


Abstract
Objectives: To assess National Institutes of Health Stroke Scale (NIHSS), stroke volume, biochemical, and blood parameters for the prediction of one-month mortality in stroke patients
Methods: The study had retrospective design and 75 patients were involved that presented to a hospital Emergency Department between January 2016 and December 2017 in Adiyaman, Turkey diagnosed with acute ischemic cerebral infarction. The patients were divided into 2 groups according to whether mortality occurred within one month. Values for NIHSS, stroke volume, Glasgow Coma Scale, and blood parameters were compared between the groups.
Results: Values for Glasgow Coma Scale p=0.002, NIHSS p=0.001, stroke volume p=0.003, monocyte/HDL ratio p=0.047, neutrophils p=0.01, white blood cell p=0.007, calcium p=0.016, and albumin p=0.027 were statistically significant for the prediction of one-month mortality. There were no significant differences between the groups for other parameters.
Conclusion: The clinical, laboratory, and radiological findings individually provide significant support for the short-term prognosis of stroke. The evaluation of these results together can provide a clearer advance understanding of a prognosis to better manage the course of the disease and prevent death.
Stroke is the third most common cause of death for patients presenting to emergency departments worldwide.1 Thus, to foresee possible mortality and morbidity in stroke cases, adoption of the right treatment and follow-up approach is important.2 The quality of the health service in a hospital emergency department depends on the successful prediction of the course of the disease and the clinical picture that may arise. Being aware of the prognosis of the disease in advance is important not only for making optimal treatment decisions but also for correctly informing the patient and managing health expenditures.
In the literature, clinical parameters such as C reactive protein (CRP), red cell distribution width (RDW), neutrophil/lymphocyte ratio, and routine blood parameters such as albumin, infarct volume on admission, and National Institutes of Health Stroke Scale (NIHSS) score have previously been defined for the prediction of mortality in stroke cases.2-5 Pro-brain natriuretic peptides and pro-atrial natriuretic peptides, 2 other biochemical parameters that are not among the routine blood parameters, have also been shown to be important markers of stroke prognosis.6,7
This study aimed to evaluate the association of clinical, biochemical, and radiological parameters with one-month mortality in patients that presented to the emergency service and received a diagnosis of ischemic stroke.
Methods
Study design
This clinical study was based on a retrospective design. The study sample consisted of 75 patients that presented to the Emergency Department of a hospital in Adiyaman, Turkey between January 2016 and December 2017 and were diagnosed with acute ischemic cerebral infarction based on the findings of diffusion magnetic resonance (MR) imaging. Informed consent was obtained from each patient, local ethics committee approval was obtained, and the study was designed according to the principles of the Helsinki Declaration. Excluded from the study were patients for whom an NIHSS score or MR images were not available or were not obtained within the first 24 h after hospital admission, for whom it was not possible to measure infarct volume due to MR artifacts, or who had a history of stroke or transient ischemic attack, coronary artery disease, myocardial infarction, atrial fibrillation, or flutter.
Clinical evaluation
The clinical examination records of all study patients were evaluated and their NIHSS scores were determined based on the 12 parameters required for the calculation of this score.8 In addition, a Glasgow Coma Scale (GCS) score and the blood parameters HbA1c, D-dimer, CRP, erythrocyte sedimentation rate (ESR), lactate, triglyceride, LDL, HDL, B12, folic acid, white blood cell count (WBC), monocyte count, lymphocyte count, neutrophil count, monocyte/HDL ratio, calcium, ionized calcium, corrected calcium, and albumin were retrospectively evaluated. In addition to these blood parameters, body mass index, blood pressure at emergency admission, and known history of chronic diseases were also retrospectively recorded.
Radiological evaluation
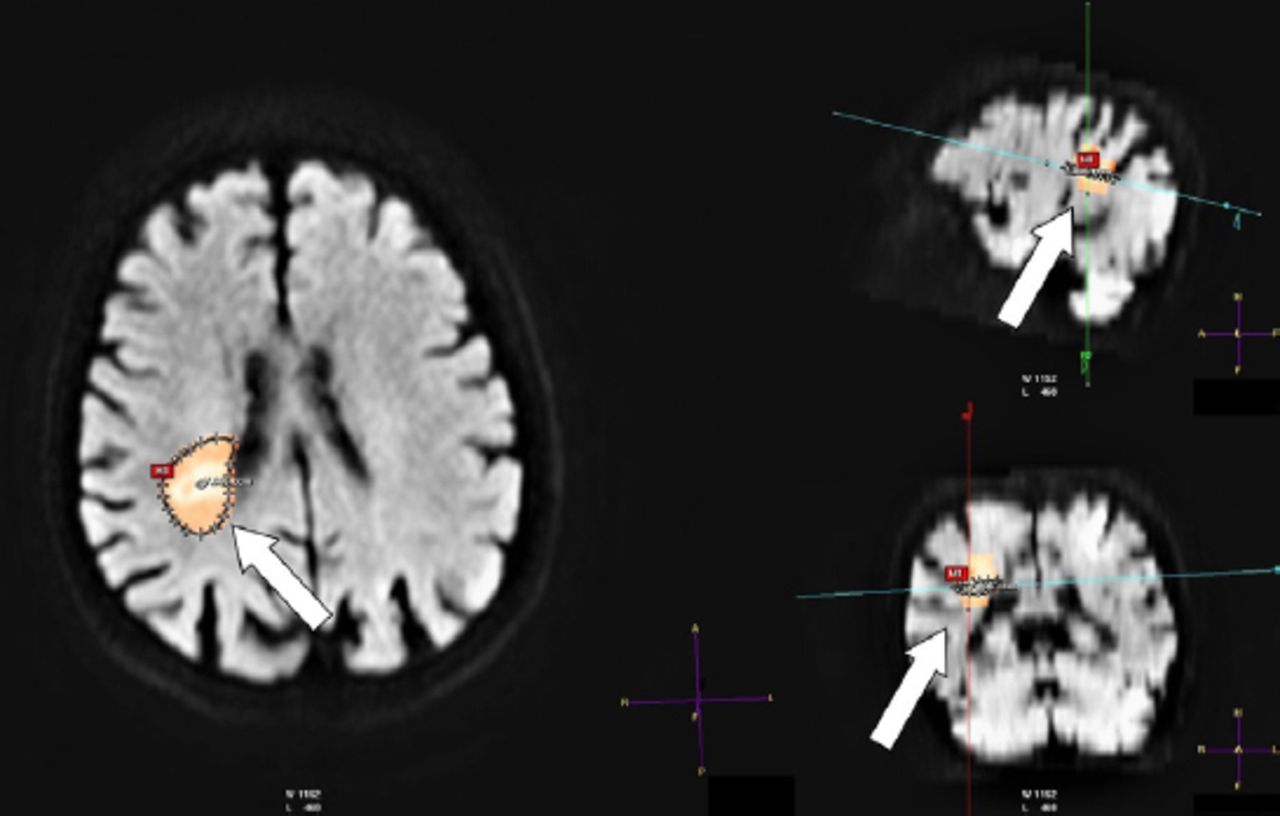
A 1.5 T Philips Achieva machine (Philips Medical Systems, Netherlands) was used for MR imaging. The measurements were taken from diffusion-weighted images obtained with a slice thickness of 5 mm using a b-value of 1000 s/mm2 (Figure 1). Stroke volume measurement was determined using the counter stack tool on a Philips Extended MR Workspace R2.6.3.1. In cases with more than one stroke area, the volume of all possible infarct areas was calculated, and the total volume was recorded. In addition, the affected anatomical location was noted. The stroke volume measurements were taken by a radiologist, with 6 years of experience in neuroradiology, blinded to the clinical findings of the patients.
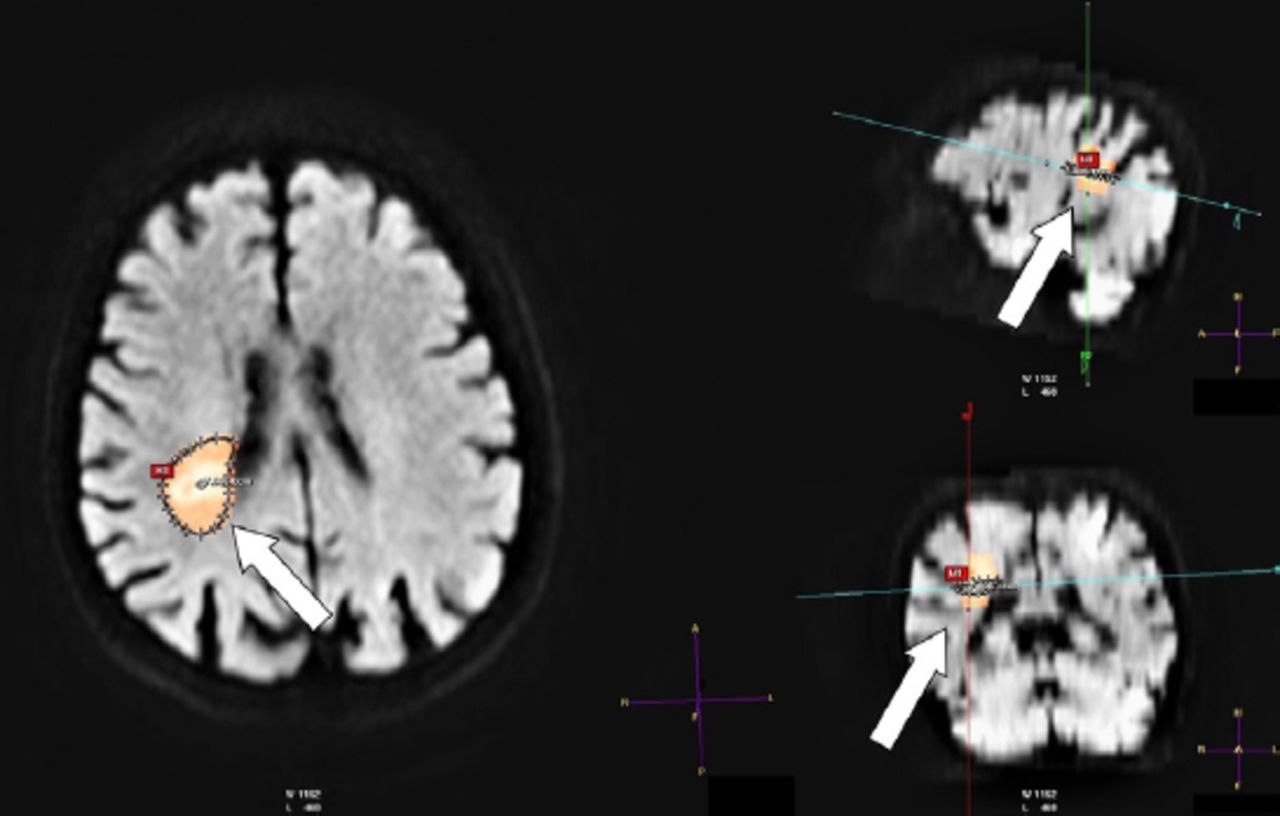
Demonstration of stroke volume measurement on MR work station. Stroke volume measurement is shown on diffusion-weighted axial, sagittal and coronal multiplanar reconstructed magnetic resonance images of an 87-year-old female patient (arrows). Restricted diffusion of the acute infarct area is observed in the right periventricular deep white matter in the centrum semiovale. Stroke volume was calculated as 7.806 cm3.
Statistical analysis
The patients were divided into 2 groups according to whether mortality occurred within one month (a mortality group and a discharged group). The NIHSS score, stroke volume, and blood parameter values were compared between the 2 groups. Categorical data were expressed in numbers and percentages; non-parametric data in minimum, maximum, and median values; and parametric data in mean and standard deviation values. The Mann–Whitney U test and the independent samples t-test were used to compare the numerical data between the groups. For the numerical data that were found to be statistically significant, the sensitivity and specificity were calculated at the optimal cut-off value using a receiver operating characteristic (ROC) analysis. In addition, binominal logistic regression analysis was used in the evaluation of the effect of independent variables on mortality.
Results
A total of 75 patients were included in the study, of whom 34 (45.3%) were male and 41 (54.7%) were female. The mean age of the patients was calculated as 73.23±11.49. At the time of admission, 34 cases (45.3%) were hypertensive, 38 (50.7%) were normotensive, and 3 (4%) were hypotensive. The anamneses of the hypertensive patients revealed that 19 patients (25.3%) had previously experienced hypertension. Fifty patients (66.7%) had a history of diabetes mellitus. In addition, there were 27 cases of cardiac diseases, 10 cases with a history of smoking, and 7 cases had previously had chronic obstructive pulmonary disease. The most frequent symptoms at the time of admission were hemiparesis (42 cases), dysarthria (33 cases), and loss of consciousness (17 cases). Other admission symptoms were seizure (one case), dizziness (3 cases), visual impairment (one case), general condition disorder (8 cases), and headache (one case).
The most common arteries in the irrigation area were the middle cerebral artery in 43 cases, the posterior cerebral artery in 20, the anterior choroidal artery in 7, and the anterior cerebral artery in 4. Twelve cases (16%) were treated in the Intensive Care Unit and 63 cases (84%) received outpatient treatment in the emergency service. The one-month survival rate of the cases was 86.7% (65 cases). At the time of admission, the minimum, maximum, and median GCS scores were 3, 15, and 15, respectively. The minimum, maximum, and median NIHSS scores were found to be 0, 26, and 8, respectively. According to the measurements taken on the diffusion-weighted images, the infarct volume was minimum 0.65 cm3, maximum 67.05 cm3, and median 8.43 cm3.
Table 1 presents the data related to the correlation of mortality with the numerical data and Table 2 shows the results of the ROC analysis on the numerical data having significant differences between the mortality and discharged groups. The data regarding the effects of independent predictors on mortality is summarized on Table 3.
Distribution of numerical data between the mortality and discharged cases.
The results of ROC analysis on the statistically significant numerical data.
Multivariate analysis of predictors of mortality. Multivariable model included all of the following variables: NIHSS score, stroke volume, neutrophil, platelet, WBC, albumin, monocyte/HDL ratio, Ca+, Glasgow coma scale.
Discussion
In this study, NIHSS score, GCS score, stroke volume, neutrophil count, platelet count, WBC count, albumin, monocyte/HDL ratio, and Ca+ were significant for the prediction of one-month mortality. While NIHSS score, GCS score, and stroke volume had the highest sensitivity for a short-term prognosis, an albumin value of <3.65 mg/dL had the highest specificity (100%) but the lowest sensitivity (43.2%) for mortality. In multivariate analysis, none of the parameters showed statistically significant relation with mortality.
Ghabaee et al9 reported that CRP value and NIHSS score had a high sensitivity for mortality prediction in stroke cases. In particular, CRP levels >2.2 mg/L were found to be associated with high mortality in these cases.9 However, in the current study, there was no statistically significant difference between the mortality and discharged groups in terms of CRP levels even though the former group had a relatively higher CRP value (p=0.48).
Previous studies reported that the area of ischemic infarct presenting with restricted diffusion in diffusion-weighted MR imaging is important for the prediction of some neurological deficits as well as for prognosis.10 Similarly, NIHSS score was also shown to be significantly correlated with stroke volume.10,11 Neurological deficits and clinical symptoms were not evaluated in the current study, but it was found that ischemic neural tissue volume showed significant results at 90% sensitivity and 60% sensitivity for one-month mortality. Findings supporting the association of stroke volume with a 90-day prognosis are also available in the literature.4
As revealed in the literature review, stroke volume, NIHSS score, and CRP are among the prognostic parameters that have been previously described. Furthermore, the neutrophil/lymphocyte ratio and the routine blood parameters of blood urea, creatinine, and glucose,11–14 have previously been proven as prognostic markers although they were not evaluated in the current study. Other significant prognostic factors, such as advanced age, dementia, and several chronic comorbidities including heart failure, ischemic heart disease, and atrial fibrillation15–18 have been reported. Moreover, socioeconomic status has been shown to have an effect on stroke mortality.19 The current study demonstrated that WBC, neutrophil count, platelet count, calcium, albumin, and monocyte/HDL ratio were significantly associated with short term mortality. The ESR, LDL, and total cholesterol have been previously reported to significantly predict mortality; however, this study found insignificant results with these parameters.14
This study has certain limitations. Firstly, the low number of patients in the sample may explain why significant results related to CRP values were not obtained, unlike in the reviewed literature. In addition, the low number of patients did not allow for evaluation of the influence of other factors on early stroke mortality, such as old age, previous strokes, and heart disease. Secondly, this study had a retrospective design. Extensive studies based on a prospective design with a higher number of patients should yield more significant results. In addition, a comprehensive meta-analysis of the data available in the literature could provide more valuable and clearer information on this issue.
In conclusion, the clinical, laboratory, and radiological findings individually provide significant support for the short-term prognosis of acute ischemic stroke. The evaluation of these results together can provide a clearer advance understanding of a prognosis to better manage the course of the disease and prevent death.
Acknowledgements
We would like to thank Scribendi for English language editing. and the radiologist Dr. Ibrahim Inan for reviewing the figure 1 for clarity and correctness.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received October 2, 2018.
- Accepted January 23, 2019.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.