatively (p=0.001, Table 2). Figure 3 illustrates the Nurick grade status for all patients at the final follow-up after surgery. There was no mortality in this case series.
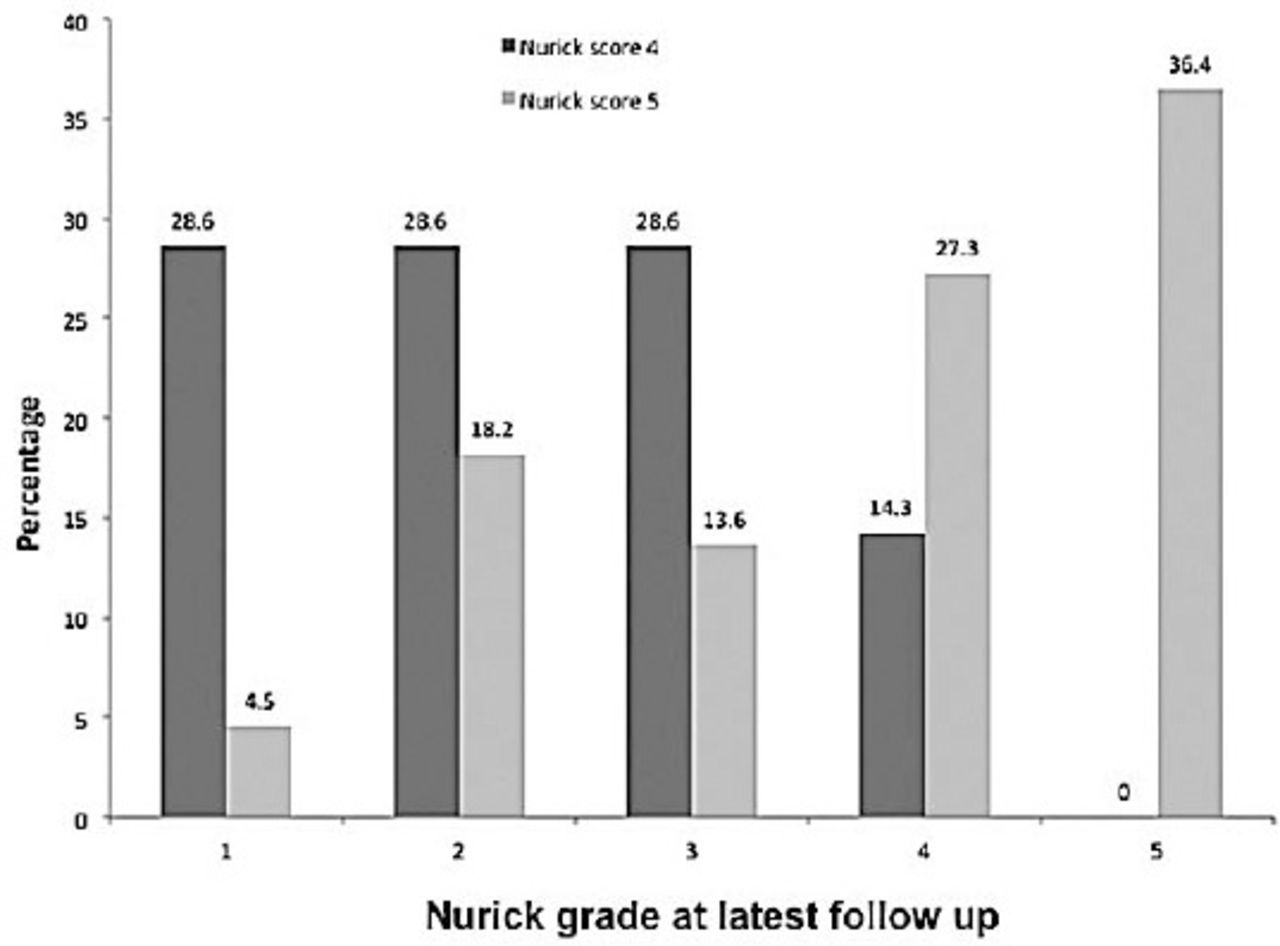
Nurick grade for all advanced cervical spondylotic myelopathy patients at latest follow-up. Among patients with pre-operative Nurick grade 5, 36.4% remained the same, 27.3% improved to Nurick 4 grade, and the rest (36.3%) had a Nurick grade from 1 to 3. On the other hand, among those with pre-operative Nurick grade of 4, only 14.3% remained the same while 85.7% improved to Nurick grade 1-3.
Imaging variables on preoperative MRI. Character and type of signal change
Hypointensity on preoperative T1WI was present in 17 patients (39.5%). Only five of the 17 patients were able to walk independently after surgery (p=0.001). The analysis of preoperative spinal cord T2WI MRI images showed high signal intensity in 40 patients (93.%) and was classified into 3 types. Type-0 was present in 2 patients (4.7%), all of whom could walk independently after surgery (p=0.36). Type-1 was present in 29 patients (67.4%), of which 20 patients could walk independently after surgery, compared with 9 patients who could not (p=0.1). Type-2 was present in 12 patients (27.9%), of which 8 did not achieve IW after surgery compared with 4 patients who could (p=0.028). All patients with low signal intensity finding on T1WI had concomitant high signal on T2WI.
Length of signal change
The signal change on preoperative T2WI MRIs was significantly longer in patients who could not walk independently postoperatively compared with those who could (21.6±13.22 mm versus 8±4.1 mm, p=0.001). While the same holds true for Nurick grade 5 patients (23.6±13.7 mm versus 8.13±2.29 mm, p=0.001), it was not significant for patients with Nurick grade 4 (12±3.46 mm versus 7.9±4.8 mm, p=0.18).
Reduction of the spinal canal antero-posterior diameter
The spinal canal AP diameter was significantly less on the preoperative MRIs of all patients who could not walk independently postoperatively compared with those who could (6.38±1.6 mm versus 7.56±1.98 mm, p=0.048). This finding approached significance when patients with Nurick grade 4 where assessed independently (4.83±3.75 mm versus 7.64±1.99 mm, p=0.06). For patients with Nurick grade 5, the spinal canal AP diameter was also smaller for those who could not walk independently postoperatively; however, it did not reach statistical significance (6.7±0.6 mm versus 7.37±2.1 mm, p=0.4).
Multivariate regression analysis for prediction of independent walking
A forward stepwise multivariate logistic regression analysis was used to identify the predictors of IW after surgery. Inclusion into the model was dependent on the result of the binary outcome of individual variables. The factors included were the preoperative Nurick grade and the MRI features of hypointensity on T1WI, the length of the T2WI signal intensity, the type of change on T2WI, and the AP diameter of the spinal canal. Significant predictors were the presence of T1WI hypointensity (odds ratio [OR] 14.26, 95% confidence interval [CI] 1.78-113.9; p=0.012) and the length of the T2WI signal intensity change (OR 1.35, 95% CI 1.05-1.73; p=0.019). The risk for dependent walking in patients with hypointensity on T1WI increased 14-fold compared with patients without a T1WI signal intensity change. As the length of T2WI signal intensity increased by one mm, the risk of dependent walking increased by 1.35-times.
Discussion
Clinical predictors of outcome
Patients with better preoperative neurological status are more likely to improve following surgery for CSM (Table 3).11,16 Early surgical results by Nurick in 197217 revealed a poor outcome (no improvement or death in the hospital) for patients who had a laminectomy for advanced CSM. Scardino et al7 analyzed 9 CSM patients with Nurick grade 5. Six patients improved postoperatively at least one grade after surgery, and only 22.2% regained their ability to walk independently at a follow-up 53.4 months later. Similarly, Matsunaga et al15 evaluated 31 CSM patients with Nurick grade 5 and found improvement in 16.2% after surgery. Better results were reported by Macdonald et al18 with an improvement in the ability to walk independently in 50% of both grades 4 and 5 patients after surgical decompression. Rajshekhar and Kumar14 found an improvement of one or more Nurick grades in all of their grade 5 patients and in 68.5% of grade 4 patients following surgical decompression at a follow-up 36.3 months later. The current study showed similar findings. The CSM patients with Nurick grade 4 had a better ability to walk independently postoperatively compared with patients with Nurick grade 5 (85.7% versus 36.4%). Several clinical variables have been addressed in the literature as being potential predictors for neurological and functional outcome after surgery. Many reports, including the current one, did not identify age, gender, duration of symptoms prior to surgery, medical comorbidities, or surgical approach (anterior or posterior) as significant predictors.19,20 However, a younger age group and a shorter duration of symptoms were good prognostic indicators in other studies.21,22
Previous studies on the surgical results of patients with advanced cervical myelopathy.
Signal change on MRI and outcome
Understanding the role of MRI in predicting outcomes is evolving. The signal change in T2WI has been categorized into fuzzy (type 1) or sharp and intense (type 2; Figure 2).9,23 Type 1 was believed to indicate a milder form of spinal cord change that is likely reversible.9,23 In contrast, type 2 corresponds to cavitation within the spinal cord and is consequently irreversible.9,23 Several studies, including the current one, have identified type 2 changes as a predictor of a poorer clinical outcome postoperatively.9,23 Vedantam et al9 assessed both types of MRI changes in 197 patients with CSM or ossification of the posterior longitudinal ligament (OPLL). After controlling for age (≥40 versus <40 years of age), the duration of symptoms (≤1 versus >1 year) and the Nurick grade (grades 1 to 3 versus grades 4 and 5), it was found that type 2 changes were associated with a decreased likelihood of recovery in patients with CSM or OPLL after anterior surgical decompression.9 Additionally, the findings of Vedantam et al9 agreed with other studies that when type 2 changes are combined with low signal on T1WI, the outcome is less favorable.8,9
Prior studies have demonstrated that signal change on T2WI was associated with a poor baseline clinical and functional condition.24 The involvement of more than one segment of the spinal cord has also been reported to indicate a poor postoperative prognosis.3,25 However, no previous study has provided a quantitative assessment of the length of the signal change on T2WI and its correlation to the functional outcome. The current study demonstrated that independent walking postoperatively was less likely in patients with a longer signal change on T2WI when Nurick grades 4 and 5 were considered together (namely, as one severe group; p=0.001) and for the more severe group (Nurick 5; p=0.001).
The current study agreed with previous literature that hypointensity on T1WI indicates a poor prognosis. Ohshio et al26 reported histopathological correlation of various spinal cord pathologies with signal intensity on MRI. They described that the combination of T2WI hyperintensity and T1WI hypointensity indicated a severe cord involvement with necrosis and myelomalacia. Ramanausakas et al27 and Fox28 associated low signal intensity on T1WI with late stages of myelomalacia, cystic necrosis, and syrinx formation. Other reports have agreed that hypointensity on T1WI is a predictor for poor clinical outcome in patients with CSM.24,29
Reduction in the AP diameter of the spinal cord and outcome
The effect of direct compression on the spinal cord has long been considered to play a role in the pathogenesis of CSM.30-32 This is seen on MRIs as a reduction in the AP diameter of the spinal canal (Figure 1), which was confirmed in the autopsy studies of patients with CSM.22 However, the correlation of this measure with the severity of myelopathy and functional outcomes has been controversial.10,34 Bucciero et al35 found that the neurological outcome was poorer for patients with a lower ratio of AP diameter to transverse diameter in the spinal cord at the area of maximum compression. The current study found that a reduction in the spinal cord AP diameter is a poor predictor for independent walking postoperatively for all patients, regardless of the Nurick grade (p=0.012).
Study limitations
Our study should be interpreted within its retrospective design and limited sample size. There could be bias related to the patients’ recall of symptoms or their own assessment of IW. On MRI, it remains unknown if the entire signal change represents gliosis and neuronal loss or oedematous changes. The current study generates the hypothesis that patients with a longer signal change on preoperative MRIs have a poorer outcome. Studies that could correlate this finding to histopathological assessment are needed. Advancement in MRI technology could address neuronal loss more accurately in the spinal cord. While previous reports indicated that multi-segment T2WI involvement is a sensitive indicator of a poorer clinical outcome, adding multi-segment lengths may not be the same as a single lesion of a given length. However, the regression analysis has controlled for other factors that may account for poorer spinal cord involvement (hypointensity on T1WI, type 2 signal change on T2WI, and narrowness of the AP diameter of the spinal canal).
In conclusion, the current study demonstrated that patients with advanced CSM (Nurick 4 and 5) who had a better baseline walking ability, a shorter signal change on T2WI MRI, reduced signal change on T1WI MRI and a wider AP spinal canal diameter were more likely to regain the ability to walk independently after surgery.
Footnotes
Disclosure
The authors declare no conflicting interests, support or funding from any drug company.
- Received June 1, 2014.
- Accepted October 27, 2014.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.