


Abstract
Objectives: Objectives: To examine the knowledge and awareness of brain death among the Saudi population and to identify what is needed to improve awareness in this community.
Methods: We conducted a cross-sectional study across various regions of the Kingdom of Saudi Arabia from July-December 2018. Data was collected from a sample of the general population via a questionnaire, which obtained sociodemographic data and included questions about assessments and guidelines for brain death. We conducted descriptive statistics, as well chi-square tests to compare between groups, with statistical significance considered at p≤0.05.
Results: We recruited 1244 participants with a mean age of 27.17±9.84 (female: n=992; 79.7%, male: n=252; 20.3%). Of these, 1208 (97.1%) were Saudi, 444 (35.7%) were married and 800 (64.3%) were single. The majority had a university degree (n=837; 67.3%), 676 (54.3%) were currently students, approximately a third of whom were from health specialties (n=393; 31.6%), and 192 (15.4%) were unemployed. A mean score of knowledge of 5.53±2.61 was observed, equivalent to 42%. There was a significant difference in total knowledge score depending on marital status, region, and educational level and specialization. In contrast, there was no significant difference in knowledge depending on gender, age, nationality, or place of work.
Conclusion: Our results suggest that Saudi Arabians have little to moderate knowledge about brain death. Education and work-based awareness programs about brain death are needed, particularly regarding prevention and causes.
From the creation of the first human to the end of the times, death is a great certainty and forms a guaranteed part of human life, it is an inevitable end for all things created from mankind to the animal kingdom and from the smallest planet in the galaxy to the largest stars. For mankind the concept of brain death has been a recent development in the last 50 or so years and the understanding of this subject has been a controversial matter for all medical practices across the globe.
There are many definitions of brain death, the most common of which was provided in the 1980s by the American Medical Association. They defined brain death as either “irreversible cessation of circulatory and respiratory functions, or irreversible cessation of all functions of the entire brain, including the brain stem”.1 Brain death is determined according to neurologic criteria. Specifically, the diagnostic criteria include the loss of brainstem reflexes and the proof of apnea, as well as coma.2,3 A patient with brain death differs from a patient in a coma because in the latter there is residual functioning of the brain stem, which continues to control breathing. In contrast, brain death is medically recognized as actual death.
The most common cause of brain death is an illness such as a brain tumor, stroke, aneurysm, or anoxia. Other common causes include accidental injuries from a fall, gunshot, or car accidents. Ancillary methods commonly used to confirm the diagnosis of brain death are cerebral angiography, electroencephalography, transcranial doppler ultrasonography, and cerebral scintigraphy.4,5
The Saudi center for organ transplantation has reported that since the start of organ donation from 1986-2016 that there have been 11866 cases of brain death.6 In 2016, 646 cases were reported at different intensive care units across the Kingdom of Saudi Arabia. In the last 5 years, a mean annual rate of 606 deaths of individuals aged less than 40 years was reported, with a ratio of men-women of 3:1. Among these, 45% of cases were caused by head trauma and 55% by vascular accidents.
Our research focuses on raising awareness in the subject matter of brain death and in order to emphasize the vital importance of organ donation. Organ donation is critical in providing a means that can effectively give an opportunity in improving human lives and to provide a chance for healthier and improved living conditions. There is a distinct lack of knowledge and information about brain death amongst the Saudi population and no real understanding exists to provide medical criteria on the subject matter.7
The population does not have a clear and precise concept of brain death and this concept is confused and compared with the deep coma state. Our aims are to investigate and conduct analysis in the following area; to understand how much knowledge and awareness of brain death among a large representative sample of the population of the Kingdom of Saudi Arabia exists. If the data highlights that such knowledge exists and is understood, then perhapsis impact as people will know that a patient has died and as such will not need to remain or be kept alive using medical equipment and hence, it would follow on that a financial burden does not have to be borne as the medical equipment is not required and will not increase a patient’s lifespan as a person is clinically dead in the matter of brain death. Similarly the financial cost savings for hospitals and medical centers as the medical equipment will not be required.
Methods
Study design
We conducted a cross-sectional study to assess knowledge and awareness of brain death among the general population of kingdom of Saudi Arabia. We recruited 1244 participants to complete a questionnaire either online or during an interview between July-December 2018. We compared knowledge and awareness of brain death between groups based on demographics namely, age, gender, and education level).
The study protocol was approved by the research ethics committee at Taif University in Taif, Kingdom of Saudi Arabia (application number: 39-36-0046). Prior to data collection, all participants were informed about the nature of the study and that their participation was voluntary. Subsequently, electronic consent was obtained from those who agreed to participate. All included participants were over 15 years old.
Questionnaire
All of the respondents provide an answer to each of the questions in the questionnaire. There are no available validated Arabic brain death questionnaires. Therefore, we used items from validated assessments of coma to create a questionnaire that was translated from English to Arabic. The survey included 2 parts; the first part included questions to obtain sociodemographic data (age, gender, marital status, nationality, residential region, education level, employment, and educational specialty); the second part included components of the Glasgow coma scale (GCS) and the FOUR score scale, which are diagnostic tools for coma. Specifically, we asked about the most prominent signs of brain death from the perspective of the GCS and FOUR score.8,9 This included response to any stimulus, response of the patient to light, reaction to pain, eyes moving when head is moved, and breathing without a ventilator.
Moreover, we included items based on the update of the American academy of neurology (AAN) guideline for determining brain death in adults.5 The principles for this guideline were derived from the definition of brain death provided by the Uniform Determination of Death Act (UDDA). The UDDA-derived principles define the essential elements needed to determine brain death. Accordingly, we asked participants about criteria required to determine cessation of all functions of the entire brain, including the brain stem. Such criteria included the presence of unresponsive coma, absence of brainstem reflexes, and absence of respiratory drive after a CO2 challenge. In addition, loss of brain function must be irreversible (namely, the state cannot be cured).
Although these criteria have been laid out in the AAN guidelines, a lack of evidence means that clinicians must exercise considerable judgment when applying the criteria in specific circumstances. Therefore, we also asked about which physician is authorized to give a reliable diagnosis of brain death and whether respondents consider it a reliable diagnosis or not. Moreover, to confirm that cessation of brain function is irreversible, physicians must determine the cause of coma, exclude differential diagnoses that may mimic brain death, and observe the patient for a period of time to exclude the possibility of recovery. We also asked about the most common causes of brain death. Anyone can complete our survey, there was no special criteria for participant.
Several tests are used to confirm a diagnosis of brain death. Important tests used to confirm diagnosis include the apnea and ancillary tests (only one needs to be performed), which are conducted only if clinical examination cannot be sufficiently performed due to patient factors. Further tests must be used if apnea testing cannot be completed, including cerebral angiogram, Tc-hexamethylpropylene amine oxime single-photon emission computed tomography (HMPAO SPECT), electroencephalography (EEG), and transcranial doppler ultrasound (TCD). Furthermore, within the questionnaire, we used concepts of brain death derived from studies by Yousefi et al,2 and Nowaka et al.3,10
Questionnaire scoring
To measure awareness, we asked 8 questions derived from items in the GCS, FOUR score and AAN guideline.5,8,9 If the participant chose the correct answer, they scored a point. If they chose the wrong answer, no points were gained. We have given 12.5 for each question when the participant answered correctly as a coefficient of calculating. We developed this way in calculation for this study and it was made by used validated assessment (GCS, FOUR scores and AAN guideline).
Data collection
The translated questionnaire was administered by trained medical students via interviews with the general public in malls, hospitals, primary healthcare centers, universities, and schools. Moreover, the questionnaire was available online (https://goo.gl/forms/UEqrEMbmnzyXKilR2), and was shared through social media applications such as WhatsApp, Telegram, Twitter, Facebook, and Instagram.
Data analysis
Data was entered into Microsoft Excel 2010 when collected and subsequently coded for analysis with Statistical Package for the Social Science (SPSS) Version 21.0 (IBM Corp, Armonk, NY, USA). We initially conducted descriptive statistics, before using chi-square tests to compare between groups. A p≤0.05 was considered significant.
Results
Most respondents had received information regarding brain death from social media or the internet (n=660; 53.1%), with the next most common sources being television (n=175; 14.1%), and books (n=142; 11.4%) (Table 1). Moreover, most respondents did not have a history of brain death among their relatives (n=823; 66.2%).
Socio-demographic information of the participants (N=1244).
Table 2 presents the questions regarding definitions of brain death that we asked participants. We observed that 957 (76.9%) answered correctly that brain death is an irreversible loss of brain function, 278 (22.3%) believed that brain death is a reversible loss of brain function, and only 9 (0.7%) said that brain death is loss of heart function. About 24% of respondents had no idea about the cause(s) of brain death. However, the remaining 76% identified road traffic accidents, heart attacks, and strokes as causes of brain death.
Responses of participants to questions testing their knowledge of brain death (N=1244).
We found that 835 respondents (67.1%) correctly agreed that brain dead patients can donate their organs, while 144 (11.6%) said they could not, and 265 (21.3%) did not know whether brain dead patients can donate organs. Only 264 respondents (21.1%) incorrectly responded that brain dead patients can be cured, 539 (43.3%) said it cannot be cured, and 443 (35.6%) did not know whether a brain dead patient could be cured. Only 26% of respondents thought that brain death was real death. Nonetheless, the majority of respondents (79.3%) agreed that brain death is different from a coma.
In terms of the signs of brain death, the highest number of respondents identified that the patient does not breathe without a ventilator (n=551; 44.4%) and that the patient does not show any reaction to pain (n=411; 33.1%).
Only 184 respondents (14.8%) knew that a neurologist is the clinician capable of determining brain death. Moreover, when we asked “Do you consider brain death to be a reliable diagnosis?” 431 participants (34.6%) responded ‘yes’, while a similar number responded ‘I don’t know’.
The mean knowledge score was 5.53±2.61. Table 3 shows differences in total knowledge scores between groups. The results suggest a significant difference in total knowledge score depending on marital status, region, educational level, and higher education specialization. Higher scores were observed in those who are single (5.85) than in married respondents (4.96), (p=0.01), in those living in central regions than in other regions (p=0.01), in those educated to university level than in those with other educational levels (p=0.019), and in those within health specialties compared with other specialties (p=0.001). In contrast, there were no significant differences in knowledge scores based on gender, age, nationality, and place of work.
Significant relationships between knowledge scores and demographic variables.
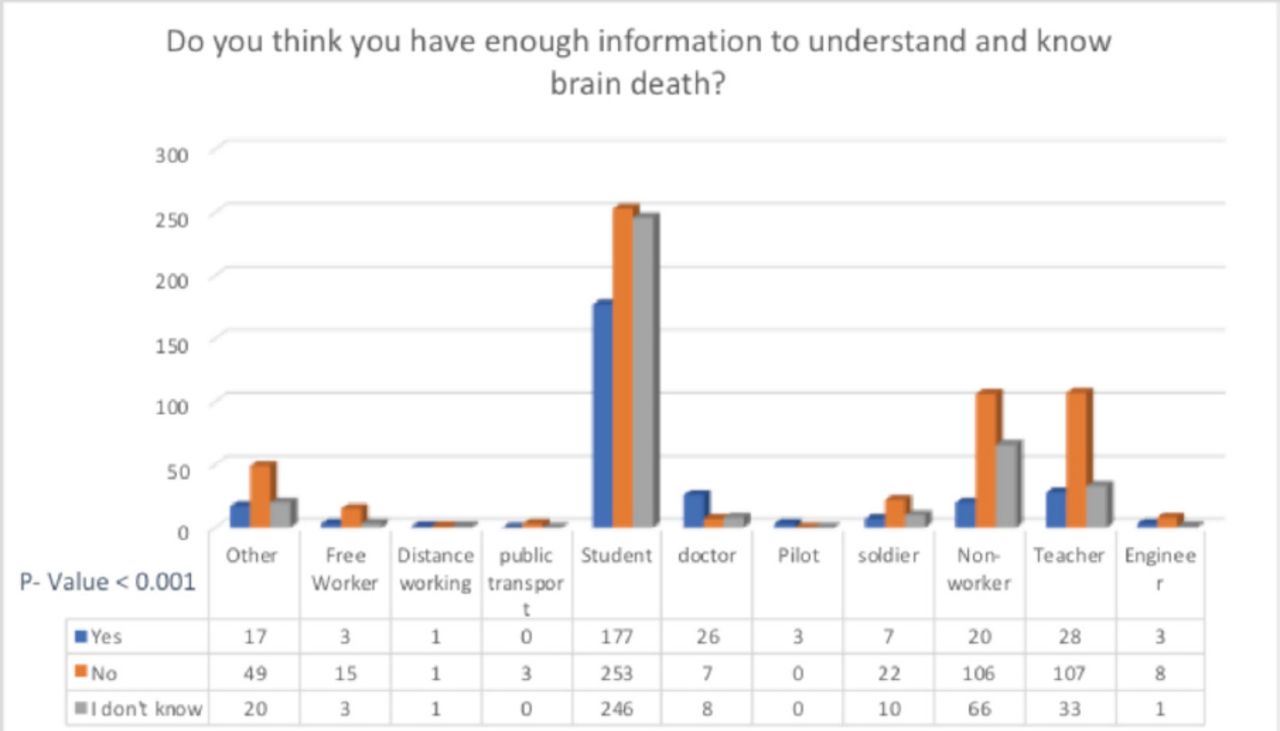
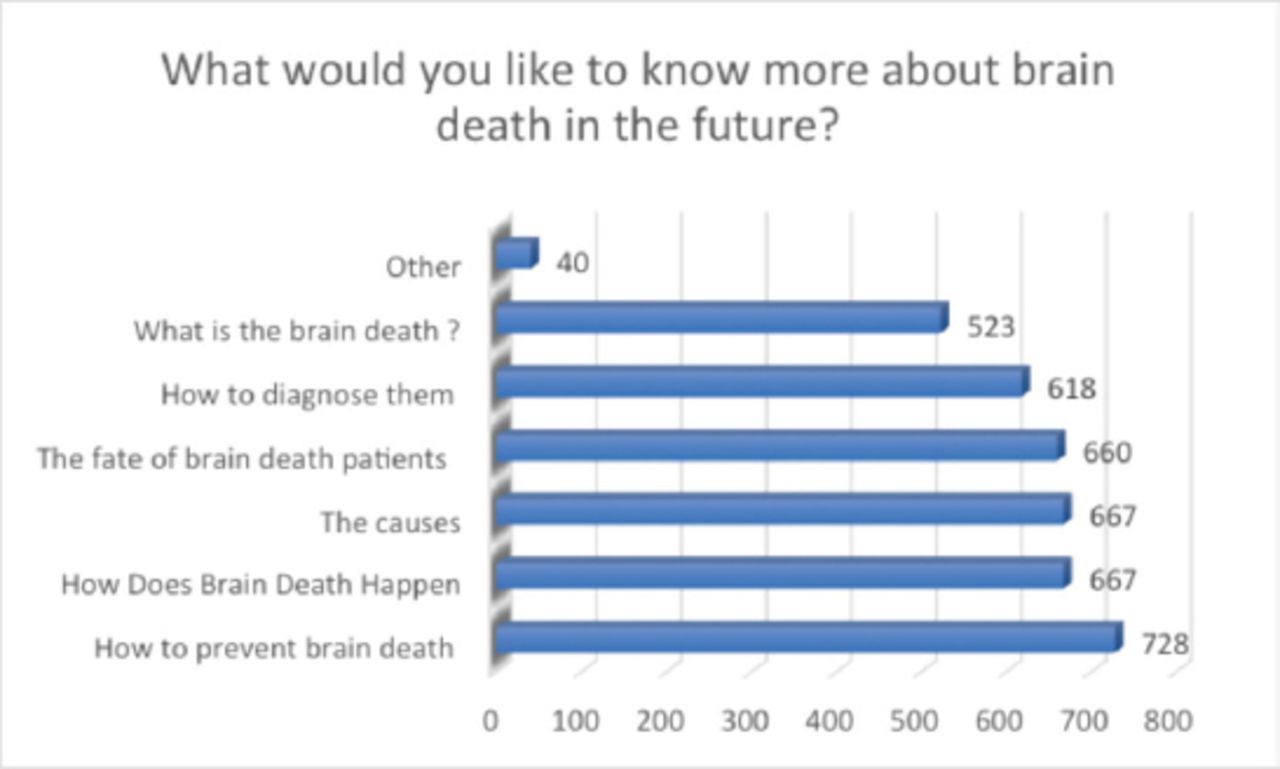
We conducted a chi-square test to assess associations of knowledge of brain death with both educational specialization and workplace. The results suggest that physicians and health practitioners have more knowledge than other participants for each question (p<0.001). Most felt they did not need more information to understand brain death (Figure 1). Moreover, 1108 participants (89.1%) would have liked to have more information about brain death (Figure 2), especially regarding the prevention and causes of brain death.

Significant relationships between a participant’s workplace and having enough information about brain death.

Response of participants in need to BD additional information.
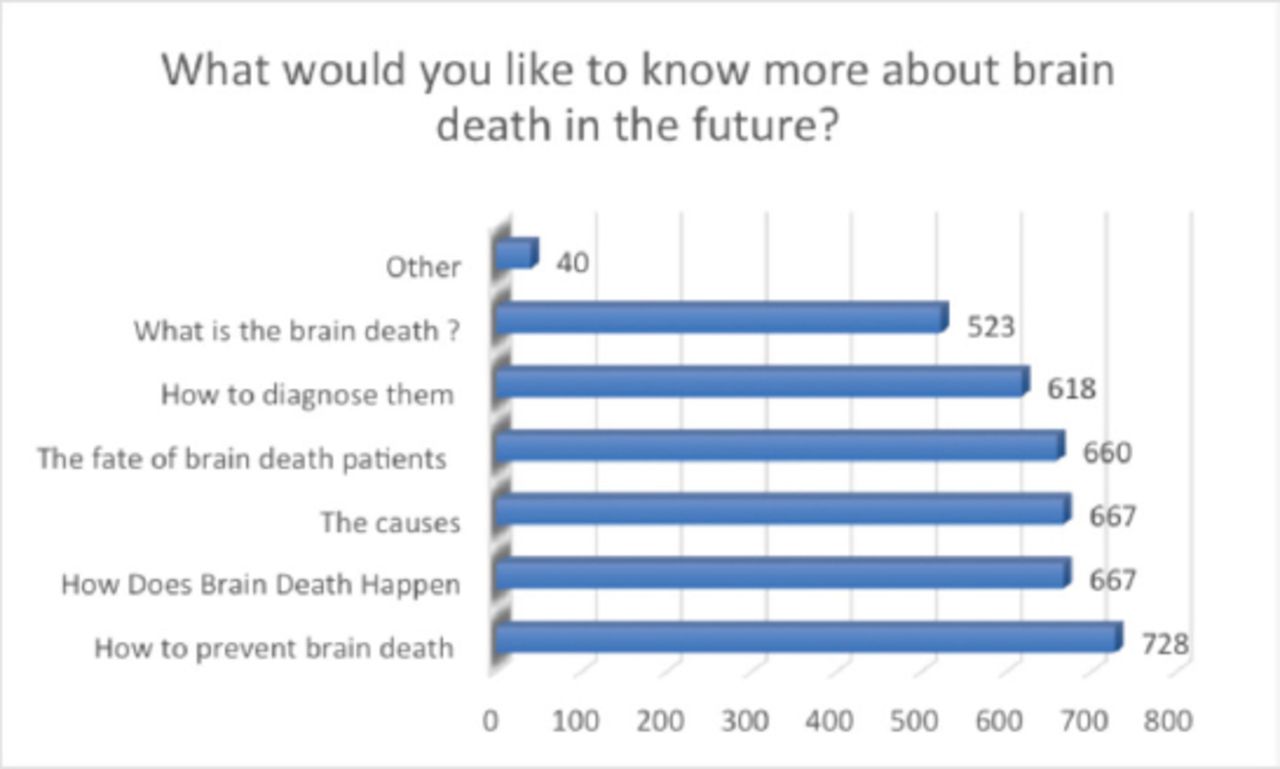
Numbers of participants who would like more information about brain death.
Discussion
There is limited public understanding of brain death, which can have several deleterious effects, including influencing organ donation. Therefore, in this study, we aimed to assess the current knowledge of brain death among the general population of Kingdom of Saudi Arabia. Most previous studies have not focused specifically on awareness of brain death, but rather its association with knowledge, attitudes and practice (KAP) regarding organ donation.
Moreover, there was no available validated Arabic questionnaire about brain death for use in this study. Therefore, we designed a questionnaire based on validated assessments that was subsequently translated from English to Arabic. We based our questionnaire on the summary of the AAN guideline and 2 other internationally approved assessments (the GCS and FOUR score). Our results suggested a mean knowledge score of 5.53±2.61, which was almost equivalent to 42%. This suggests that the general public in Kingdom of Saudi Arabia have little-moderate knowledge about brain death. This is similar to knowledge levels reported previously, in which just under half of surveyed men and women had sufficient awareness of organ donation and brain death.11 However, it is in contrast with 2 other studies conducted in Turkey and Iran which reported poor awareness and a need to improve knowledge of brain death and organ donation.12,13
Several studies of awareness of organ donation and brain death have been conducted in Kingdom of Saudi Arabia with university students, secondary school students in the south and in Al-Ahsa.7,14,15 Knowledge of brain death has been reported to be inadequate, and these studies have highlighted the importance of increasing awareness of brain death to improve the knowledge among Saudi people.
We observed that 76.9% of participants knew the concept of brain death, which is higher than that reported by Febrero et al16 in which only 38% understood the concept of brain death. However, this figure is lower than that in the AL-Ahsa study (84.6%).7 We also observed that 21% of participants thought that a brain dead patient could be cured. This is slightly less than the figure of 22.5% reported by Bshabshe et al.14 In contrast, the majority of participants in a study by Bormand et al17 believed that rebirth after brain death could be possible.
We also observed that 67.1% of participants were aware that a brain dead patient can donate his/her organs compared with 60.7% in the Al-Ahsa study.7 Meanwhile, more than the half of participants in our study consider brain death as real death, and 79.3% noted that there is a difference between brain death and coma.
We observed that some demographic variables influenced the knowledge scores of participants. For example, single individuals (5.85) had significantly higher scores than did married participants (4.96), (p=0.01), (Table 3). This may possibly be due to the higher number of single participants than married participants in our sample (making up 64.3% of respondents). We also observed that respondents from central regions had the highest mean knowledge score compared with the other regions (5.79±2.65; p=0.01), (Table 3). This was despite the fact that the largest proportion of participants were from the Western region (45.9%), but this was applicable with the Saudi Ministry of Health Annual statistical book 2017, which shows the highest numbers of Hospitals, beds including the specialty beds (intensive care and neurology), resources, and total manpower in the central region of Kingdom of Saudi Arabia.18
Finally, as might be expected, those with a university degree had the highest mean knowledge score (5.73±2.62; p=0.019). Moreover, physicians and health practitioners had the highest knowledge scores compared with other specializations (p<0.001). They are more likely to have encountered brain death or to have studied the concept, meaning that they do not need additional information about brain death due to the nature of their specialties. There were no significant relationships between knowledge scores and the other sociodemographic variables (namely, gender, age, and place of work).
The strengths of our study include the large sample, the coverage of all regions in Kingdom of Saudi Arabia, and the use of a validated Arabic questionnaire based on the GCS, FOUR score, and AAN guideline.
Limitations
the study is subject to some limitations, including the fact that a higher proportion of participants were female (79.7%), and a low proportion were younger (9.1%), while a large proportion were from the Western region (45.9%). These proportions suggest that the sample may not be completely representative of the general population. Indeed, future studies should attempt to recruit participants from different regions of the country in equal proportions for more accurate results and can be generalized in all of the community. As will be noted, the number of women participating in the questionnaire is very huge compared to men and may be due to the time when the sample was collected or perhaps its location and this may be considered a kind of potential bias.
In conclusion, our results suggest that among the general population of Kingdom of Saudi Arabia there is little-moderate knowledge of brain death. Therefore, we suggest that awareness of brain death in the Saudi population could be improved by using various mass media resources. Moreover, education and work-based awareness programs about brain death are needed, particularly regarding prevention and causes.
Acknowledgements
The authors gratefully acknowledge editage (https://www.editage.com) for English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received December 4, 2018.
- Accepted March 6, 2019.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.