


Abstract
Objectives: To assess the outcome and impact of multiple sclerosis (MS) using validated Arabic versions of the Barthel index (BI) multiple sclerosis impact scale (MSIS-29), the modified Rankin scale (mRS), and the expanded disability status scale (EDSS).
Methods: A cross-sectional study conducted at King Abdulaziz Medical City in Riyadh, Kingdom of Saudi Arabia, during July-November 2017. All Saudi adult patients diagnosed with MS between 2000-2016 (269 patients) were included. Patients were contacted via phone calls and were assessed using a newly developed and validated multi-component questionnaire that included demographic data, disease course, and Arabic versions of the scales.
Results: Out of 269 patients, 210 (78.2%) responded. The average patient age was 37.44±10.3 years. The majority were females (69.5%). Only, 51 (24.3%) patients reported worsening conditions. Annually, the average relapse rate was 2.28±1.91. In regard to patient outcomes, 120 (57.1%) showed no significant disability in mRS, 146 (69.5%) were ambulatory without aid in EDSS, and 185 (89.4%) were independent in BI scores. The average MSIS-29-PHYS score was 33.6±27.6 and MSIS-29-PSYCH score was 38.2±25.8. Modified Rankin scale and EDSS were significantly associated with the current use of disease-modifying therapy (DMT). Modified Rankin scale was negatively associated with delayed diagnosis. Barthel index showed significant association with medication compliance and the absence of attacks.
Conclusion: Majority of patients had a favorable outcome that was linked with the use of DMT, compliance, early diagnosis, and absence of attacks.
Multiple sclerosis (MS) is a neurological disease that is singularly characterized by multifocal areas of demyelination in the central nervous system (CNS). Though its precise etiology is unclear, the pathogenesis of the disease is believed to be immune-mediated myelin destruction and, eventually, axon disruption, which is the main cause behind the progressive disability.1 Multiple sclerosis is the most common neurological autoimmune disorder in the world, with an estimated number of 2.3 million until 2013. The increase from 2.1 million in 2008 to 2.3 million in 2013 has raised not only epidemiologists’ interest and alarm but also neurologists’.2 As of Kingdom of Saudi Arabia, it was estimated that 40/100,000 is the prevalence of multiple sclerosis in 2008.3 When it comes to gender, women are generally more affected than men, estimated by a study carried out in Kingdom of Saudi Arabia.4 Affected person’s average age of onset is 30 years.
The outcome and prognosis of MS do not only vary depending on a plethora of factors but are also unpredictable in nature. It is well-recognized in the literature that MS can cause disability with varying degrees, and this can have an impact on patients’ quality of life (QoL) and daily activities.5 However, the outcome is not thoroughly studied, especially in Kingdom of Saudi Arabia. To predict MS patient outcomes, conventional and physician-based validated scales are usually used, one of which is the EDSS. It mainly assesses the degree of disability and monitors the diseases’ progression but with several limitations which are documented, such as its insensitivity to change over a spectrum of 2-3 years.6 Therefore, in this study, we additionally considered other vital scores and scales that not only assess disability via the EDSS, but also the mRS. Moreover, health-related quality of life (HRQoL) is evaluated by the MSIS-29 and the BI. Such measures will help us to have a more objective and reliable endpoint regarding the patients’ outcome and survival.
In this study, we hypothesised that the outcome in regard to disability and HRQoL would differ depending on the variables we took into consideration when assessing MS. Thus, the aim was to evaluate the outcome of this neurological disease that we call MS.
Methods
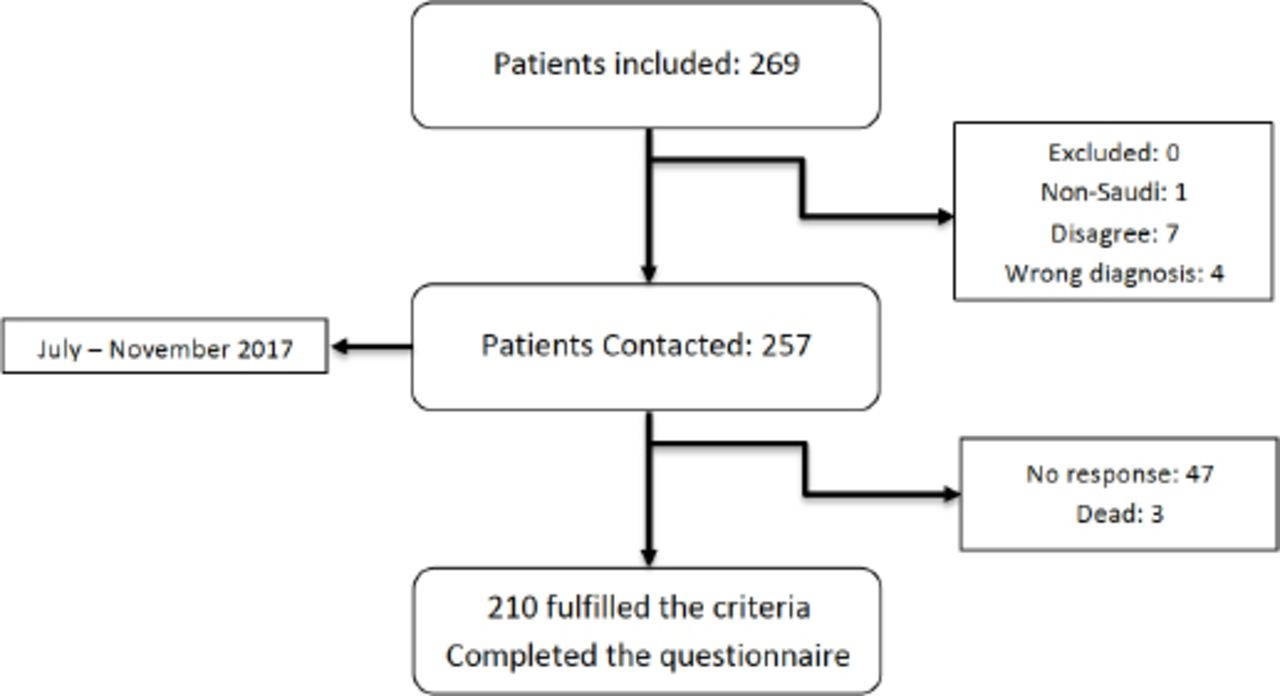
This was a single-centered, cross-sectional study that was conducted in the Adult Neurology Department at King Abdulaziz Medical City in Riyadh, Kingdom of Saudi Arabia, from July-November 2017. King Abdulaziz Medical City is a tertiary care center in Riyadh, Kingdom of Saudi Arabia. All Saudi adult patients who were diagnosed with MS at King Abdulaziz Medical City between 2000-2016 were included, and there were 269 patients. Excluded individuals were individuals not meeting the criteria in a telephone interview, including non-Saudis, wrong diagnoses, and those who disagreed.
The included variables were age, gender, smoking (type, amount, and duration), age at diagnosis, duration of symptoms before diagnosis, number of attacks/Emergency Department admissions per year, current medications (type, duration, and compliance), previous medication, the disease status during year 2015-2016 (improved, no change, worsen, and dead), BI score, mRS score, EDSS score, MSIS-29 score.
Measures
Firstly, the demographic data including age, gender, and age at diagnosis were collected from patients’ charts. Then, the above-mentioned variables were collected after contacting the patients via phone-calls. The duration of symptoms before diagnosis and number of attacks per year were collected, based on the patient’s memory. To determine delay in diagnosis, we considered more than 1.5 year between the disease onset and diagnosis as delayed. Patients’ outcome including HRQoL and degree of disability were assessed by using validated, Arabic versions of the BI of activities of daily living, mRS, EDSS, and MSIS-29.
We developed our own multi-component questionnaire using the aforementioned variables and scales.
Validation
We conducted the validation through 3 phases. Firstly, we translated the English form into Arabic and simultaneously enquired for a non-medical translator to translate it into Arabic. Then, we compared both copies and asked an expert in the field to check them. Secondly, the form was back-translated by another non-medical translator from Arabic to English without access to the original survey, and was later compared with the original. Both copies showed no major differences. Thirdly, pilot testing survey was carried out on 22 people and the final version was edited until no modifications were needed and the survey was unambiguous and understandable.
The validity of the questionnaire was confirmed using Cronbach’s alpha analysis of inte
Expanded disability status scale (EDSS)
Expanded disability status scale is a scale used to assess the degree of disability in patients with MS. Additionally, it is used to monitor the level of changes and the progression over time. It assesses disability through measuring the level of impairment in 7 functional systems (FS) that include cerebral (mental), pyramidal, cerebellar, brainstem, visual, sensory, bowel and bladder functions plus (“other”). The scale ranges from 0-10, and each score represents level of disability. Score 0 indicates perfect health and normal neurological exam, while score 10 indicates death due to MS. Owing to the fact that our study is a phone-call interview and does not include clinical bed-sided exam, patients were assessed using a previously published questionnaire, which is called the nurse-led telephone assessment of EDSS. It is a 12-question form that assesses the disability based on the ability to walk, with or without assistance, for an EDSS of 6 and higher.7 For the patients who needed examination to determine their EDSS score, they were given the term “less than 6”.
At the analysis, the scores of EDSS were grouped into 4 categories: 6 or less implies “Fully ambulatory without aid”, 6.5 to 7.5 implies “ambulatory with aid”, 8 to 9.5 implies “restricted and severely disabled”, and 10 implies “death”.
Modified Rankin scale
modified Rankin scale is a scale widely used to assess the level of disability or dependence in patients’ daily activities. It is commonly used to measure the functional outcomes for patients who have suffered a stroke or other neurological disability. The scale consists of 6 grades, from 0-6, with 0 corresponding to perfect health without symptoms while 6 corresponding to death.8 At the end of the interview, the investigator gave a sutible score for the patient.
At the analysis, the scores of mRS were grouped into 4 categories: 0 and 1 indicates “No significant disability despite symptoms”, 2 and 3 indicates “mild disability”, 4 and 5 indicates “severe disability”, and 6 indicates “death”.
Multiple sclerosis impact scale
Multiple sclerosis impact scale-29 is a patient-based outcome measurement for clinical trials of MS. It is disease-specific and combines patients’ perspective with rigorous psychometric methods. It is made out of 20 physical (MSIS-29-PHYS) items and 9 psychological (MSIS-29-PSYCH) items, measuring the impact of MS. Furthermore, MSIS-29 satisfies all the 5 psychometric criteria (data equality, scaling assumption, acceptability, reliability, and validity), which indicate a significant clinical usefulness and applicability for clinical trials and epidemiological studies. The total score is calculated, and the higher the score reaching 100, the greater the degree of impact on physical and psychological well-being.9
Barthel index
Barthel index is another scale used to evaluate the physical assistance required in activities of daily living (ADL) in patients who had stroke and those with neuromuscular or musculoskeletal disorders. It is scored based on the sum of a patient’s scores in 10 variables describing ADL and mobility, (namely: feeding, bathing, grooming, dressing, bowel control, bladder control, toileting, chair transfer, ambulation, and stair climbing). The items are rated from 0-5, with a lower score suggesting greater impact of the disease on the patient’s physical functioning.10 A cutoff value of 65 was used from a previous study to categorize BI scores into independent (65 or more) and dependent (less than 65).11
Analysis
The Statistical Package for the Social Sciences (SPSS), version 23 (IBM Corp., Armonk, NY, USA) was used for data management and analysis.
Categorical values were reported in terms of percentages, and continuous values were expressed as mean, standard deviation (SD). For testing associations, chi-square was used for categorical data. A bivariate analysis was carried out to examine the association of each scale with gender, smoking, number of attacks/year, delayed diagnosis, current use of DMT, type, and compliance. For continuous data, an independent t-test was used to assess the difference between males and females in terms of age at onset. Odds ratios (OR) with 95% confidence intervals (CI) were reported for significant results. All tests were considered statistically significant if the p-value was less than 0.05.
Ethical considerations
Upon assessing patients’ outcome via phone-calls, the consent was taken verbally in the presence of a witness. Confidentiality is guaranteed, and the data was secured with the primary investigator and co-investigators. Medical record numbers (MRN) and names were not included in the data; serial numbering was used instead.
Results
In all, between a recruitment period of July-November 2017, 269 MS patients were enrolled in this study, 210 (78.2%) of whom responded and completed the questionnaire (Figure 1).
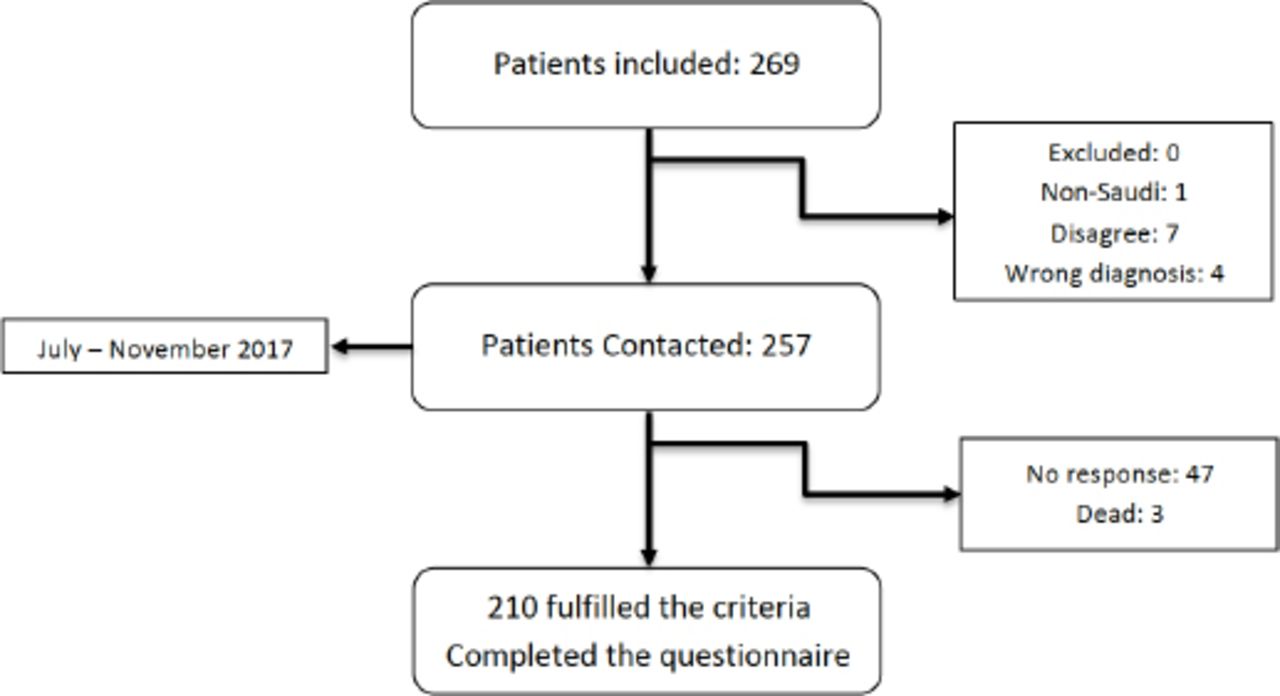
Data collection flowchart.
Table 1 presents the demographic characteristics of the study sample in detail. The mean age at diagnosis was 22.89±11.9 years old with no significant difference in terms of gender female [M±SD=22.9±11.98] and male [M±SD=22.8±11.6], conditions; p=0.96. Additionally, each scale was analyzed separately (Table 2).
Distribution of characteristics of study subject (N=210).*
Univariate analysis of mRS, EDSS, BI, and MSIS-29 (N=210).
Tables 3, 4, & 5 present the bivariate analysis of mRS, EDSS, and BI with several variables.
Distribution of Saudi MS patients according to mRS (N=207).
Distribution of Saudi MS patients according to EDSS (N=207).
Distribution of Saudi MS patients according to BI (N=207).
A statistically significant correlation was found between high scores of mRS and delayed diagnosis (OR=0.395; 95% CI=[0.176-0.885]; p=0.025). Scores of BI were significantly low with absence of recurrent attacks of MS (OR=0.47; 95% CI: [0.194-1.2]; p=0.054). A statistically significant correlation was found between low scores of EDSS with use of DMT (OR=2.4; 95% CI [1.01-5.83]; p=0.042). Similarly, low scores of mRS were positively correlated with use of DMT (OR=3.2; 95%CI [1.4-7.12]; p=0.002). There was a significant association between medication compliance and BI (OR=2.9; 95% CI: [0.8-10.4]; p=0.044). Regarding gender, smoking, and type of DMT, there was no significant association with any of the scales.
Discussion
In this study, we assessed the disability and HRQoL via 4 major scales. We also examined the variables separately and explored their association with the scales. We compared the demographics of the present study with 2 other works carried out on similar sample sizes of MS patients. Our mean age at diagnosis was 22.89, which is consistent with previous studies. Similarly, two-thirds of the population were females.12,6 In addition, we found that the most commonly used DMT during follow-up was interferon beta-1a (Rebif ©), one of the earliest treatment used in MS.13 The average number of attacks/year was lower (0.65) compared to our study (2.29).12 However, when patients were asked about the yearly number of attacks, it was mainly memory dependent. Sixty one point eight percent had no attacks in the previous year; therefore, it could be vulnerable to recall bias and over-estimation.
When comparing the results of each scale separately with other international studies, the average MSIS-29-PHYS score showed better physical outcome of our patients compared to one of the largest cohort studies whose average was 62±20.5. However, our population had a slightly higher average MSIS-29-PSYCH score compared to 23.6±8.7.6 With that being said, we can infer that our patients had a greater psychological impact compared to international results. Moreover, this can be explained by another local study that had similar findings; the study was carried out to assess the QoL of MS patients in Kingdom of Saudi Arabia and some Arab contraries. They concluded that out of 382 MS patients, 32.2% had an impact on their psychological well-being in several aspects, including feeling depressed and nervous, as well as being inattentive.14
In regard to the BI results, the majority of our patients were independent with a mean of 76.2±13.9. In comparison, Nicholl et al15 reported a BI mean of 84.0±17.0 in 90 adult MS patients, which is considered slightly better. Moreover, in CombiRx, a double-blinded, 3-year clinical trial that assesses mRS, the mean score was 1.0±0.7, which corresponds with no significant disability despite symptoms.16 Likewise, the majority of our patients had no significant disability despite symptoms. While a retrospective study of 76 MS patients had a 67% of severely disabled patients in EDSS, the majority of our patients were fully ambulatory without aids.17
In terms of scales, our data showed that the majority of patients had generally good outcomes. This is linked significantly with the use of DMT, medication compliance, early diagnosis, and the absence of attacks. On the other hand, we could not interpret the significant p-value when comparing the scales with gender and smoking. This might be due to the small number of males when compared to females as well as smokers to non-smokers.
In total, 72% patients did not have delayed diagnosis. Our data showed that delayed diagnosis is significantly associated with disability. In contrast, no association was found by Marrie et al18 in this regard. Overall, 61.8% of our patients had no attacks in the previous year. The absence of attacks was significantly associated with BI. There is a theoretical hypothesis which proposes that preventing relapses can prevent disability. In one study, they correlated the frequency of relapses in the early phase of the disease with the degree of disability, in which they found a significant association. Moreover, upon interpreting the current use of DMT, the majority (77.8%) of the patients were on DMT with a significant association between DMT use and better outcomes with regard to some scales. On the other hand, in a previous study of 367 adult MS patients, no significant association was reported. They found that both treated and untreated patients had a similar average of EDSS scores.19 Moreover, 79.9% of our patients were compliant to their medications, which positively impacted their activities of daily living as it was significantly associated with BI, meaning 89.8% of independent patients were compliant.
In summary, we observed that our patients had good physical and psychological QoL with no significant disability or major impact of the disease on their activities of daily living. In contrast to another study conducted in Kingdom of Saudi Arabia, HRQoL and disability were assessed in 598 MS patients, in which they reported low score in HRQoL measures and a considerable disease impact that was correlated with significant disability.20
The present study has a number of limitations. Firstly, it was carried out with a small sample size; therefore, some of the variables were not interpreted sufficiently. Hence, further studies with a larger sample size are recommended to examine the association of outcome with other factors and variables like gender and smoking. Secondly, the data was collected through interviewing patients via phone-call, so disability and health status were self-reported. Lastly, our study could be vulnerable to recall bias during phone calls mainly for the memory-dependent questions (For example, average numbers of attacks).
In conclusion, the majority of our patients had a favorable outcome, which was significantly linked with the use of DMT, compliance, early diagnosis, and the absence of attacks. Moreover, our data showed a slightly higher impact of the diseases on psychological well-being compared to international literature. Therefore, attention and care should be directed towards patients chronically suffering from a disease like MS. Furthermore, as a future implication in research and clinical settings, this multi-component questionnaire can be used as an integrated system to monitor disease progression for early intervention and better outcome.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received December 18, 2018.
- Accepted March 19, 2019.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.