


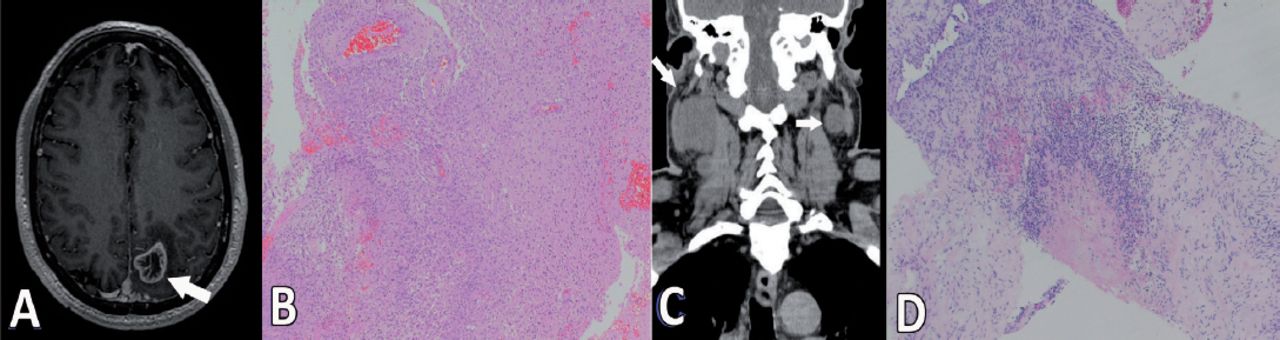
Glioblastomas are the most common malignant primary brain tumor. Only 0.2%-0.5% of cases metastasise outside the brain.1,2 We present a rare case of glioblastoma with bilateral cervical lymph node metastases. A 60-year-old man presented with 3-weeks of progressive right arm tingling. He had no medical history of note and the only abnormalities found on examination were decreased light touch and proprioception in his right arm. Brain MRI revealed a lesion in the left superior parietal lobe with surrounding oedema (Figure 1A). The appearances were suggestive of a high-grade glioma. He underwent debulking of the lesion and post-operative MRI scans showed complete removal of enhancing tumor tissue. He recovered very well after surgery with resolution of his symptoms. The tumor was histologically shown to be a glioblastoma (Figure 1B). He received 50 Gy whole brain radiotherapy, but declined concurrent chemotherapy. Approximately 6 months later, he noted painless swellings on either sides of his neck. Investigations showed enlargement of the upper cervical lymph nodes (Figure 1C). He refused a lymph node biopsy. Then 2 months later, he became increasingly confused. Repeat scans showed recurrence of the brain tumor and progressive enlargement of his cervical lymph nodes. He was convinced to undergo a lymph node biopsy. The biopsy specimens were consistent with that of a glioblastoma (Figure 1D). Soon after, he deteriorated rapidly and was too weak to receive chemotherapy. He received palliative care and died 2 months later.

Brain MRI A) Pre-operative enhanced T1-weighted MRI demonstrating a lesion in the left superior parietal lobe C) Non-contrasted computer tomography scan of the cervical region demonstrating a large right-sided mass in the upper cervical lymph node with a smaller left-sided lesion. B) Hematoxylin-eosin stained sections (X40) of the brain and D) Cervical lymph node with histological features of a glioblastoma.
Extracranial glioblastoma metastasis are extremely rare, with only 83 reported cases to date.2 The lack of a lymphactic system in the brain, the presence of the blood-brain barrier and dura, the low affinity of glioblastoma cells to arterial blood vessels, the lack of direct connection between the subarachnoid space and blood or lymphatic vessels, or because most patients with glioblastoma die before extracranial involvement becomes apparent may all account for the rarity of glioblastoma metastases.3 The most common sites for extracranial spread are the lungs and pleura followed by the lymph nodes, bones, and viscera1. Glioblastoma metastases to lymph nodes almost always follow surgical procedures, especially craniotomies.2 Surgery may predispose to metastases by allowing tumor cells access to scalp lymphatic and vascular pathways.4 However, there are reports of distant metastasis in the absence of surgery,4 in which case, intrinsic factors of the tumor may play a role. Locoregional nodal involvement almost always occurs ipsilateral to the craniotomy. Our case is unusual as there was bilateral nodal spread. This challenges the traditional belief that lymphatic drainage in the head and neck does not cross the midline. Indeed, lymphocintigraphic studies have shown that contralateral lymphatic drainage occurs is a small number of cases.5 We hypothesised that free tumor cells enter the scalp lymphatic system on the same side as the craniotomy then disseminate through the jugular chain of lymph nodes to either side. The proximity of the surgical field to the midline probably facilitates bilateral lymphatic metastases. The prognosis in patients with glioblastoma is poor, with an overall median survival of only 9-12 months.3 Survival in patients with glioblastoma metastases is worse with an average survival of only 1.5 months after the development of metastases.2 Survival time is influenced by age, performance status, histological grade, tumor location, and treatment modality.4 However, median survival even with surgery and chemoradiotherapy is only 4.2 months from the discovery of metastases.2
Extracranial metastases from glioblastoma are very rare and are associated with a poor prognosis, regardless of treatment. Lymphatic involvement usually occurs in the context of previous surgery and is almost invariably unilateral.
Acknowledgments
We would like to thank Dr. Ute Pohl, PhD, FRCPath, for providing the histopathological slides as well as reviewing the manuscript. We would like also to thank Dr. Mohammad M. Hayder, MBBS, MRCS for reviewing the manuscript.
- Received August 2, 2015.
- Accepted December 23, 2015.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue




{kind=link}
Related Articles
Cited By...
- No citing articles found.