


Clinical Presentation
A 62-year-old man, with no vascular risk factors or prior history of myocardial infarction, presented to the emergency department after experiencing a sudden collapse while driving. Neurological consultation was sought for a Glasgow coma scale of 9/15 and transient acute right hemiparesis 6 hours after the onset of his initial symptom. He scored 13 points on National Institute of Health stroke scale (maximum possible score of 42). His brachial systolic blood pressure was unequal: 90 mm Hg in the right arm and 120 mm Hg in the left arm. Imaging scans of brain (Figure A & B) and blood vessels (Figure C) were obtained.
Questions
What findings are observed in Figure A & B?
What does the vascular imaging scan show (Figure C)?
What is the diagnosis?
Answers
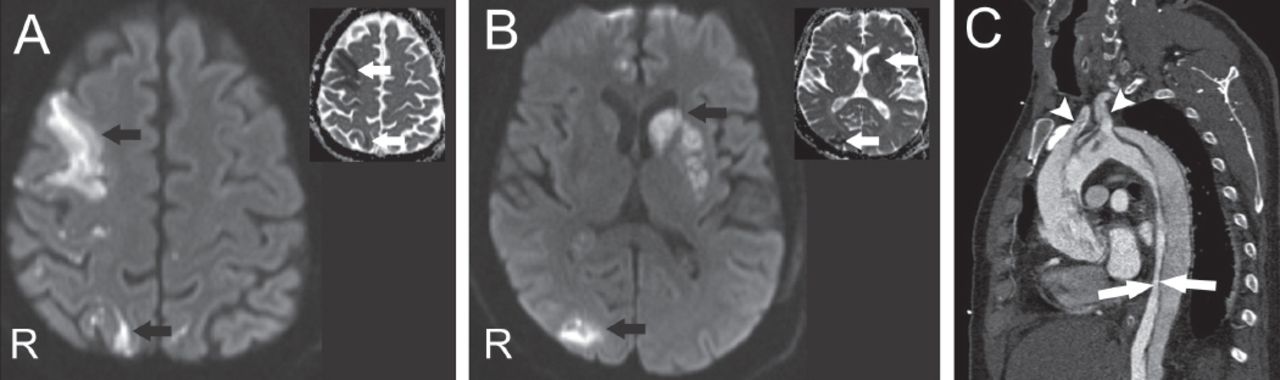
Cranial diffusion weighted MRI (Figures A & B) and corresponding apparent diffusion coefficient map (insets in answer Figures A & B) revealed multiple, acute infarctions (arrows) in the right frontal and parietal areas, and left basal ganglia.
Computed tomographic angiography showed the dissection of ascending, arch, and descending aorta (white arrows pointing to the true lumen) extending into the brachiocephalic trunk and left common carotid artery (arrowheads) (Figure C)
Type A aortic dissection, causing bilateral carotid dissection, accounted for bilateral, multifocal acute infarctions in both cerebral hemispheres.
Discussion
Aortic dissection that involves the ascending aorta is termed type A aortic dissection and is a rare cause of acute ischemic stroke.1 Bedside monitoring of pulses and blood pressure in both arms could aid in suspecting aortic dissection in stroke patients with altered mental status (especially in those who could not provide history of chest or abdominal pain). An inter-arm pressure difference of more than 20 mm Hg is abnormal and suggests an underlying vascular disease such as aortic dissection or subclavian stenosis.2 If aortic dissection is suspected or confirmed, thrombolytic therapy should be avoided in the case of hyperacute presentation (within 4.5 hours of ischemic stroke onset). This patient presented beyond the thrombolytic time window and the extension of the dissection into bilateral cervical carotid arteries accounted for multiple infarctions in the bilateral carotid distribution (Figure 1). He was considered unsuitable for surgical (repair such as segmental resection and interposition of Dacron graft) or endovascular intervention, as there was an extensive dissection involving the ascending, arch and descending aorta along with complications/poor prognostic factors such as preoperative bilateral ischemic stroke and renal dysfunction as a result of ischemic nephropathy. He was managed conservatively and died of a fatal cardiac arrest 7 days later. Beta-blockers are utilized for treating high blood pressure in aortic dissection with a target systolic blood pressure of 100-120 mm Hg and heart rate of 60-80/minute.3
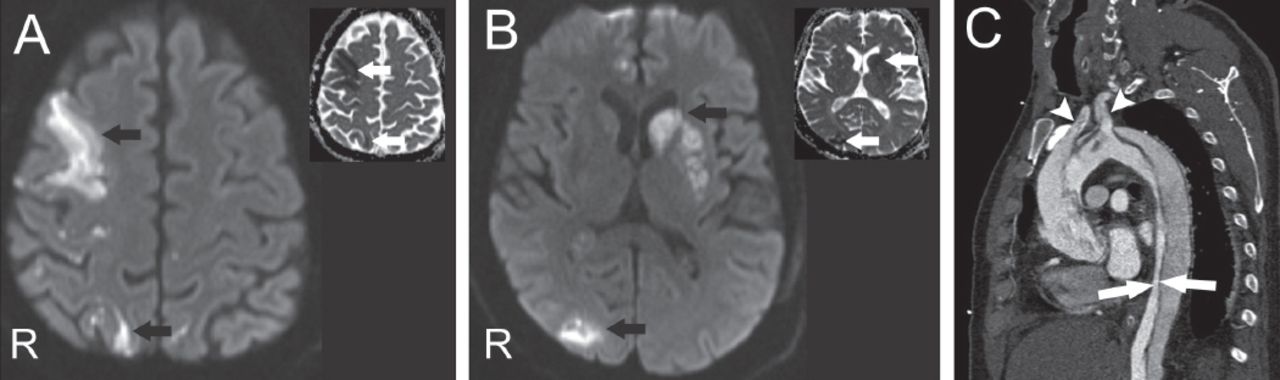
Axial diffusion weighted MRI (DWI, b=1000 sec/mm2) A & B) the brain and the corresponding apparent diffusion coefficient map (ADC map, insets in A & B) show restricted diffusion (black and white arrows), suggestive of acute infarction, in the right frontal and parietal convexities and left basal ganglia. C) Computerized tomographic angiography of the aorta showing dissection involving the whole length of aorta including the ascending segment (termed type A aortic dissection), with the arrows pointing to the true lumen in the descending aorta. Note the extension of dissection into brachiocephalic trunk (first white arrowhead) and left common carotid artery (second white arrowhead).
Footnotes
Notice: Authors are encouraged to submit quizzes for possible publication in the Journal. These may be in any specialty, and should approximately follow the format used here (maximum of 2 figures). Please address any submissions to: Editor, Saudi Medical Journal, Prince Sultan Military Medical City, PO Box 7897, Riyadh 11159, Kingdom of Saudi Arabia. Tel. +966 (11) 4777714 Ext. 42841. E-mail: info{at}smj.org.sa
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.