


Article Figures & Data
Figures
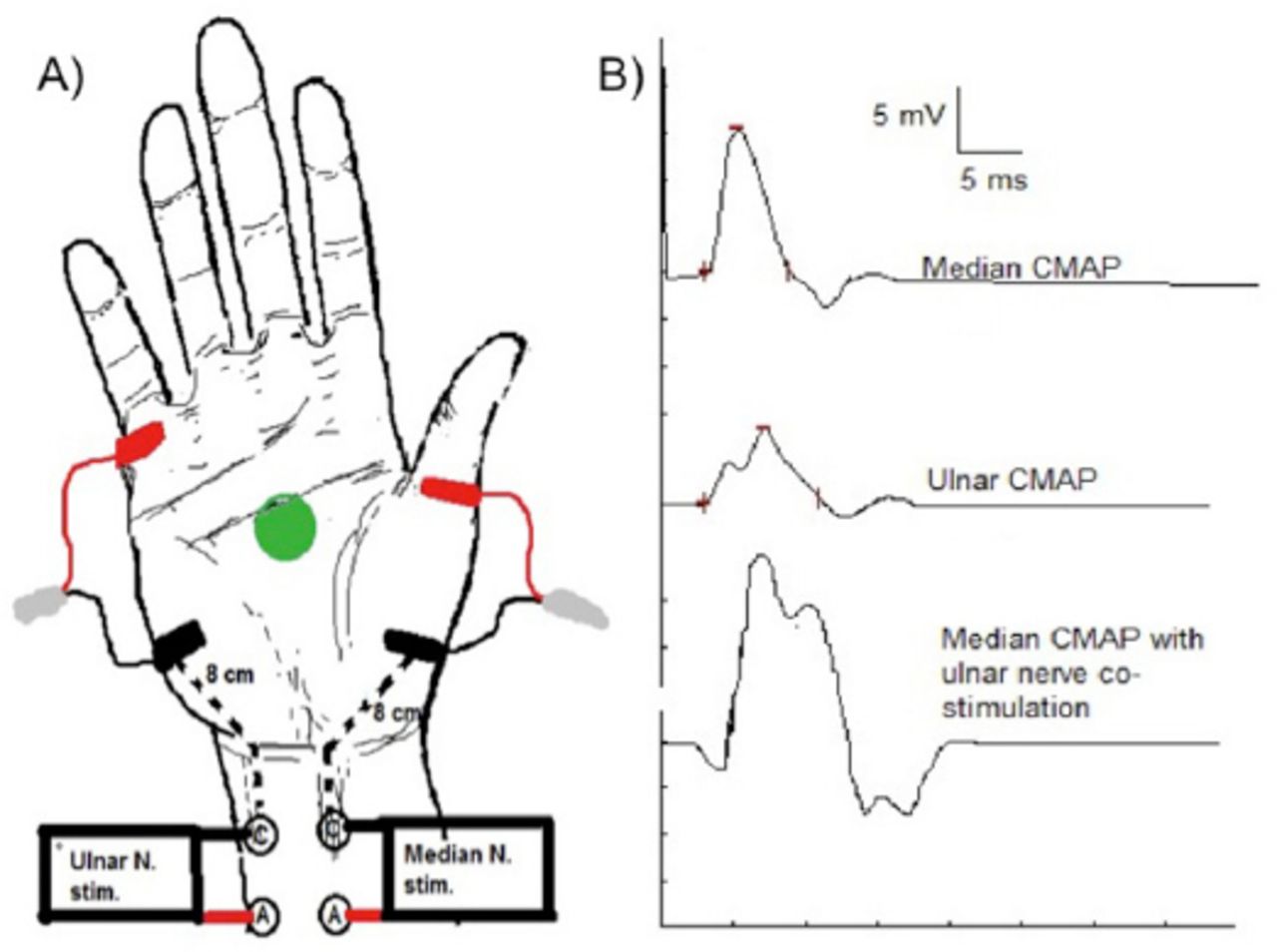
- Figure 1
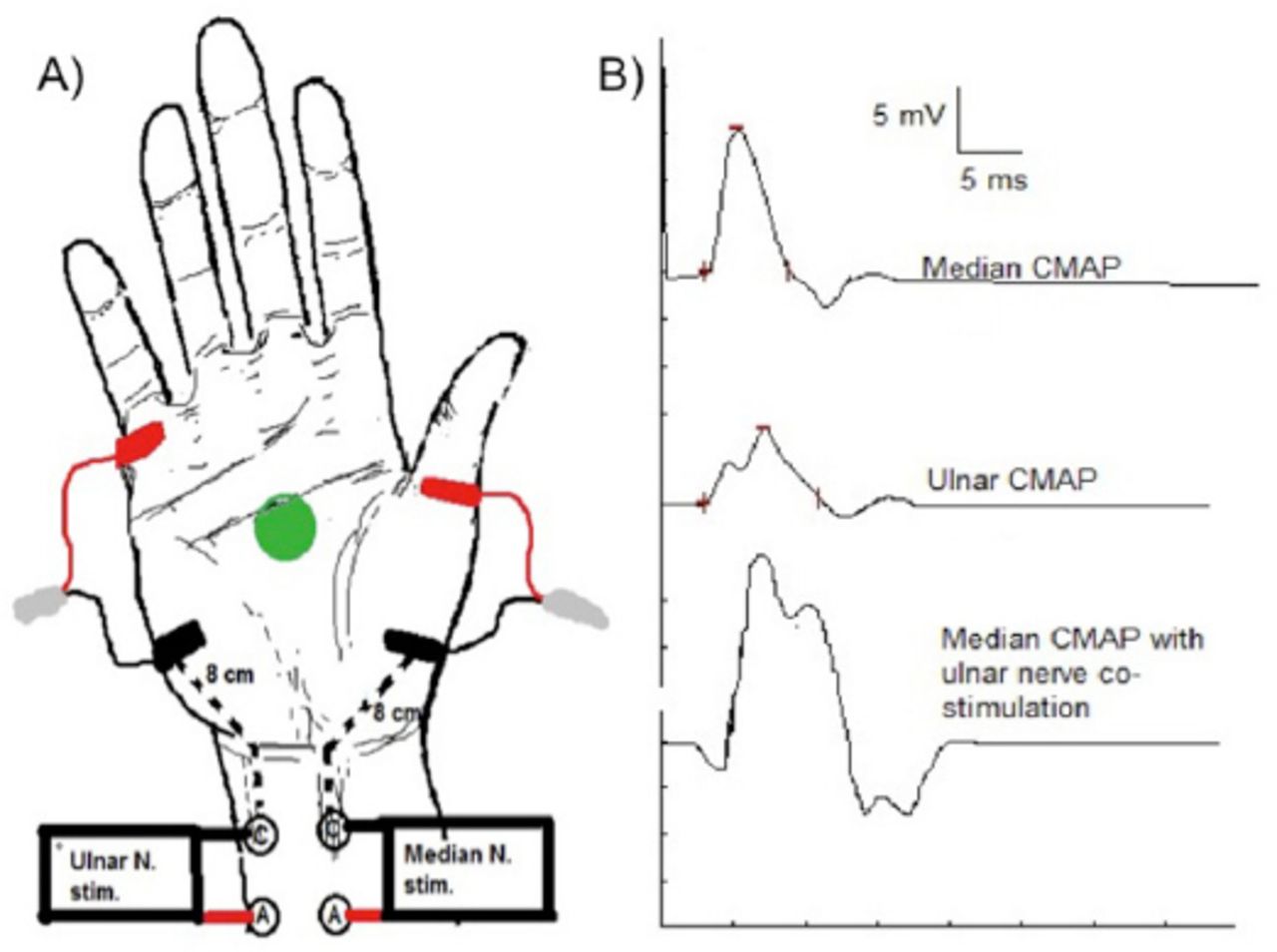
Median and ulnar motor nerve conduction studies recording abductor pollicis brevis and abductor digiti minimi, respectively. A) Electrode placement (black: active, red: reference, and green: ground) and stimulation sites. B) Compound muscle action potential waveform of the median (top trace) and ulnar (middle trace) nerves. Notice the change in the median waveform when ulnar co-stimulation occurs (bottom trance).
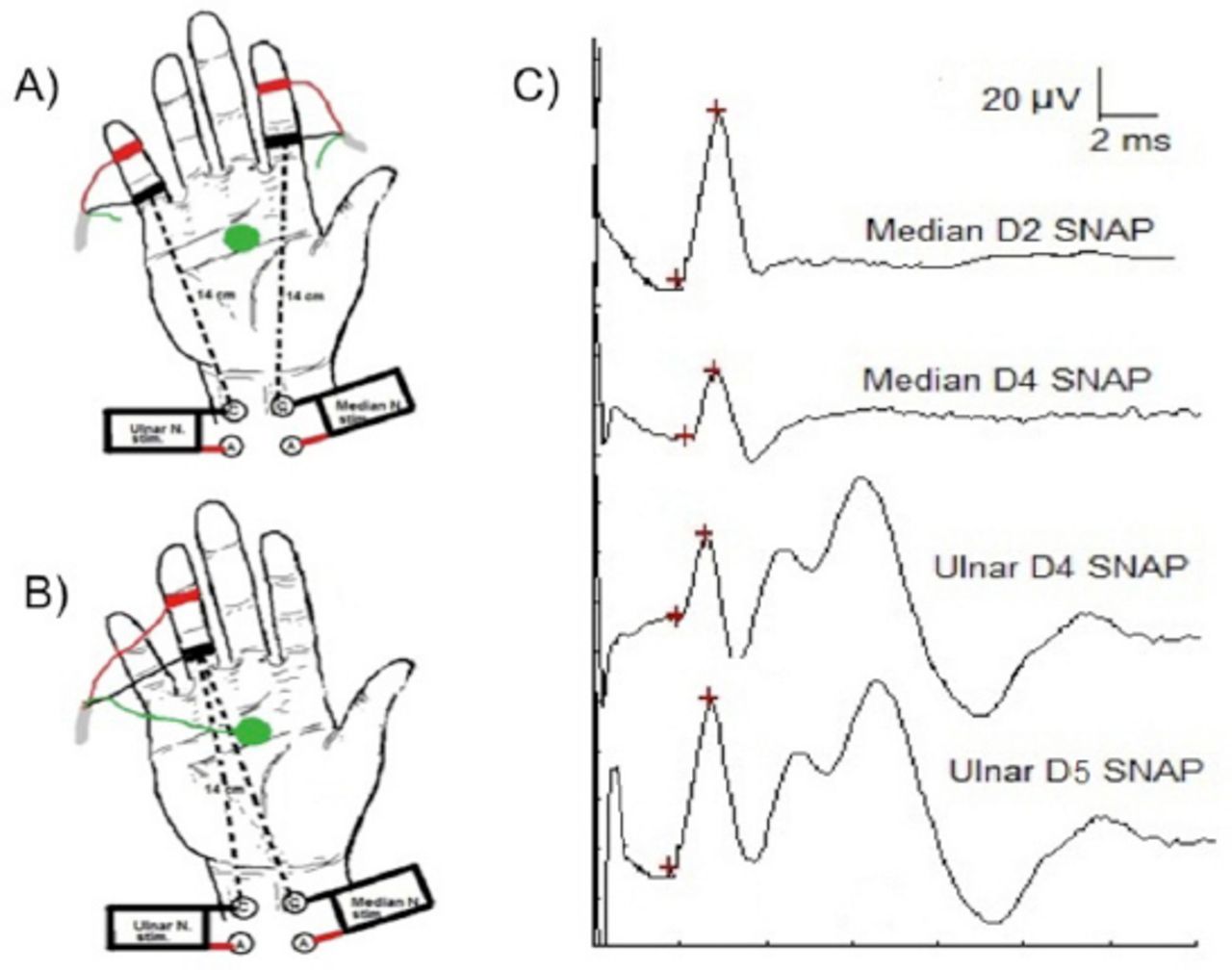
- Figure 2
Median-ulnar antidromic sensory comparison study. Electrodes placement (black: active, red: reference, and green: ground) and stimulation sites are shown. A) Median digit 2 versus ulnar digit 5. B) Median digit 4 vs ulnar digit 4 sensory comparison studies. C) Sensory nerve action potential waveform morphology.
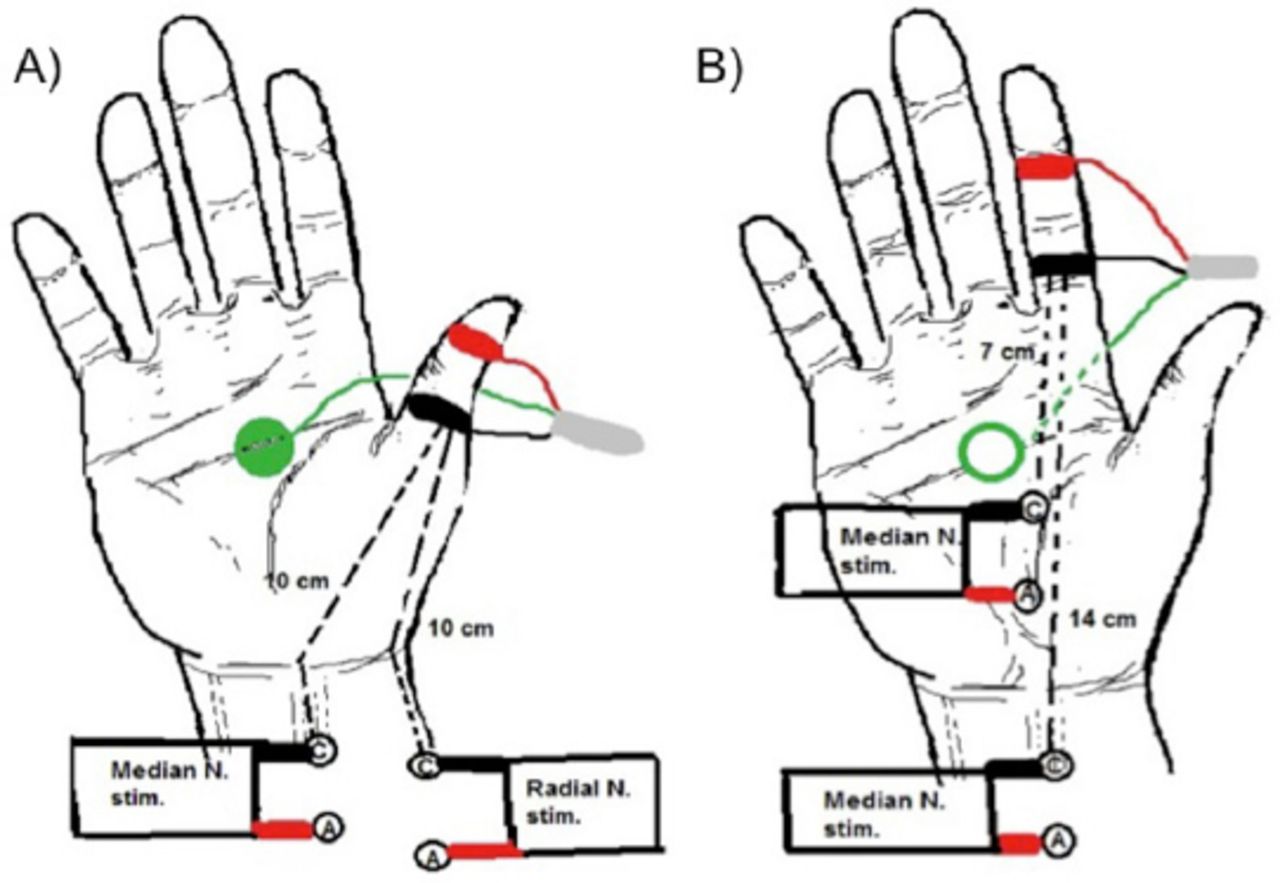
- Figure 3
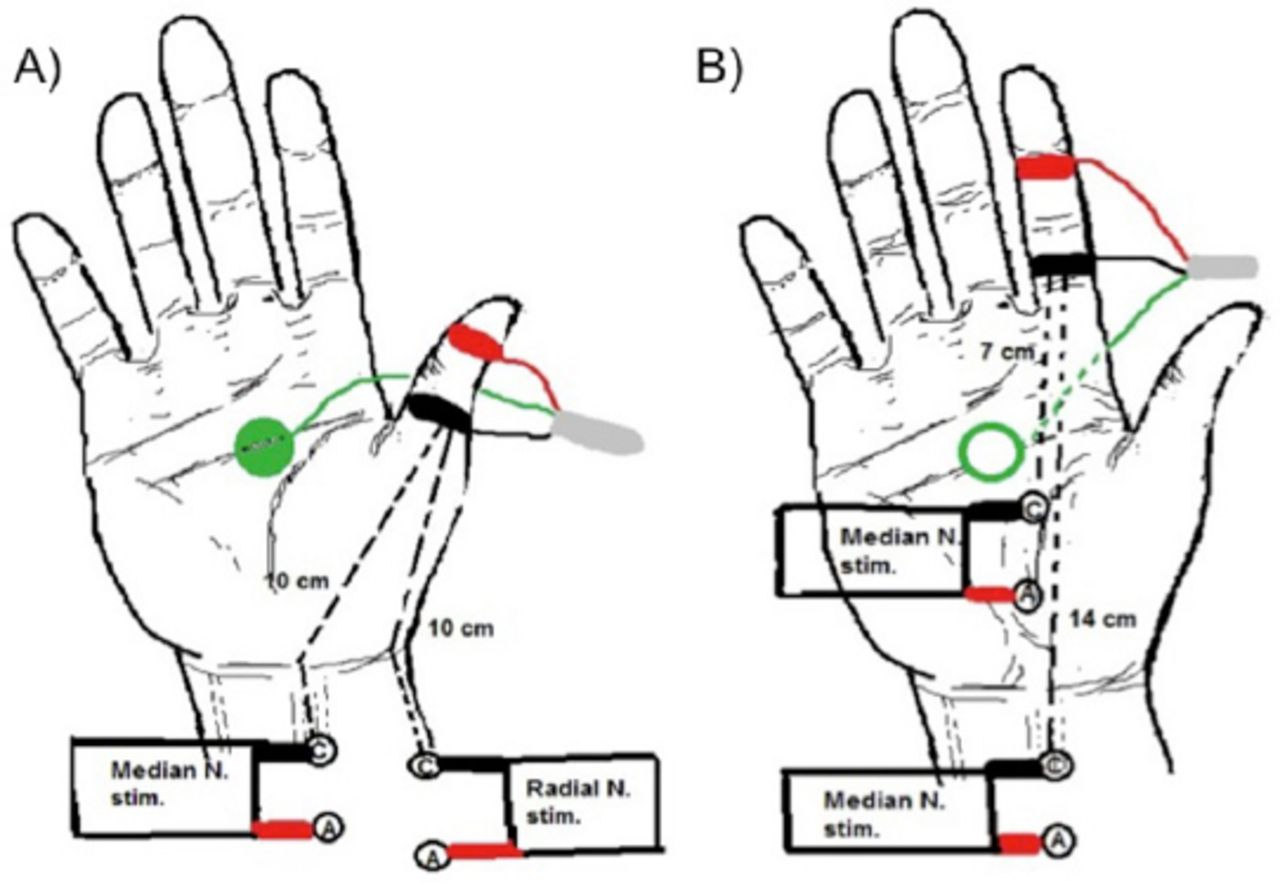
Comparison studies A) Median-radial antidromic sensory comparison study. B) Segmental median sensory conduction velocity of wrist-to-palm compared to palm-to-digit segments. Electrodes placement (black: active, red: reference, and green: ground) and stimulation sites are shown.
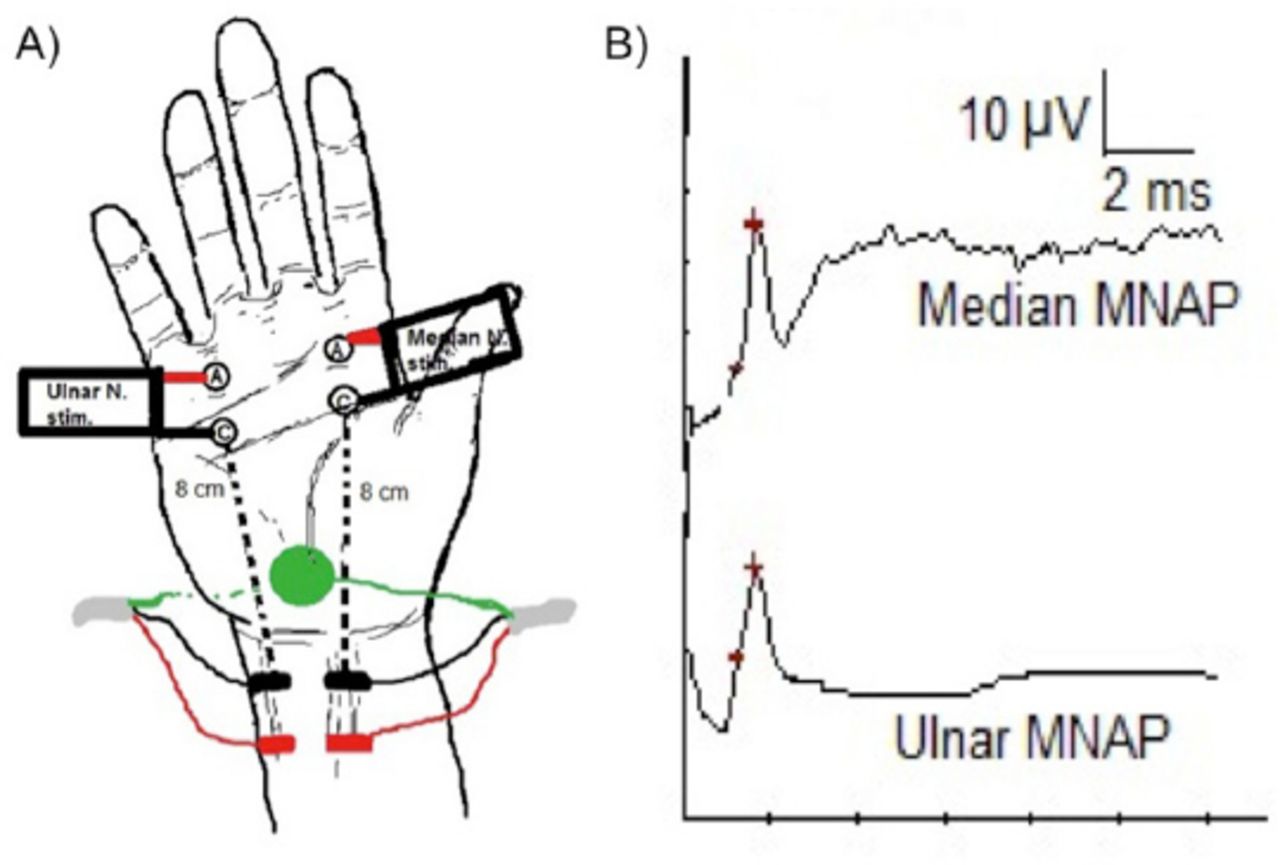
- Figure 4
Palmar orthodromic mixed nerve study. A) Electrodes placement (black: active, red: reference, and green: ground) and stimulation sites. B) The recorded median and ulnar mixed nerve action potential (MNAP) waveforms and peak latency comparison.
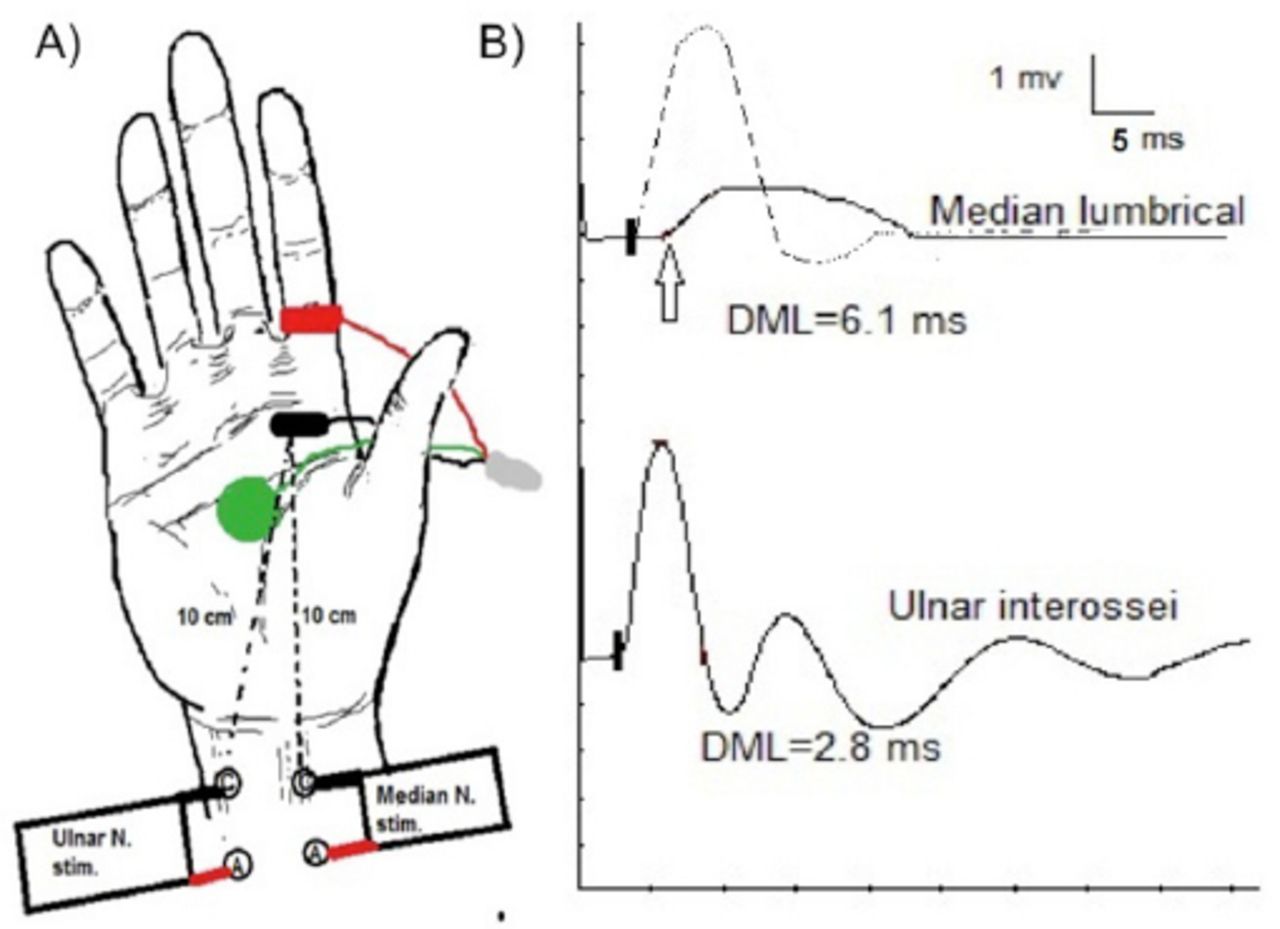
- Figure 5
Lumbrical-interossei comparison study. A) Electrodes placement (black: active, red: reference, and green: ground) and stimulation sites. B) In CTS, the median distal motor latency is prolonged (6.1 ms, arrow) in comparison to the ulnar latency (2.8 ms). The dashed-line in the top trace shows the change in median waveform morphology when ulnar co-stimulation occurs.
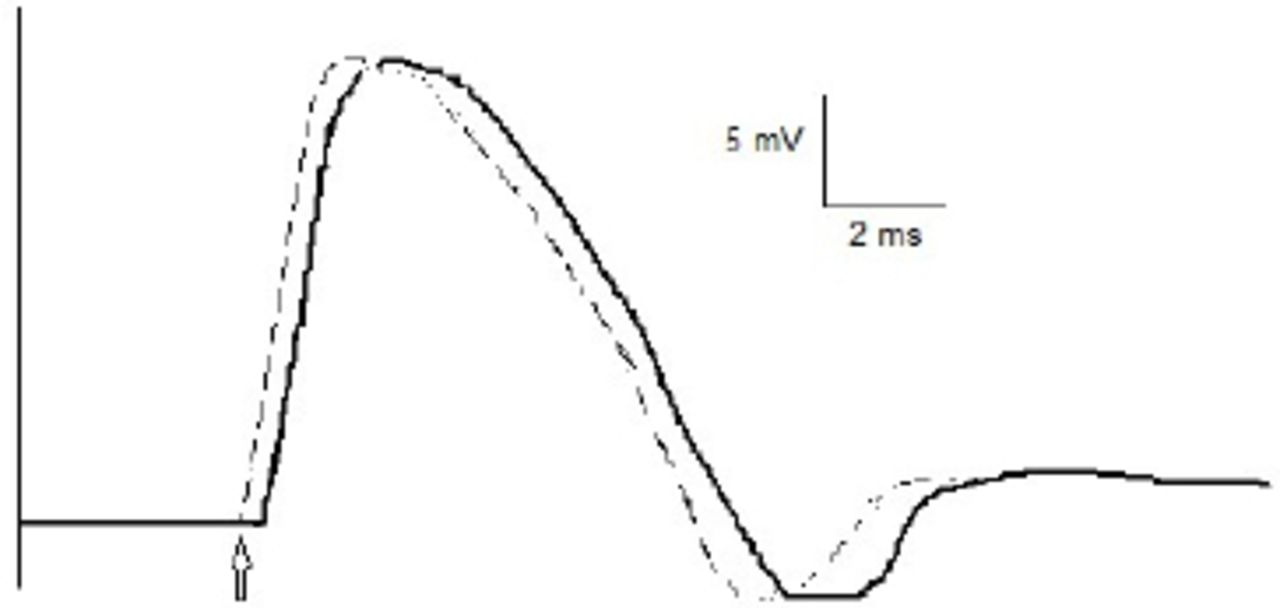
- Figure 6
Stimulus lead. Median compound muscle action potential (CMAP) waveform is shown. Note the shortening of distal motor latency without increment in the amplitude (dashed-line) indicating a stimulus lead.
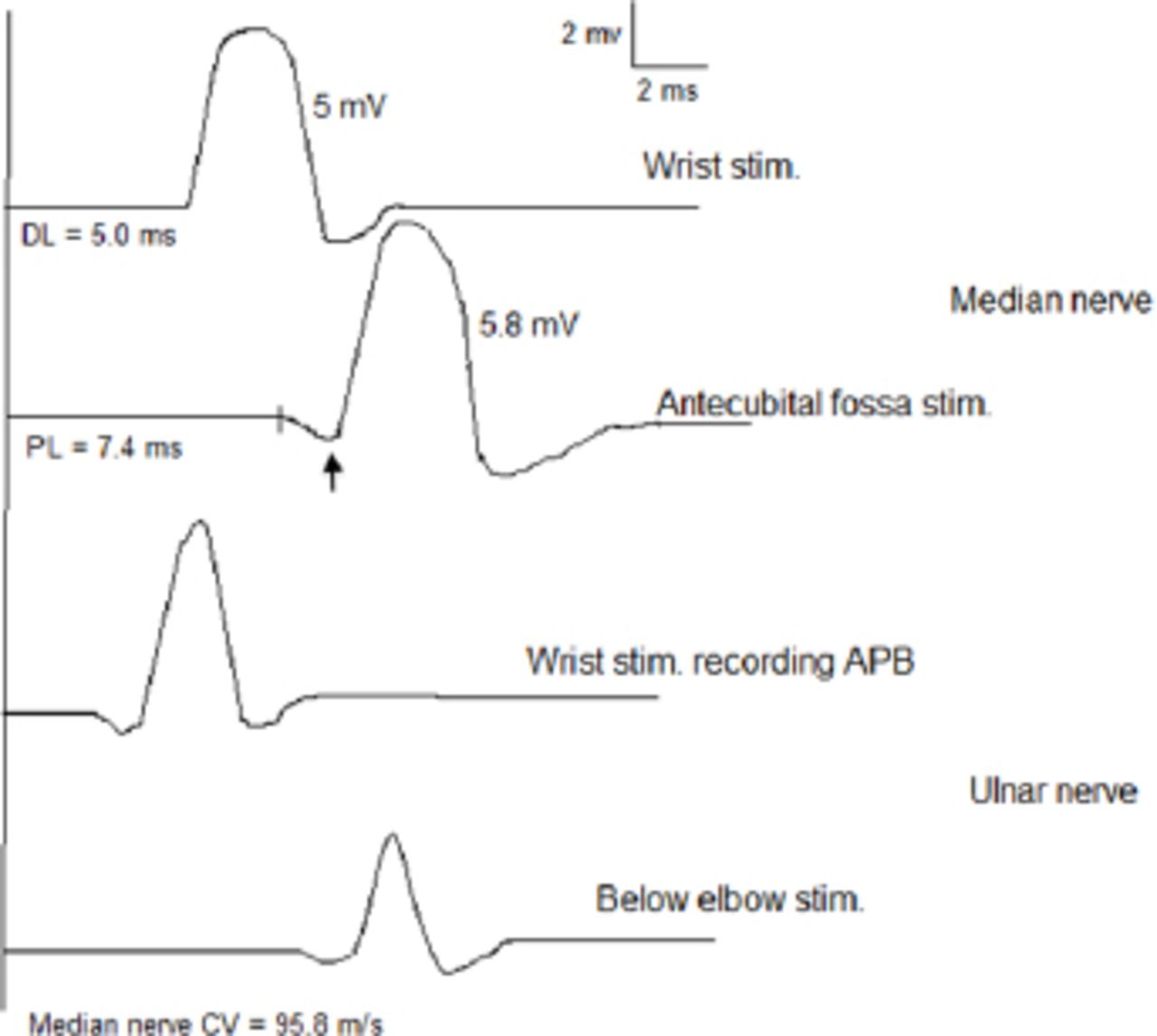
- Figure 7
Combination of Martin-Gruber Anastomosis (MGA) and Carpal Tunnel Syndrome (CTS). An MGA with cross-over fibers innervating the thenar muscles. Routine median motor study reveals higher compound muscle action potential (CMAP) amplitude with antecubital-fossa stimulation than that obtained with wrist stimulation. Ulnar nerve stimulation recording thenar muscles shows a drop in CMAP amplitude with proximal stimulation. With a coexistent CTS, there is a positive deflection (arrow) with antecubital- fossa stimulation, and a factitiously fast conduction velocity of the median nerve in the forearm.
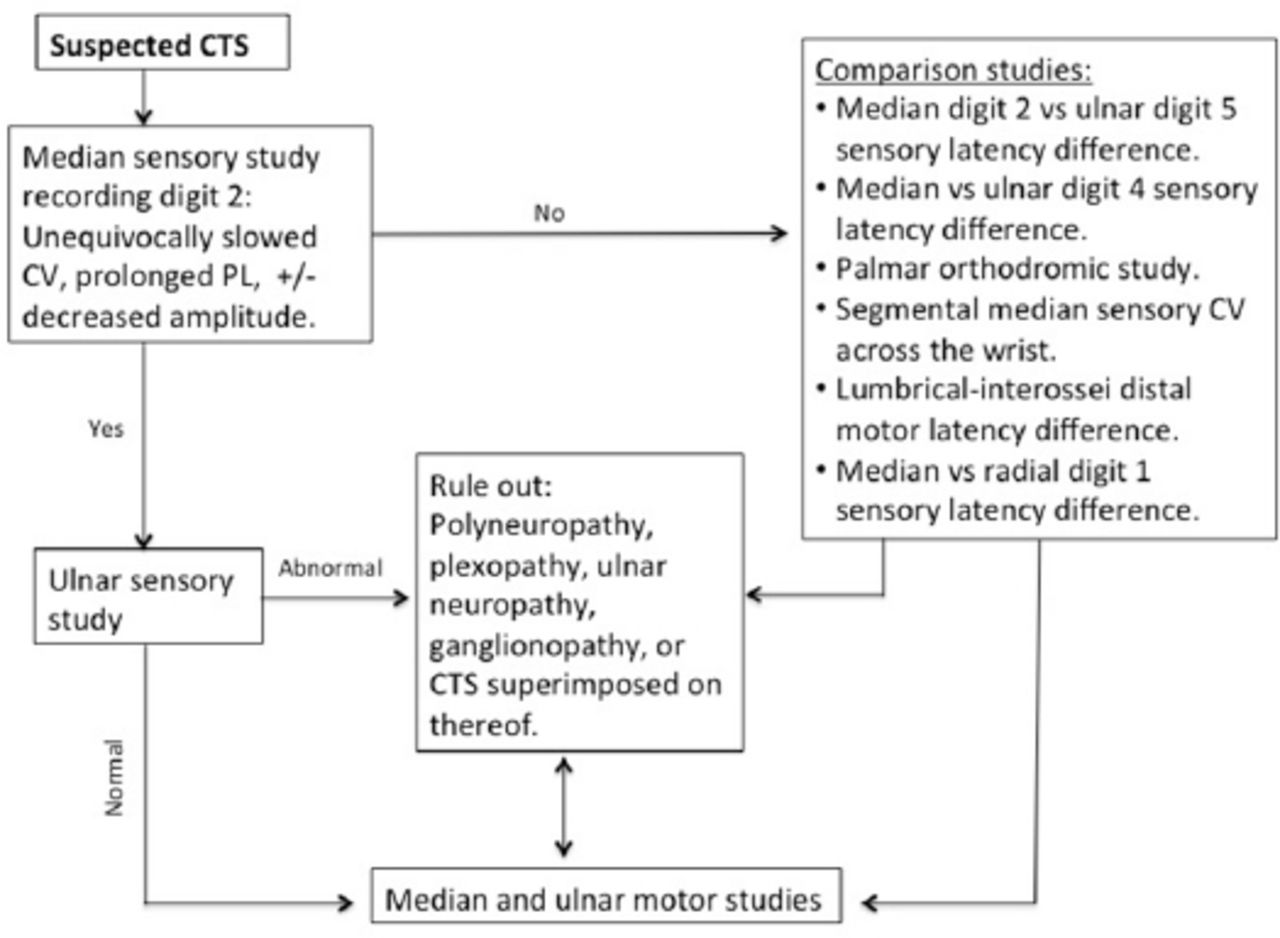
- Figure 8
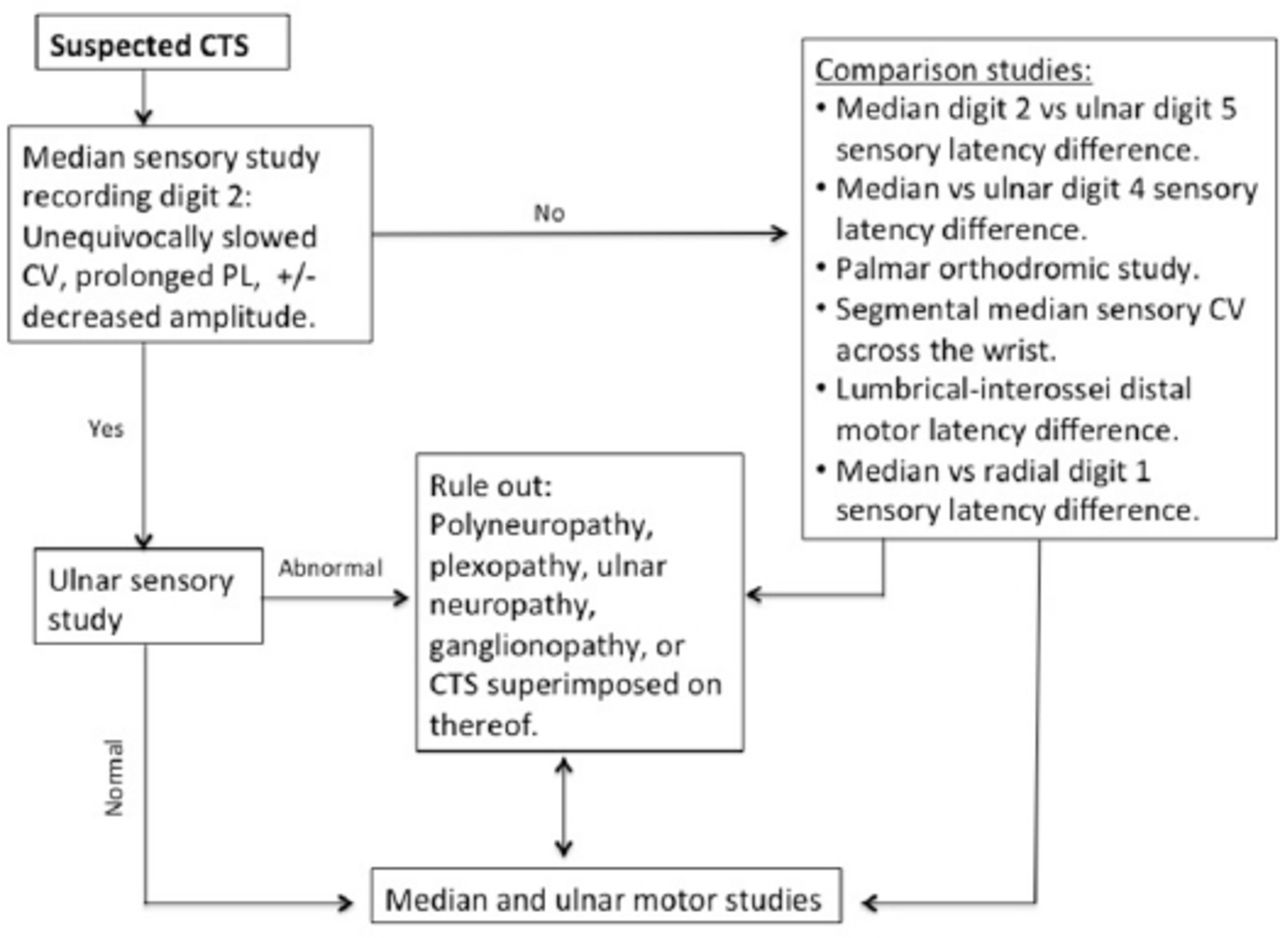
Nerve conduction study algorithm for patients with suspected CTS.
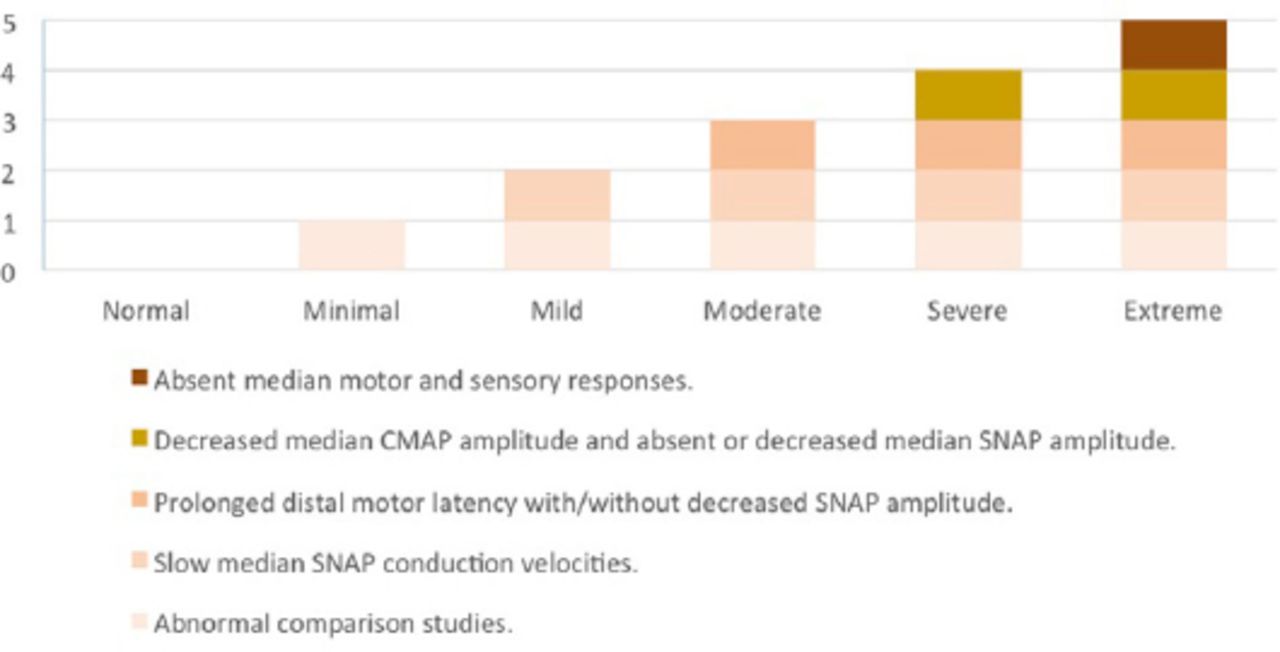
- Figure 9
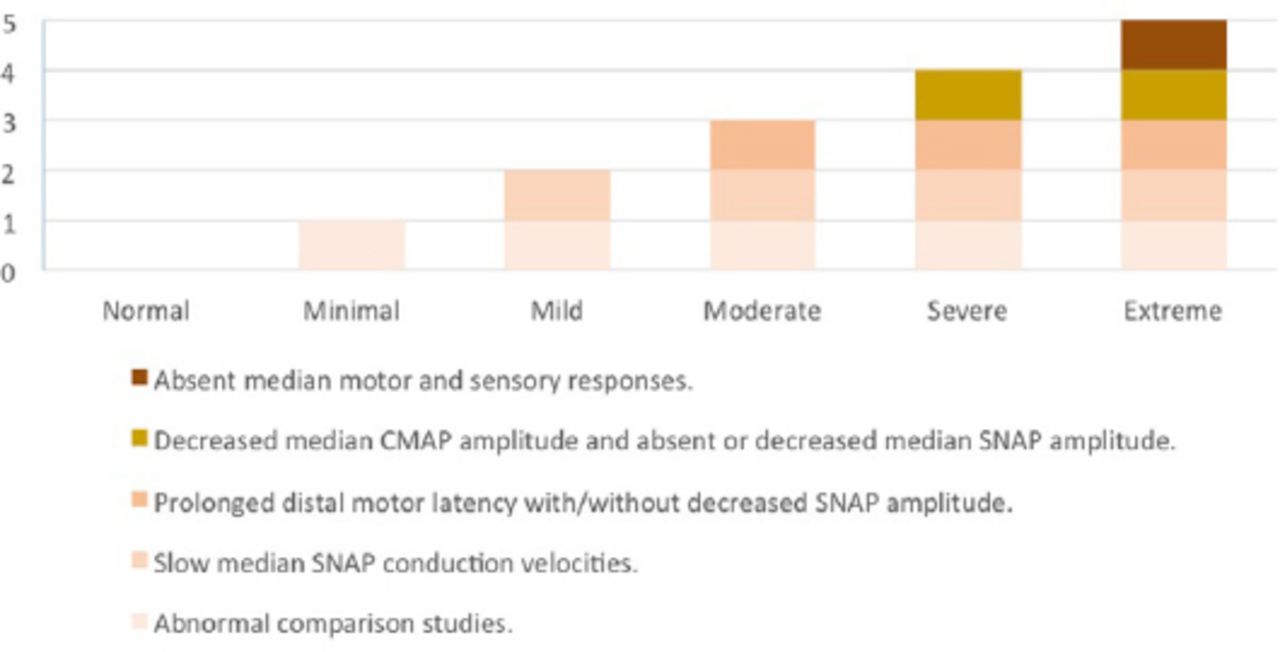
An NCS grading scale for the severity of CTS. The severity of involvement of NCS parameters generally follows the pattern depicted in the chart above. An unequivocal deviation from this pattern indicates a coexistent or a different diagnosis.





Tables
- Table 1
Sensory motor NCS and needle EMG findings in disorders that may mimic Carpal Tunnel Syndrome.
Disorders Sensory NCS Motor NCS Muscles involved by EMG Motor neuron disease e.g. ALS Normal38 Median CMAP: low amplitude
Ulnar CMAP: low amplitude38EMG signs of LMN dysfunction in at least 2 of the 4 CNS regions: bulbar, cervical, thoracic, or lumbosacral spinal segments38 C8/T1 radiculopathy Normal39 Median CMAP: normal or low amplitude
Ulnar CMAP: normal or low amplitude39All or some of C8/T1 supplied muscles (APB, FDI, ADM, FPL, EIP, and paraspinals)40 Thoracic outlet syndrome (lower trunk) Median SNAP: normal
Ulnar and medial antebrachial
SNAP: low amplitude41Median CMAP: low amplitude
Ulnar CMAP: less severe involvement than median CMAP42All or some of C8/T1 supplied muscles (T1 worse than C8), sparing paraspinals41 Medial cord lesion Median SNAP: normal
Ulnar and medial antebrachial
SNAPs: low amplitude41Median CMAP: low amplitude
Ulnar CMAP: low amplitude41C8/T1 muscles; spares fibers traveling through posterior cord (e.g., EIP) and Paraspinals41 C5 radiculopathy Normal39 Median CMAP: normal
Ulnar CMAP: normal39C5 muscles: supraspinatus, infraspinatus, deltoid, brachioradialis, biceps, and C5 paraspinals40 C6 radiculopathy Normal39 Median CMAP: normal
Ulnar CMAP: normal39C6 muscles: as in C5 + PT, FCR, triceps, anconeus, EDC and C6 paraspinals40 C7 radiculopathy Normal39 Median CMAP: normal
Ulnar CMAP: normal39C7 muscles: triceps, anconeus, PT, FCR, EDC, and C7 paraspinals40 Upper trunk Median-D1& 2 SNAP: low amplitude
Radial SNAP: low amplitude
Lateral antebrachial: low amplitude
Ulnar SNAP: normal41Median CMAP: normal Ulnar CMAP: normal41 All or some of C5/6 muscles (listed above) sparing paraspinals, serratus anterior and rhomboids41 Lateral cord Median-D1, 2 & 3 SNAP: low amplitude
Lateral antebrachial: low amplitude
Ulnar SNAP: normal41
Radial SNAP: normal41Median CMAP: normal
Ulnar CMAP: normal41Biceps, brachialis, PT, and FCR41 Median nerve at or proximal to the elbow Median SNAP: decreased
Ulnar SNAP normal43Median CMAP: low amplitude
Ulnar CMAP: normal43APB, FPL, FDP-D2 & 3, FDS, PQ, FCR and PT43 AIN neuropathy Normal Normal FPL, FDP-D2 & 3, PQ43 Length dependent axonal polyneuropathy Sural SNAPs are affected earlier and more severely than upper limb SNAPs44 Lower limb CMAPs are affected earlier and more severely than upper limb CMAPs44 Denervation is worse in distal compared to proximal muscles, and in lower more than upper limbs44 ADM - abductor digiti minimi, AIN - anterior interosseous nerve, ALS - amyotrophic lateral sclerosis, APB - abductor pollicis brevis, CMAP - compound muscle action potential, EDC - extensor digitorum communis, EIP - extensor indicis proprius, EMG - electromyography, FCR - flexor carpi radialis,
FDI - first dorsal interosseous, FDP D2 & 3 - flexor digitorum profundus digits 2 and 3, FDS - flexor digitorum superficialis, FPL - flexor pollicis longus, LMN - lower motor neuron, NCS - nerve conduction study, PQ - pronator quadratus, PT - pronator teres, SNAP - sensory nerve action potential
- Table 2
Reference values for the nerve conduction studies used in the evaluation of Carpal Tunnel Syndrome.
Study Onset-to-peak amplitude: LLN (3rd percentile) Peak latency: ULN (97th percentile) (ms) Onset latency: ULN (97th percentile) (ms) Conduction velocity: LLN (3rd percentile) (m/s) Digit 2 median antidromic sensory 11 mv* 4.0 3.3 NA Digit 5 ulnar antidromic sensory 10 mv* 4.0 3.1 NA Digit 2 median vs digit 5 ulnar peak latency difference NA <0.5 NA NA Digit 4 median vs digit 4 ulnar peak latency difference NA <0.5 NA NA Palmar orthodromic peak latency difference. NA <0.3 NA NA Median motor 4.1 mv* NA 4.5 49 Ulnar mot 7.9 mv* NA 3.7 52 (below elbow)
43 (across elbow)
50 (above elbow)LLN - lower limit normal, ULN - upper limit normal, NA - not applicable.
↵* Values represent all ages. For stratification by age and body mass index, we refer the reader to the paper of Chen et al11
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.