


Abstract
Objectives: To determine the prevalence of shunt malfunction without change in ventricle size in imaging modalities, and its clinical presentation.
Methods: A cross-sectional study conducted at King Abdulaziz Medical City, Riyadh, from June 2015 to May 2019. Patient’s demographics, clinical presentation and changes in ventricle size were collected. Statistical analysis was done using SPSS version 23.
Results: The study included 42 patients who underwent shunt revision. Imaging showed no change in size in 10 (24%) patients, mild enlargement in 8 (19%), and obvious enlargement in 24 (57%). The mean age of diagnosis was 22±16.7. 55% of the patients were males, 45% females. The cause of the malfunction was ventricular catheter occlusion in 14 (34%) patients, 10 (24%) patients had valve-related malfunction, and peritoneal catheter occlusion was present in 6 (14%) patients, and 12 (28%) patients had a combination of the previously mentioned causes. Analysis of the association between ventricular size and headache, vomiting, seizure, confusion, and loss of consciousness in patients with unchanged ventricular size and those with increased ventricular size has shown no statistical significance.
Conclusion: Shunt malfunction without ventricular size change was observed in 24% of all shunt malfunction patients. In addition, there was no relationship between ventricular size and patient symptoms.
Hydrocephalus is a serious condition in which cerebrospinal fluid (CSF) accumulates and causes the intracranial pressure to increase. The mean global prevalence of hydrocephalus is 85/100,000.1 The etiology behind hydrocephalus can be divided into 3 causes: an obstruction in the flow of the CSF, a defect in reabsorption of CSF, or overproduction of CSF. Increased intracranial pressure has different presentation based on age group. Neonates, for instance, will have bulging of the fontanelles, which can lead to disproportionate head growth if left untreated. In older children and adults, headache, vomiting and drowsiness are considered the typical symptoms. Obstructive hydrocephalus can be treated by inserting a ventriculoperitoneal shunt. This shunt bypasses the obstruction and drains the CSF into the peritoneum causing intracranial pressure to return to normal. Shunt failure can occur in 11-25% of cases. Failure can be due to obstruction or infection of the shunt. This failure is commonly called a shunt malfunction, and it is generally treated by doing a shunt revision.2,3
It is challenging to diagnose a shunt malfunction based on the clinical manifestation alone, which causes more reliance on imaging modalities. These diagnostic imaging modalities include CT scan and MRI. It is possible to confirm shunt failure if the ventricles appear dilated in imaging, a sign upon which physicians sometimes rely. This increased reliance can be disastrous in some cases because the imaging modalities occasionally reveal normal-sized ventricles while the shunt malfunction is present.4 According to a study conducted at Boston Children’s Hospital in 2014 in children who had surgery due to shunt malfunction, CT scan was positive in 65.7% and MRI was positive in 51.4% of patients.5 Another study conducted at Children’s Hospital in Birmingham found that 24% of the imaging results had described the ventricular system as “unchanged”, “stable”, “normal”, “unremarkable”, “small”, “smaller”, “slit”, “negative”, and “no hydrocephalus”.4 There is a lack of researches conducted in Saudi Arabia into imagining reliability in shunt malfunction, which had led to a misleading radiological reports in spite of presence of shunt malfunction. So, this study aimed to determine the prevalence of shunt malfunction without change in ventricle size in imaging. It also defined their characteristics, which included: the part of the shunt that was malfunctioning, and the clinical presentation. The study also investigated previous visits to the hospital with complaints of increased intracranial pressure with negative radiological findings.
Methods
The study was approved by the Institutional Review Board (IRB) of King Abdullah International Medical Research Center (KAIMRC). It was conducted in the neurosurgery department of the King Abdulaziz Medical City (KAMC), in Riyadh, Saudi Arabia. It was a cross-sectional study of 42 patients, covering the period from June 2015 to May 2019. Included patients were those who had shunt malfunction and underwent shunt revision. For diagnostic accuracy, the study excluded patients with brain tumors, shunt infections, supratentorial extra-axial fluid collections, holoprosencephaly, hydranencephaly, or those in which the distal terminus of the shunt was in a location other than the peritoneum. The collected data were patients’ demographics at time of shunt revision, presenting signs and symptoms, causes and site of shunt malfunction, and the severity change in ventricular size. The size of ventricles was determined by radiological imaging, which included computer tomography scan (CT-scan), magnetic resonance imaging (MRI), and ultrasound (US). Statistical analysis was carried out using SPSS version 23. Categorical data were presented as frequencies and percentages. Numerical data were presented as means and standard deviation. A chi-square test was used to analyze the associations. P-value less than or equal to 0.05 was considered statistically significant.
Results
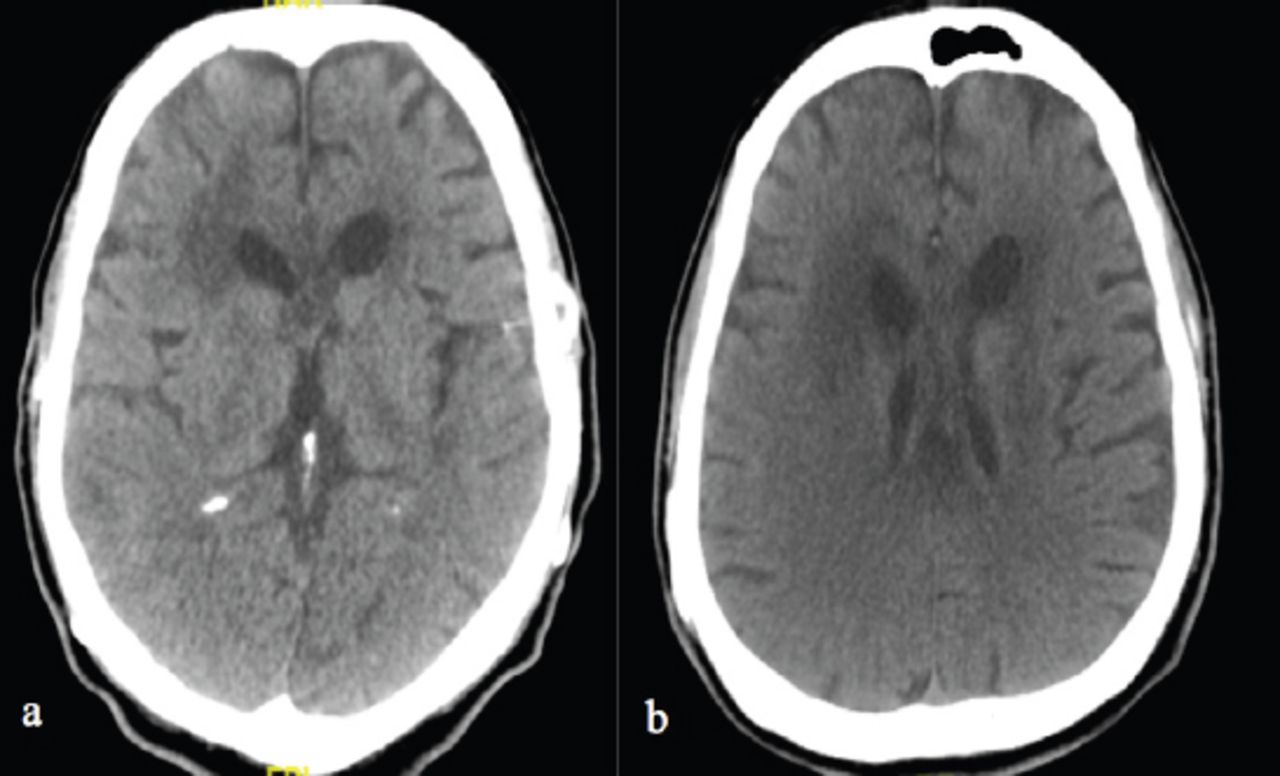
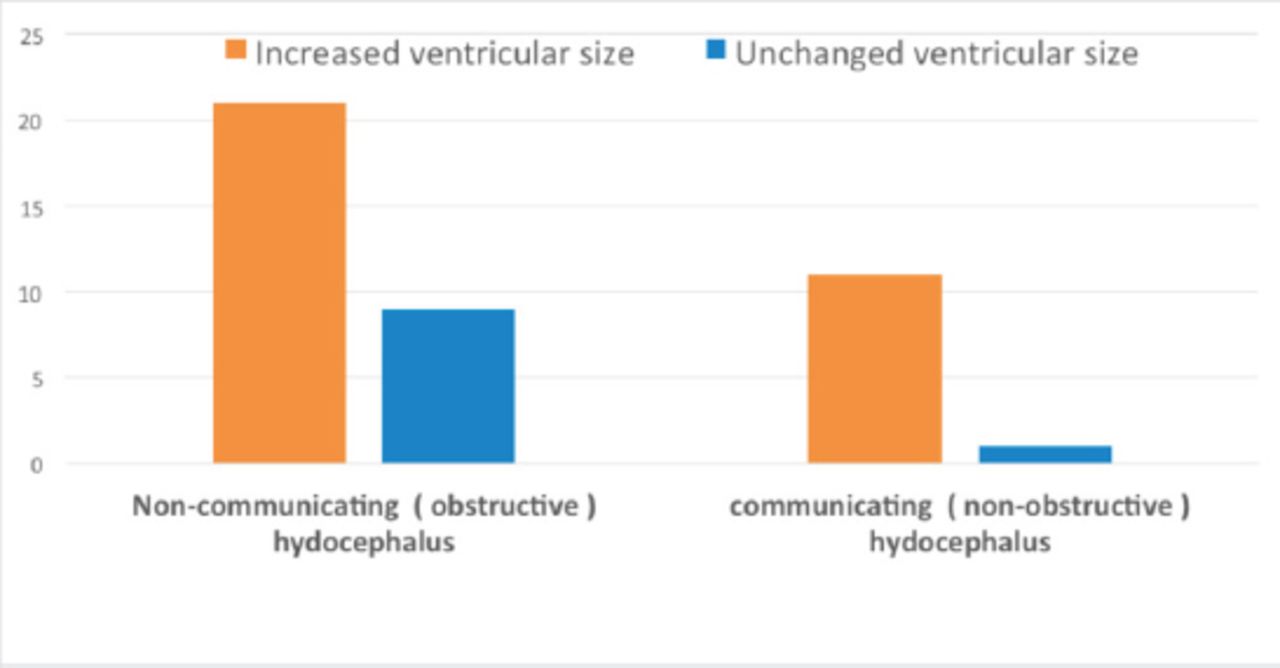
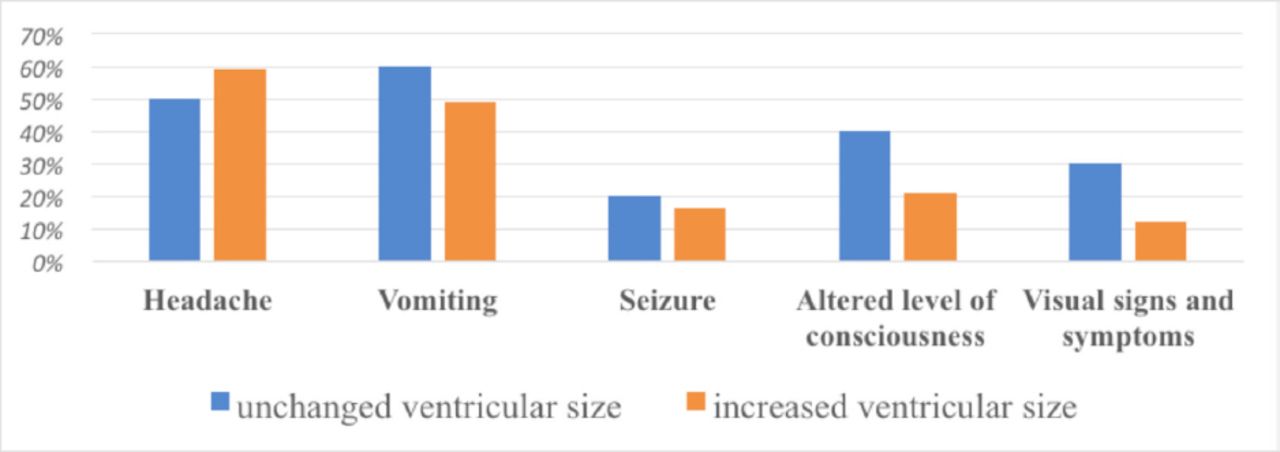
A total of 42 patients who underwent a shunt revision during the period from June 2015 to May 2019 were included in this study. The CT scans and MRIs showed no ventricular size change compared with the previous images in 10 (24%) of patients (Figure 1), mild enlargement in 8 (19%) patients, and obvious ventricular size enlargement in 24 (57%) patients. Table 1 shows characteristics of the study population. The mean age at diagnosis was 22±16.7 years. In terms of gender, 55% of the patients were male, 45% were female. Regarding causes, ventricular catheter occlusion was present in 14 (34%) patients, valve-related malfunction was present in 10 (24%) patients, and peritoneal catheter occlusion was present in 6 (14%) patients, and 12 (28%) cases had some combination of the previous causes. Figure 2 shows Types of hydrocephalus with both increased and unchanged ventricular size. Signs and symptoms in patients with shunt malfunction both with and without ventricular size change are shown in Figure 3. The analysis of the association between ventricular size and headache was statistically insignificant (p=0.4). Also, there was no statistically significant difference in vomiting, seizure, confusion, and loss of consciousness between patients with unchanged ventricular size and those with increased ventricular size (Table 2).
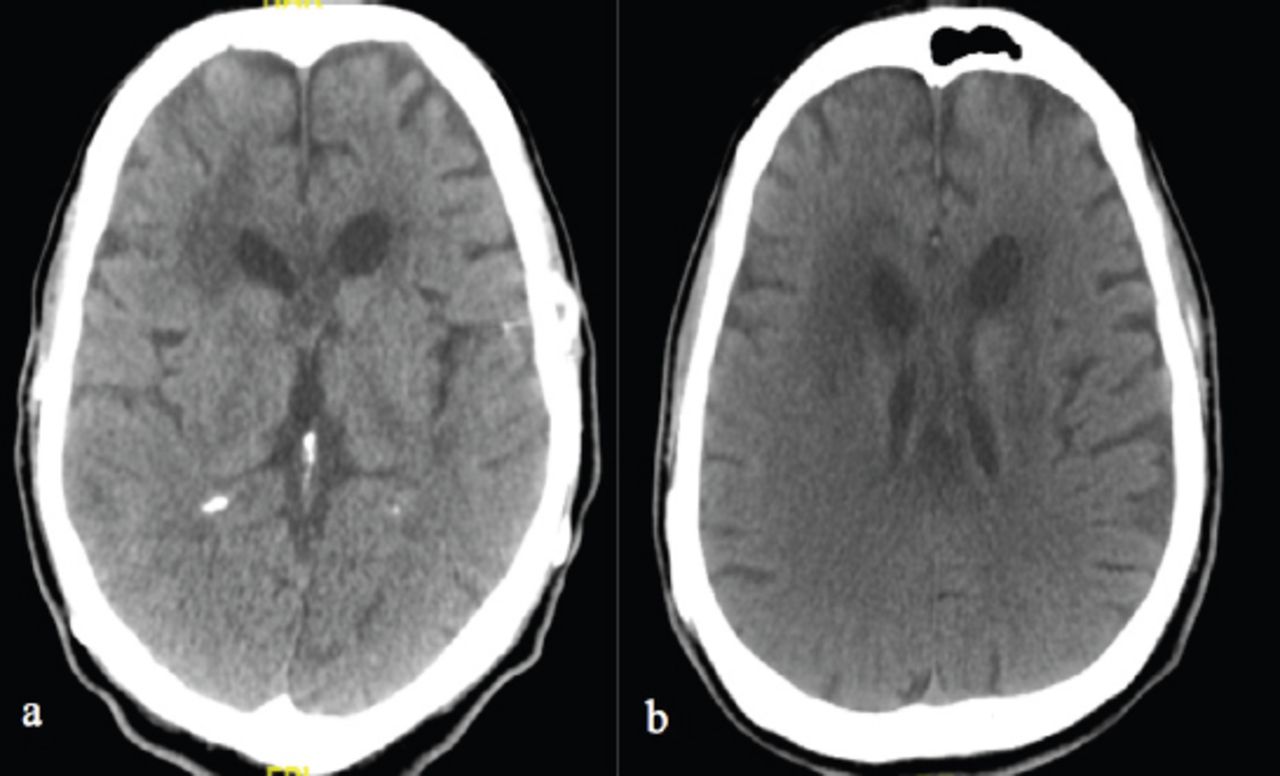
Non-contrast head CT scan in a patient with a) VP shunt malfunction showed unchanged ventricular size as compared to the previous head CT scan (b).
Characteristics of the study subjects.

Types of hydrocephalus with both increased and unchanged ventricular size.
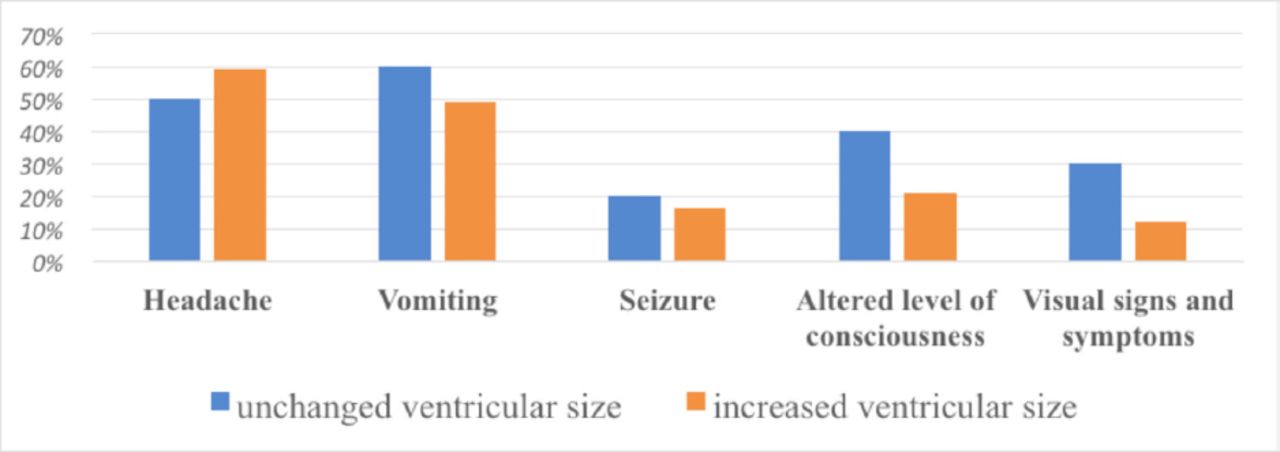
Signs and symptoms in patients with shunt malfunction both with and without ventricular size change.
The association between ventricular size and the most presenting symptoms.
Discussion
It is crucial to detect shunt malfunction cases because missed diagnoses may result in disastrous complications such as permanent neurologic injury or death.5 For diagnosis of shunt malfunction, CT scan and MRI both have similar sensitivity, specificity and accuracy rates.6-8 Occasionally, neurosurgeons observe shunt malfunction without ventricular dilatation on imaging studies. This study reported 24% of 42 patients presented with shunt malfunction without ventricular size changes. Other studies reported similar findings; Iskandar et al9 reported 11% of cases out of 68 patients having a shunt malfunction without ventricular size changes compared to the previous images with an age range from 1 month to 26 years. Amacher et al10 reported 4.3% of 23 patients with 0-17 age range. McNatt et al11 reported 9% of 177 patients. Sellin et al12 reported 10% of 42 patients. Mater et al13 reported 10.6% of 386 patients. Miller et al14 reported 27.4% of 155 patients who had no CT changes and needed shunt revisions. For only pediatric age group patients, Sean et al. reported 9% of 177 patients with median age of 7.2 years.15
All of the mentioned reports suggest that imaging studies are not totally reliable for definitive diagnosis of shunt malfunction because some patients may have a normal or small ventricular size despite the presence of shunt malfunction. Invasive monitoring of intracranial pressure in these groups of patients is also insufficient to make a definitive diagnosis.10-11 This study suggests that the safest approach to take upon suspicion of shunt malfunction and for deciding whether surgical intervention is necessary is primarily evaluating patients’ clinical signs and symptoms.
Even with ventricular dilation on CT scan, definitive diagnosis of shunt failure cannot be made as ventricular shunt pseudo failure (chronic constipation) can be the actual cause of dilatation thus shunt revision may not be needed and only releasing of bowel content is enough to normalize ventricular dilatation.16
One of the risk factors associated with low compliance ventricles is childhood ventriculitis. Small-sized ventricles in shunt malfunction could be due to one or more causes, including: poor compliance, intermittent shunt malfunction, slit ventricle syndrome, CSF leak (through skin incisions, sub glial collections, or the formation or enlargement of a syringohydromyelia), and the possibility that the ventricles were smaller in the past and that what is now observable is in fact large for that particular patient.
In order not to miss an enlarged ventricle that appears normal and to accurately perceive changes, the imaging studies taken when patients present with symptoms of shunt malfunction should be compared with previous imaging studies in which the patient was normal.17
A radiology report might be misleading for diagnosing shunt malfunction; therefore, radiologists should be aware and notify neurosurgeons of that fact. Evaluation of shunts by non-specialists who tend to rely on the radiologist’s report like emergency physicians, family physicians or pediatricians puts patients at greater risk of misdiagnosing malfunction and of developing fatal complications by sending them home without appropriate management.4,9 It is possible to carry out alternatives for malfunction detection other than CT-scan and MRI. These are a shunt tap, shunt patency, intracranial pressure monitoring, long in-hospital observation, and surgical exploration. However, this study suggests that the final determination of shunt functionality should be through surgical exploration.
Ventricles with low compliance have limited ventricular dilation capability. Some authors stated that patients in this situation are at greater risk to encounter acute neurological deterioration with shunt malfunction.14,18 However, our results showed no significant association. Single-centered experience and low sample size are limitations of this study. We recommend further multi-center studies on larger groups of patients.
In conclusion, out of 42 cases, we observed 24% of shunt malfunctions without ventricular dilatation on CT or MR scans. Therefore, detection of shunt malfunction by imaging studies is unreliable. Neurosurgeons should consider this phenomenon when encountering symptomatic patients and for their decision of surgical intervention when scans’ images reveal no change in ventricular size.
Ethical Consent
All manuscripts reporting the results of experimental investigations involving human subjects should include a statement confirming that informed consent was obtained from each subject or subject‘s guardian, after receiving approval of the experimental protocol by a local human ethics committee, or institutional review board. When reporting experiments on animals, authors should indicate whether the institutional and national guide for the care and use of laboratory animals was followed.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received June 12, 2020.
- Accepted August 18, 2020.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.