


Abstract
New-onset refractory status epilepticus (NORSE) is a drug-resistant status epilepticus that often has a catastrophic outcome. Our patient was diagnosed with NORSE and had an EEG reading that showed status epilepticus persisting for 8 months in general anesthesia. After autoimmune workup showed positive antiphospholipid antibodies, his seizure was controlled, and he was discharged with good condition apart from moderate cognitive impairment. However, he later developed schizophrenia. Although psychiatric disorders have been associated with antiphospholipid syndrome, to the best of our knowledge, it has not been reported to be associated with status epilepticus. We recommend vigilance of psychological complications of refractory status epilepticus’ patients for early psychiatric referral, diagnosis, and treatment.
New-onset refractory status epilepticus (NORSE) is a syndrome of new-onset drug-resistant status epilepticus that often has a catastrophic outcome. Epilepsy is usually associated with psychiatric disorders of different manifestations of which psychosis is an example.1 However, not much is found in the literature review regarding psychiatric disorders following NORSE although a recent study concluded 32% of NORSE patients ended up with altered behavioral states like aggression.2 Schizophrenia following NORSE like in the rare presentation of this case has not been reported in the literature review before, although an association between schizophrenia and autoimmune disorders like APS has been reported.3
Case Report
Patient information and clinical findings
A 41-year-old, nonsmoker, married man works in a college with no past relevant family or medical history. He had blurry vision and headache, and after 2 hours he developed generalized tonic-clonic seizure. He was brought to the local emergency department where benzodiazepine and 2 antiepileptic drugs loading doses failed to stop his seizures. Midazolam boluses as a continuous infusion over 5 days were then administered. Although the medications’ doses were increased, his seizure was drug resistant. He was then intubated, and propofol, midazolam, fentanyl in addition to the maintenance medication valproic acid, phenobarbitone, levetiracetam, and phenytoin were administered.
Diagnostic assessment and therapeutic intervention
He was given empirical antibiotics although the workup findings of CT scan and brain MRI performed at the local hospital he first presented in were normal, including the lumbar puncture which only showed slightly elevated white blood cells with normal protein and glucose levels.
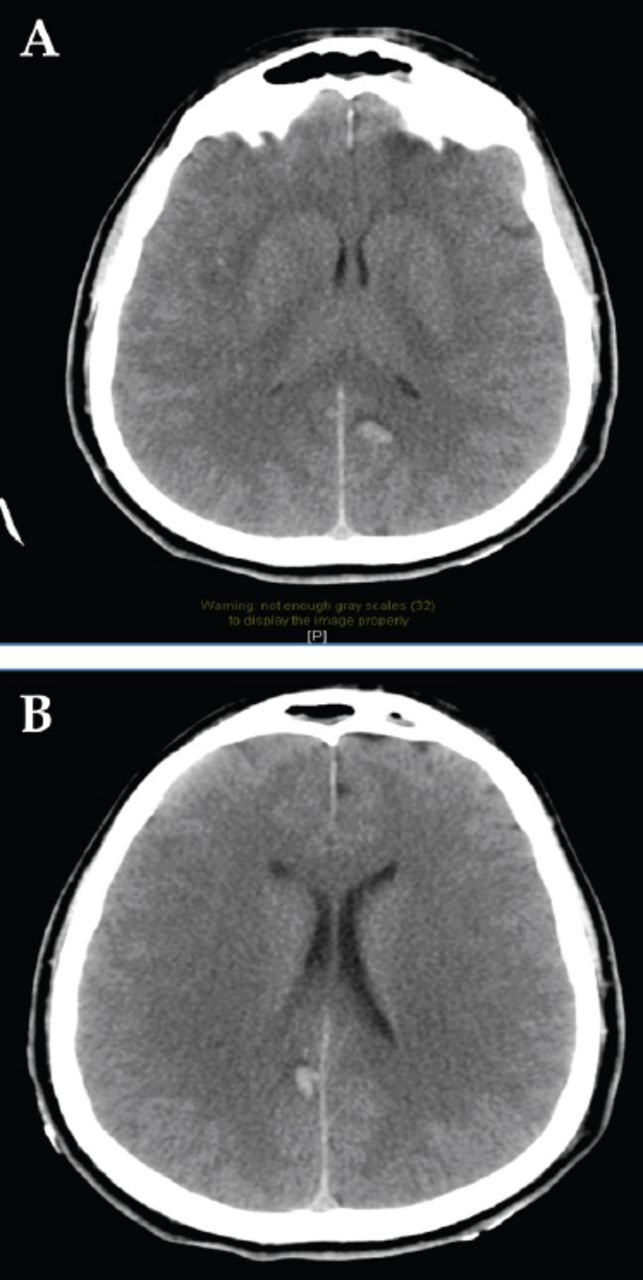
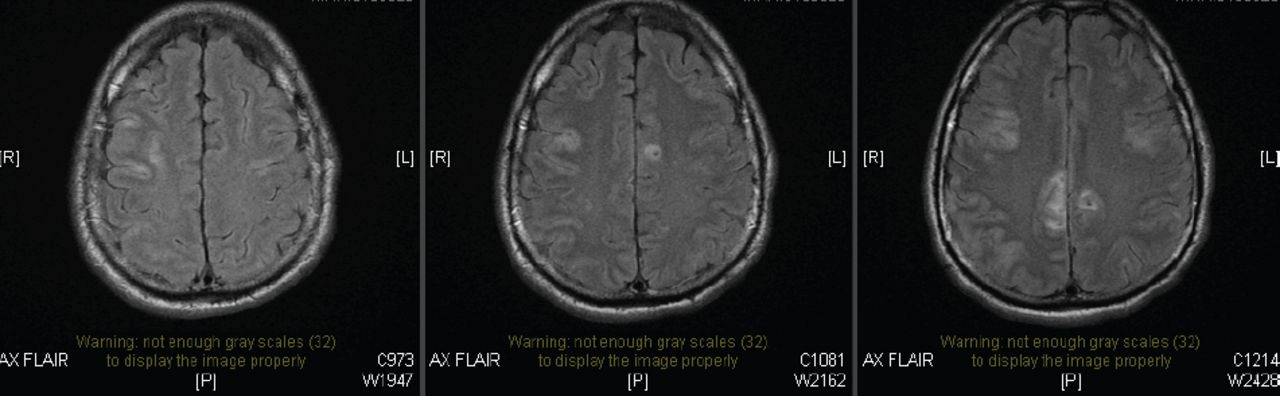
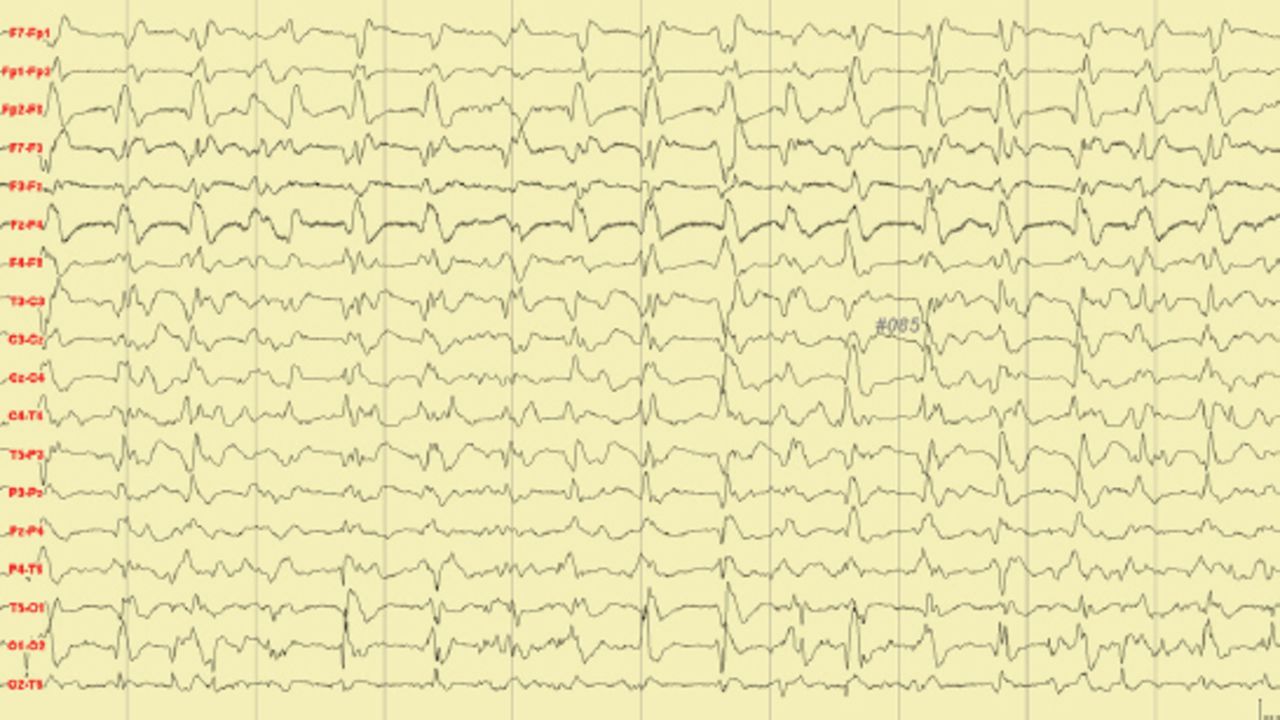
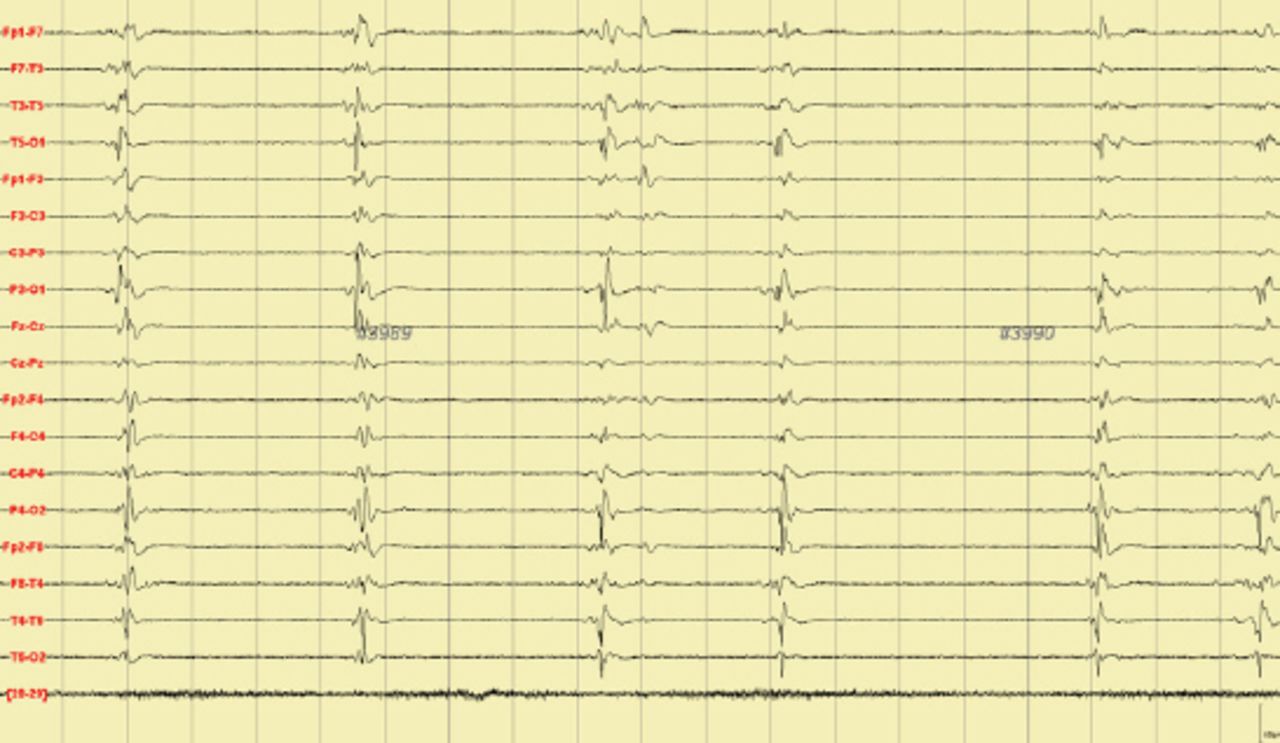
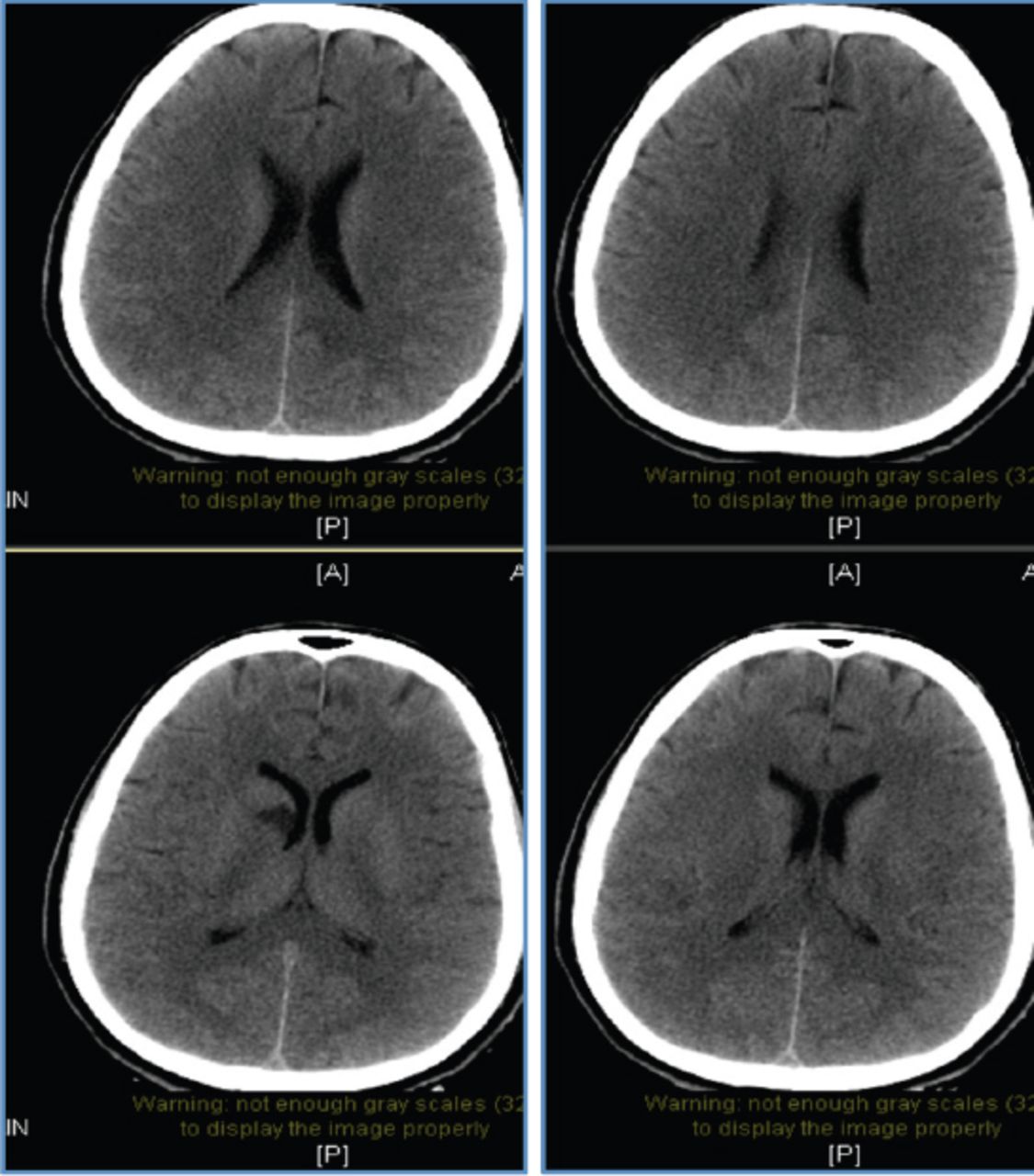
After 2 weeks, he was transferred to a tertiary center Emergency Department due to his deteriorated status. He was comatose and was having intermittent twitching of the face and upper extremity. He was transferred immediately to the intensive care unit and epilepsy service. Head CT, MRI and neck magnetic resonance angiography and venography (MRA/MRV), in addition to cerebral angiography showed no abnormality detected except for a parasagittal hematoma (Figure 1, 2) which improved after 2 weeks although the patients status remained the same. Although he was already on midazolam, propofol, and fentanyl, he had a prolonged seizure that lasted more than 10 minutes. He continued having in between seizures activities while he was being kept intubated and ventilated on tracheostomy with ketamine and thiopental. Continuous EEG showed initially generalized spikes and waves every 1-2 seconds (Figure 3) for >48 hours, and NORSE was diagnosed. Then, anesthesia induced burst suppression pattern was observed (Figure 4).
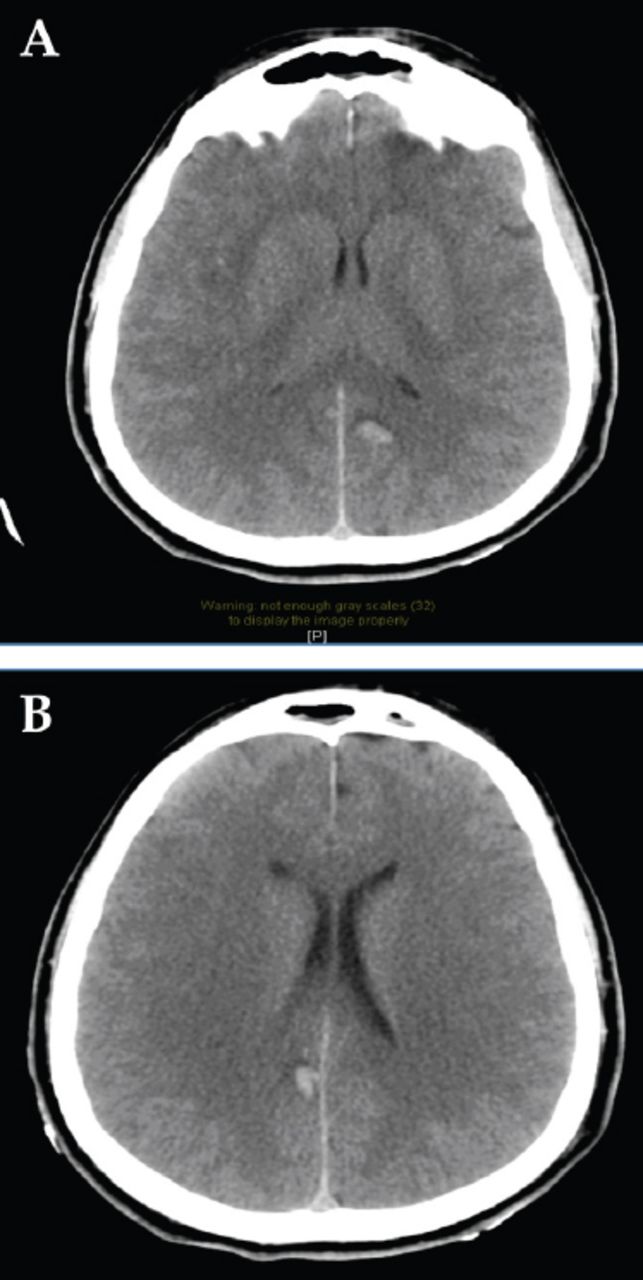
Axial CT brain showed left (A) and right (B) parasagittal hematoma without mass effect.
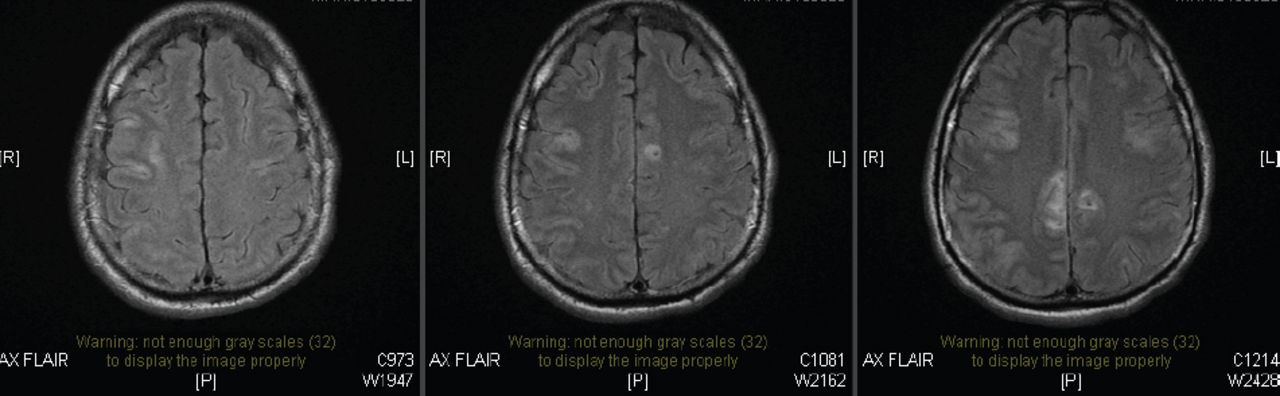
Axial FLAIR MRI with bilateral diffuse high signal intensities.

Electroencephalography showing generalized periodic discharges.

Electroencephalography showing suppression-burst pattern.
Work-up excluded Anti-NMDA receptor encephalitis and revealed elevated Antiphospholipid antibody (APA) including antiB2 Glycoprotein I. Lumbar puncture yielded clear cerebrospinal fluid, 6 white blood cells, with normal glucose and protein content. Bacterial, fungal cultures, cryptococcal antigen, cytology and whole-body pet scan in addition to para-neoplastic work-up all showed negative findings including voltage-gated potassium channel (VGKC), AMPA, GAD 65, LGI1. The APA levels remained elevated on 2 occasions.
Anti-β2 glycoprotein-I antibodies result was (50–100 U/mL) (IgG&IgA) and our normal laboratory value is <20U/mL. Antiphospholipid syndrome was diagnosed and heparin started. He continued to have episodic right arm and leg jerks with right facial twitching.
Multiple intravenous doses of benzodiazepine and a loading dose of phenytoin, valproic acid, levetiracetam, midazolam, thiopental, phenobarbitone, fentanyl, and ketamine infusion were administered. Moreover, a trial of 5 days induced hypothermia ended up with insufficient seizure suppression.
He was then put on a treatment plan which included pulse intravenous steroid, immunoglobulin, plasma exchange and rituximab which showed no immediate response. The doses were as follow :- IVIg 0.4g/kg for 5 days, steroid 1g for 5 days, and Rituximab 1g/once, 2 doses given within a 2 week interval. Over the following 8 months, levetiracetam 2g intravenously twice daily, lamotrigine 200mg nasogastric twice daily, and phenobarbital 110mg twice daily were administered and suppressed the seizures completely.
Follow-up and outcomes
A third head CT and MRI (Figure 5) after 8 months showed complete resolution of the hematoma. All anesthetic agents were then tapered off gradually while his seizures remained controlled, and he was eventually extubated. After approximately 8 months of ICU admission, he was discharged to the regular floor.
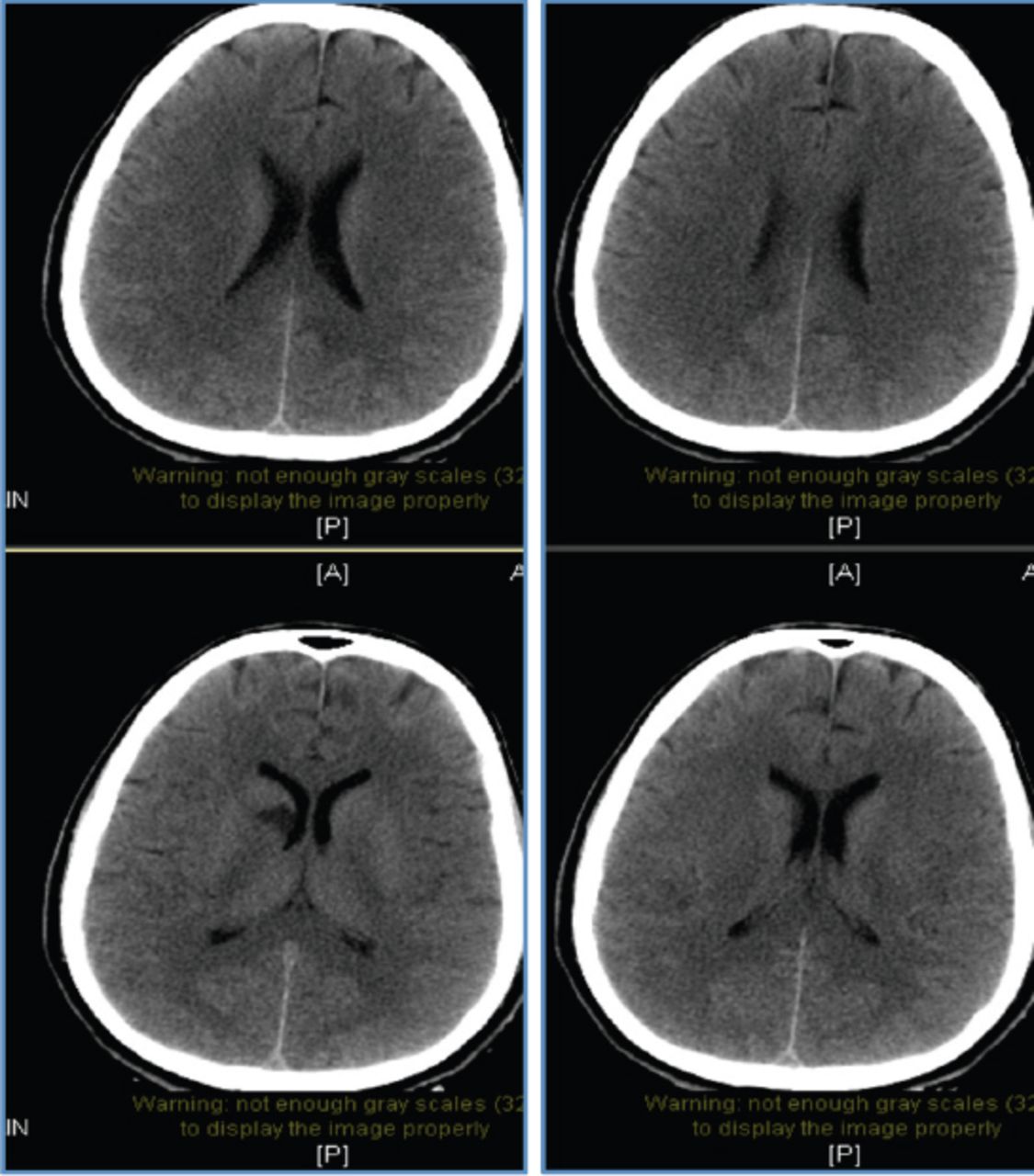
8 months later, a third CT brain showed complete resolution.
During the neuropsychologist’s evaluation, the patient was neat and mostly cooperative, although slightly aggressive. The patient showed neurocognitive decline, affected temporal orientation to day, date and year, slowed motor activity, labile mood, constricted affect, distracted attention and memory, and orientation impairment. Although his speech was impoverished, he had some insight of his illness, lack of words and difficulty in articulation. Although visual hallucinations were present, he did not have any suicidal or delusional thoughts. He was then being monitored in the same tertiary center for few months and then discharged with phenobarbital, tegretol, lamictal, and levetiracetam to a rehabilitation center with residual moderate to severe cognitive decline without any focal neurological deficits.
After 7 months of following up and being evaluated by the rheumatology and epilepsy service, he remained seizure free, and neurological examination showed nystagmus bilaterally and intact cranial nerves. However, psychiatric assessment’s remarkable findings were euphoric mood, cognitive impairment, poor planning, and macropsia with positive illusion picture.
During his routine outpatient follow up, a mental status assessment was conducted and it was reported that his appearance was disheveled, his speech was tangential, and his eye contact was intense with slowed motor activity and labile affect. He was easily distracted and had an irritable mood. In addition, his behavior was agitated with grandiose and paranoid delusions along with visual and auditory hallucinations. Furthermore, he was aggressive, homicidal, and had self-harm thoughts with short-term memory and orientation to place, object, and person. Schizophrenia psychosis was then diagnosed in the outpatient clinic after 9 visits over the course of a year. He started treatment with regular psychiatric follow-up at the local hospital in his town.
Relevant Past Medical History and Interventions of A 41-year-old, nonsmoker, married man who works in a college with no past relevant family or medical.
Medication summary table.
Discussion
Autoimmune disorders result in various neurological and psychiatric presentations. Antiphospholipid syndrome (APS), an acquired autoimmune disorder, can manifest a spectrum of clinical manifestations, including pregnancy morbidities; vasculopathies; and neuropsychiatric disorders such as stroke, seizures, and psychosis.4
The pathogenic mechanisms underlying APS are mostly complex or unclear. One mechanism of the pathogenesis of epilepsy secondary to APS could be linked to the immune-mediated response and vasculopathy inherent to APS. The vasculopathy is hypothesized to occur via the activation of endothelial cells, monocytes, and platelets, resulting in the overproduction of tissue factors and thromboxane A2.4 Autoimmune epilepsies are also known to be associated with refractory status epilepticus, the outcome of which is primarily determined by the underlying etiology of the seizures, age of the patient and duration of status epilepticus.5
An association between schizophrenia and autoimmune disorders such as APS has been previously documented. Although a coagulation pathway abnormality and immune-related phenomena have been suggested, the mechanisms underlying this association remains unclear,3,6 Since APS can manifest itself in the central nervous system as psychosis, we tend to believe that the schizophrenia could be a complication of the status epilepticus secondary to APS.7 However, we cannot dismiss the fact that schizophrenia could have been triggered by multiple factors, such as the use of antiepileptic medications that can cognitively impair epileptic patients.8
A recent study has shown that the pathophysiology of schizophrenia and epilepsy seems to involve a common pathway of dysfunctional glutamatergic neurotransmission.9 Moreover, there has been a proved positive genetic correlation between schizophrenia and epilepsy.10 Although an association with refractory status epilepticus is yet to be investigated, the incidence of mental health disorders such as schizophrenia is very common in epileptic individuals.10 According to our literature review, other than a case report of a schizophrenic patient developing status epilepticus, schizophrenia following status epilepticus has, to our knowledge, never previously been documented.
Our patient was in the intensive care unit (ICU) for 8 months with status epilepticus under continuous EEG monitoring. The patient underwent multiple trials of anti-epileptic medications and anesthesia to electrographically and clinically suppress seizures. These were successful, yielding a relatively good outcome. After ruling out symptoms of schizoaffective and mood disorders in addition to substance abuse and medical conditions, the patient met all the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) criteria for schizophrenia. These included visual hallucinations, delusions, disorganized speech, grossly disorganized behavior, continuous disturbance for more than 6 months, and social and occupational dysfunction.
In conclusion, we, therefore, advocate early referral of refractory status epilepticus patients to specialized centers in order to ensure better management. In addition, we recommend consistent psychiatric monitoring both inside and outside the ICU, particularly if an autoimmune disorder is suspected
Acknowledgment
We would like to thank Mrs. Lamees Al Khateeb for assisting in the writing of the manuscript. We would also like to thank Editage [http://www.editage.com] for editing and reviewing this manuscript for English language. Moreover, Dr. Riyadh Al Aqaili was the radiologist in charge of the case.
Footnotes
Disclosure. The authors declare no conflicting interests, support or funding from any drug company.
- Received November 25, 2018.
- Accepted April 15, 2019.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.