


Notice: Authors are encouraged to submit clinical images for possible publication in the Journal. These may be in any field of Clinical Neurosciences, and should approximately follow the format used here. Please address any submissions to the Assistant Editor, Neurosciences Journal, Prince Sultan Military Medical City, PO Box 7897, Riyadh 11159, Kingdom of Saudi Arabia. E-mail: malaskar{at}psmmc.med.sa
Isolated oculomotor nerve palsy secondary to fascicular midbrain infarction
Clinical Presentation
A 52-year-old man with a past medical history of uncontrolled hypertension and diabetes mellitus presented with acute onset of drooping of the right upper eyelid and double vision on looking to the left side. He had no other associated ocular or neurological manifestations. Neurological examination showed a fully conscious and oriented gentleman with normal speech and higher mental functions. Cranial nerves assessment showed ptosis of the right upper eyelid with downward and outward deviation in primary gaze. Extraocular movements assessment is shown in Figure 1. Right pupil was dilated with very sluggish reaction to direct and consensual light; 7.5 mm (Dark), 7 mm (Light). He did not exhibit Bell’s phenomenon. Otherwise, his motor, sensory, cerebellar and gait assessment were normal. Magnetic resonance imaging (MRI) of the brain is shown in Figure 2.

Photographs of 9 cardinal positions of gaze showing right upper eyelid partial ptosis and exotropia in primary gaze, limited adduction and impaired vertical voluntary gaze (upward gaze more affected than downward gaze) on the right side. Dilated right pupil cannot be seen.
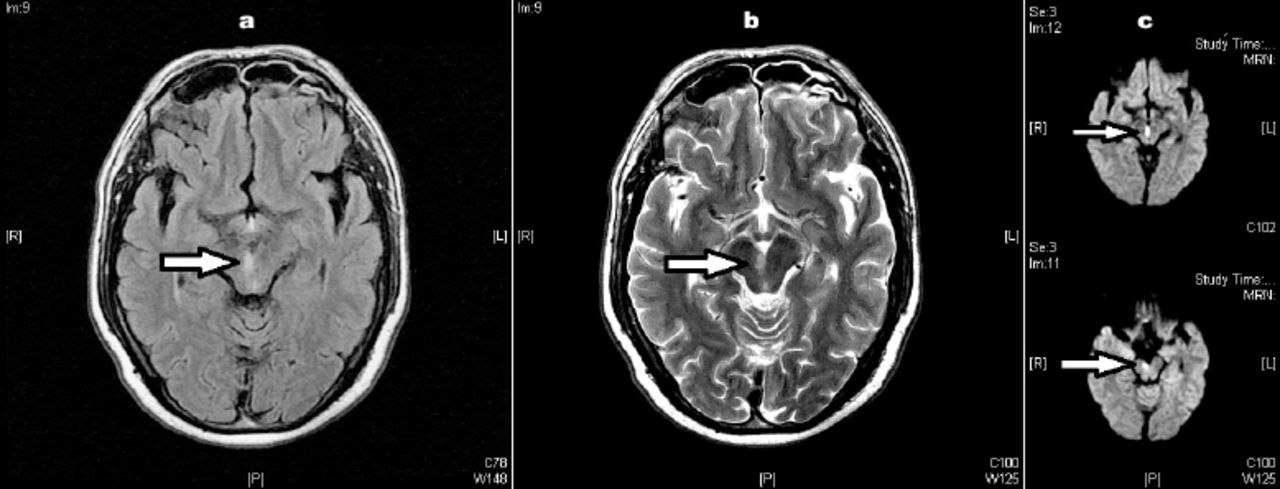
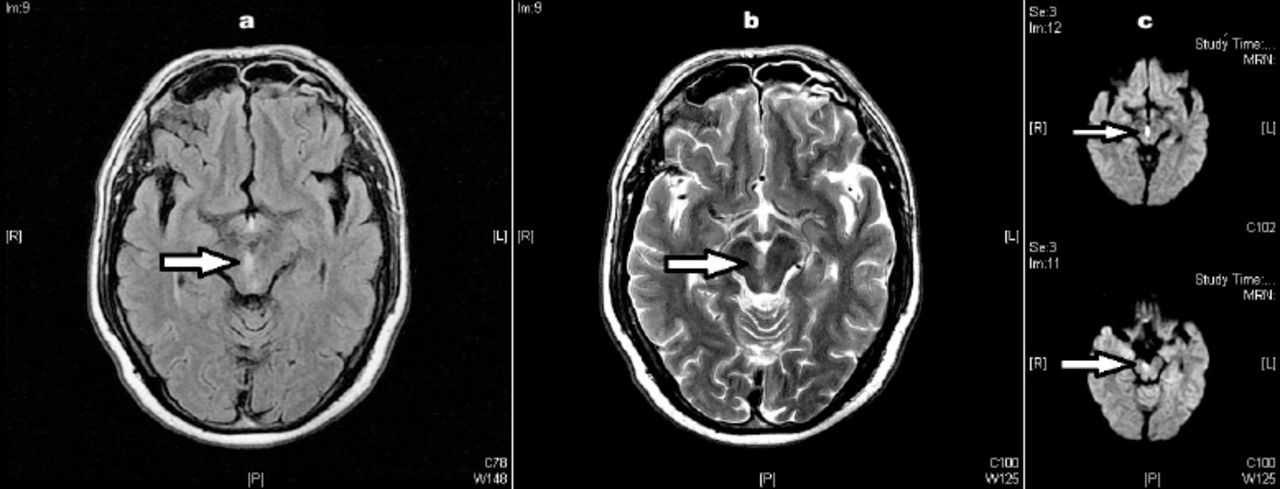
MRI of the brain at the level of the midbrain; a) axial FLAIR, b) axial T2-weighted images and c) diffusion-weighted images (DWI) showing an ischemic lesion (arrow) in the paramedian upper midbrain tegmentum involving the oculomotor fascicles on right side.
Questions:
What are the clinical features of oculomotor nerve palsy?
What are the differences between nuclear and fascicular midbrain lesions?
What are the common syndromes usually associated with fascicular midbrain lesions?
Answers & Discussion
Oculomotor nerve palsy is an important and common clinical finding. Its main features are diplopia and ptosis secondary to affection of the levator palpebrae superioris, superior rectus, medial rectus, inferior rectus, and inferior oblique muscles. It also innervates the iris sphincter and the annular portion of the ciliary muscle through its parasympathetic fibers resulting in fixed dilated pupil if affected.1 The nuclei of the third cranial nerve originate at the level of the superior colliculus. The oculomotor fascicles run ventrally and laterally from the oculomotor complex, pass through and medial to the red nucleus and exit the brainstem medial to the cerebral peduncles.2
A third nerve palsy due to midbrain infarction results from either nuclear or fascicular lesion. Such lesions can usually be differentiated clinically. The subnucleus of the levator palpebrae superioris, the central caudate nucleus, is single and midline, and the fibers to the superior rectus muscles originate in paramedian nuclei and provide crossed innervation. Lesions of the oculomotor nucleus would result in bilateral ptosis and contralateral upward gaze palsy. However, lesion affecting fascicular fibers, as in our patient, will result in unilateral palsy mimicking a peripheral third nerve lesion. Pupillary affection in such cases is variable, but its involvement is more common.3
Several syndromes have been recognized with fascicular lesions including: Weber syndrome, Benedikt syndrome, Nothnagel syndrome and Claude syndrome. Rarely, fascicular lesion of the third cranial nerve develop in isolation without involvement of adjacent midbrain structures as in our patient.4
Acknowledgment
The authors would like to thank Dr Ehab Abdelnabi, Neuroradiologist, Ibn Sina Hospital, for clarity and correctness.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue




{kind=link}
{kind=link}
Related Articles
Cited By...
- No citing articles found.