


Abstract
Objectives: To assess the etiology of status epilepticus (SE) among the pediatric patients of a tertiary center in Jeddah, Kingdom of Saudi Arabia (KSA).
Methods: Data from 88 cases was obtained retrospectively from 2006 to 2017 from King Abdulaziz University Hospital (KAUH). Patients aged between 28 days and 14 years with the symptoms of SE were selected for this study.
Results: The data show that the proportions of SE etiologies were 30.5% for febrile seizure, 11.9% for electrolytes imbalance, 8.5% for hydrocephalus, 6.8% for CNS infections, and 6.8% for neoplasm. The other etiologies of SE were trauma, fever, intractable epilepsy, cerebrovascular accident, hemorrhagic stroke, etc. There were no clear etiologies in 8 cases. Most of the patients were not of Saudi origin (64.3%), boys (67.8%), and had generalized epilepsy types (91.8%), and 58.6% of the patients complied with epilepsy medications.
Conclusion: The most prevalent etiology of convulsive status epilepticus was a febrile seizure, followed by electrolyte imbalance and hydrocephalus. However, a nationwide study in KSA must be conducted to determine the major etiologies of SE for its effective management and prevention. Educating families and patients regarding antiepileptic drugs is necessary.
Status epilepticus (SE) is a life-threatening seizure and common pediatric crisis. It is the most critical case of seizure. For every 100,000 children, 73 had SE. The younger the child, the higher the incidence of SE will be. The incidence of SE in children aged less than 2 is high at 156 per 100,000 and is at the highest for infants.1-3 The SE is the commonest pediatric neurological emergency and a major cause of admission to the pediatric intensive care unit (PICU). Historically, many attempts have been made to define and explain seizure and SE. The International League Against Epilepsy (ILAE) recently defined SE as generalized convulsive SE for any tonic-clonic seizures that continue more than 5 minutes, as focal SE for any focal seizure that continues more than 10 minutes.4 Clinicians describe it in a very operational and timed manner, stating that early action can prevent neuronal injuries from happening. They define SE as a continuous attack that exceeds 5 minutes or 2 or more separate attacks with incomplete recovery of consciousness between attacks.5 The SE is of 2 types: the convulsive type (CSE), which is the commonest, and the non-convulsive type (NCSE), which accounts for only 6% of the cases.6
The main risk factors for SE are listed in many studies, with acute febrile illness being listed as a major cause. One study conducted in Japan found that prolonged febrile seizure is the cause of SE for 81.6% of the cases, while the causes for 18.4% of the cases were epilepsy, encephalopathy/encephalitis, and meningitis.7 Another study was carried out at Ayub Medical College with 125 patients, where most of the cases were caused due to acute febrile illnesses.8 In a cohort study conducted by the Specialized Children Hospital’s Pediatric Emergency Department at Cairo University, the acute symptomatic (AS) causes were the main etiologies. In that study, most AS cases (61%) were caused due to central nervous system (CNS) infection; the other causes were metabolic, hemorrhagic stroke, and neoplasim; most of them were infants aged less than one year at the SE onset (67%) and suffered from refractory seizure (86%) in which the seizure lasts for more than 60 minutes.9 Another main cause of SE was epilepsy; as mentioned in previous study in 1994, most SE patients have a history of epilepsy. Febrile seizures, meningitis, encephalitis, and metabolic disease were the other etiologies of SE in the study.10 However, only few studies include pediatric cases from Riyadh city of Saudi Arabia11 and a guideline management,12 and only a few and old (2002 and less) studies on SE pediatric patients in Jeddah,13,14 and thus making our study a significant contribution in this field. The study objectives are to identify the most common SE risk factors to prevent them in the future.
Methods
This is a retrospective cross-sectional study performed at King Abdulaziz University Hospital (KAUH), a tertiary teaching health center in Jeddah, Saudi Arabia. Data was gathered from medical records dated from 2006 to 2017. We were only able to collect data for 108 suspected cases of SE and epilepsia partialis continua (EPC), and the number of patients was low, as this hospital only serves the university’s staff members and their families, except for some complicated and referred cases from other hospitals. We carried out data collection at KAUH from 1 March 2006 to 10 July 2017 to assess the SE determinants. In this study, we excluded the neonatal age group and epileptic patients without SE and EPC or absence seizure. We define SE as 5 minutes seizure duration. We included all patients who were 28 days to 14 years old. Furthermore, 7 cases were excluded from the study, as they were clearly not cases of SE or there was not enough evidence to back up the diagnosis. The study variables consisted of demographic data, admission to either Emergency Room (ER) or PICU, seizure type, epilepsy character, cause of admission (e.g., prolonged febrile seizure, CNS infection, electrolyte imbalance (hypocalciemia, hypoglycemia, hyponatrimiea and hypokalemia), hemorrhagic stroke, neoplasm, trauma, and hydrocephalus), compliance with medication, medical history of epilepsy, metabolic disorder, cerebral palsy, or neoplasm, and the frequency of epileptic attack. We did not obtain any information about the use of EEG in seizure monitoring and diagnosis. This study was approved by the Unit of Biomedical Ethics of KAUH in Jeddah, Kingdom of Saudi Arabia (KSA).
The participant’s demographic data is presented in a descriptive statistic. Mean and standard deviations (SD) were used to report the continuous variables. Categorical variables were presented as frequencies and proportions. Pearson’s chi-square test was used to compare the epilepsy distribution with gender and nationality. The P-value was set as <0.05 for statistical significance. Statistical Package for Social Science (SPSS), Version 23 (IBM, Armonk, NY, USA) was used for all the analyses in the study.
Results
Of the collected cases, 88 patients (81.5%) fulfilled the study criteria. Of the total, 51 (58%) were males, and the mean age was 4.5 (SD±3.7).
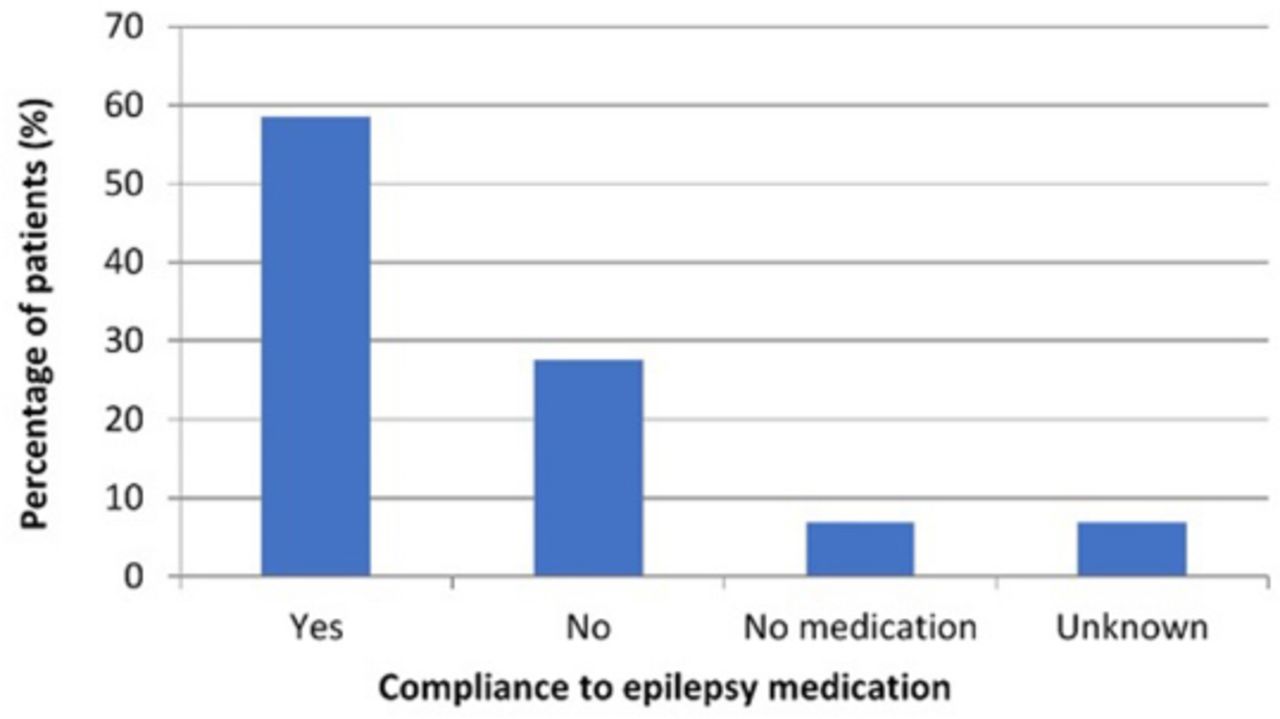
Table 1 shows that the predominant type of seizures among the cases was generalized epilepsy 56 (91.8%), and the main cause was prolonged febrile seizure (30.5%), followed by electrolyte imbalance (11.9%). Figure 1 presents the percentages of the different causes of epilepsy. Table 1 reveals that most of the participants complied with epilepsy medications (58.6%), as shown in Figure 2.
Characteristics of the participants, n (%).
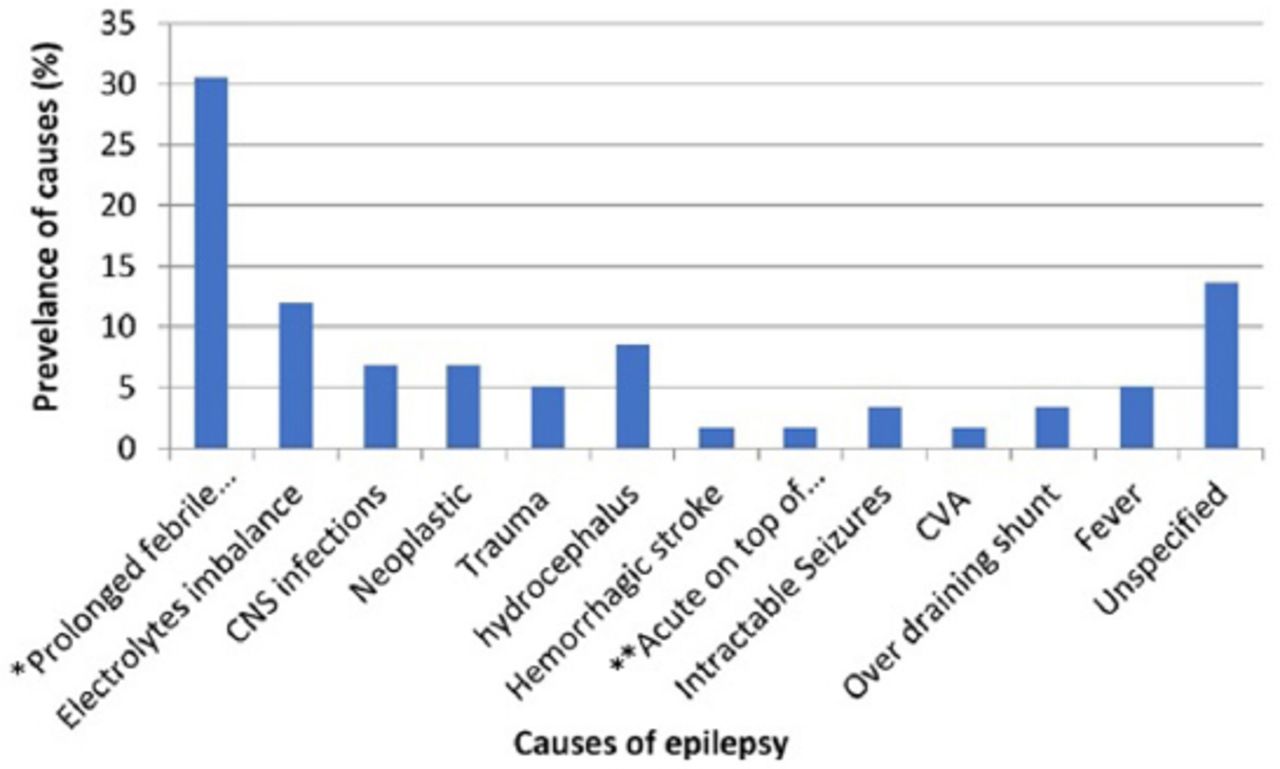
Causes of epilepsy (%). *Prolonged febrile seizure, **Acute on top of remote symptomatic
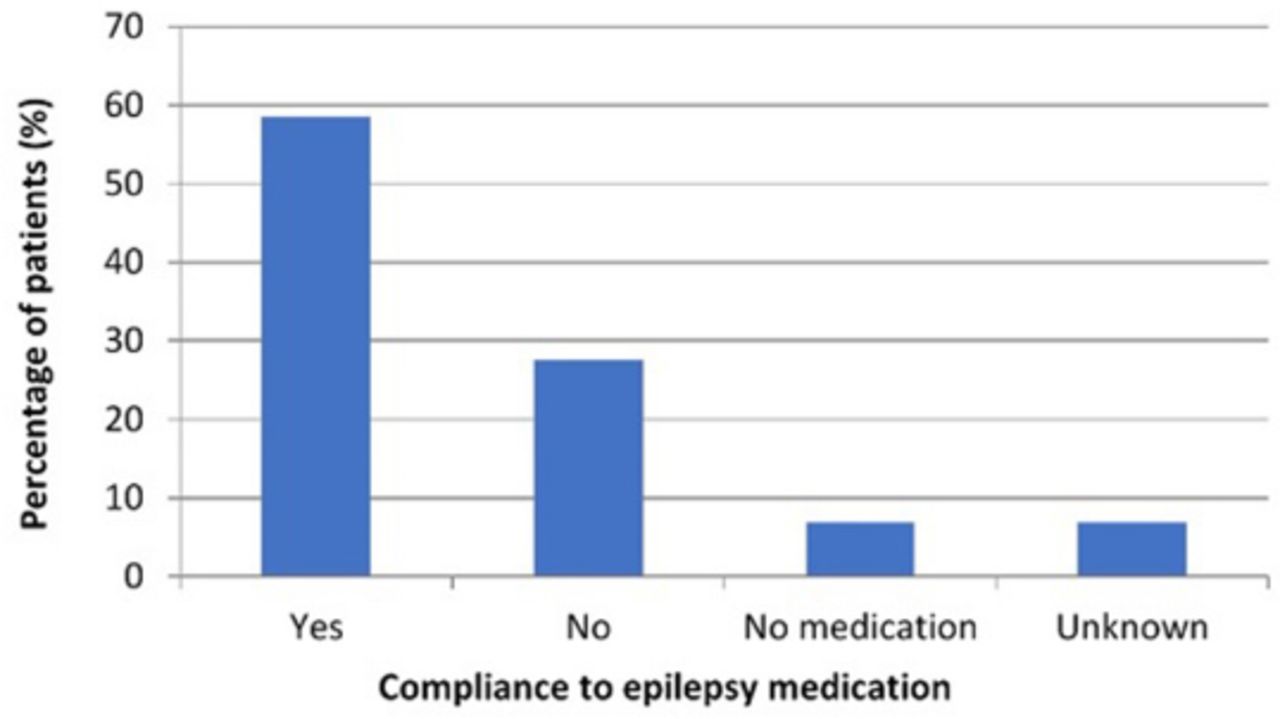
Compliance to epilepsy medications and medication state among the patients (%)
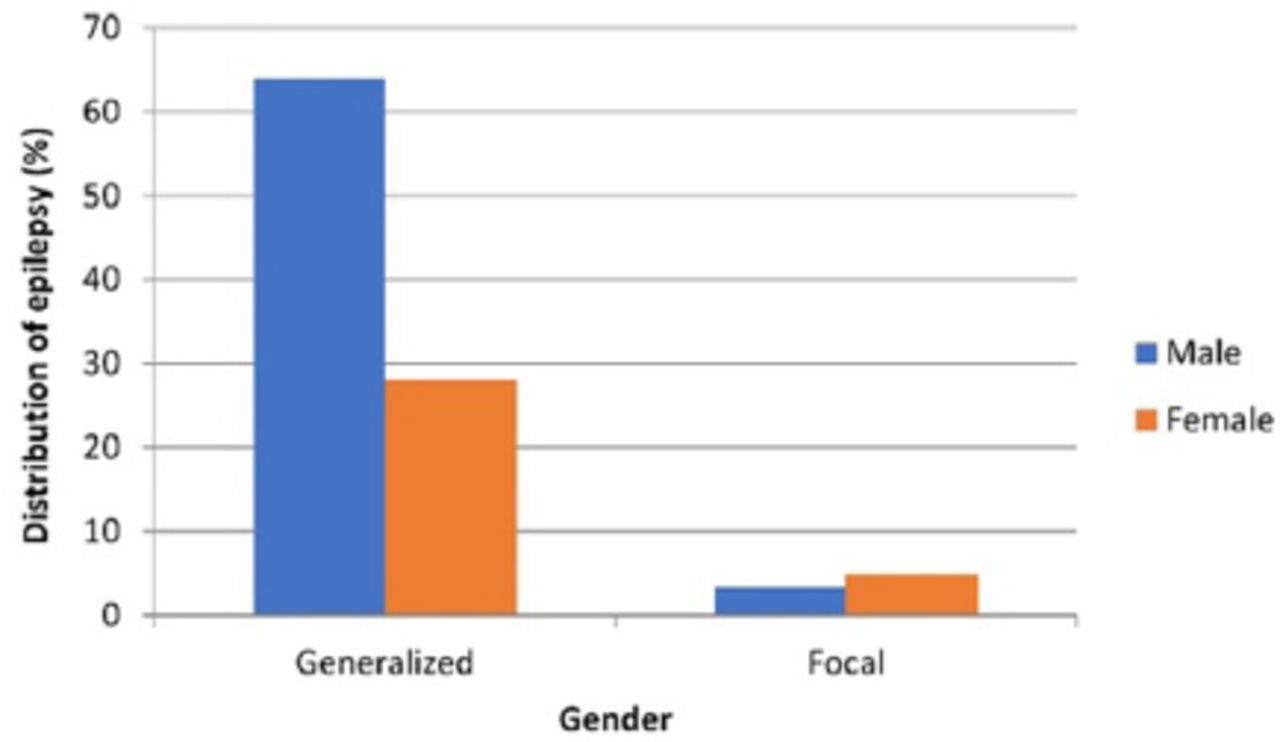
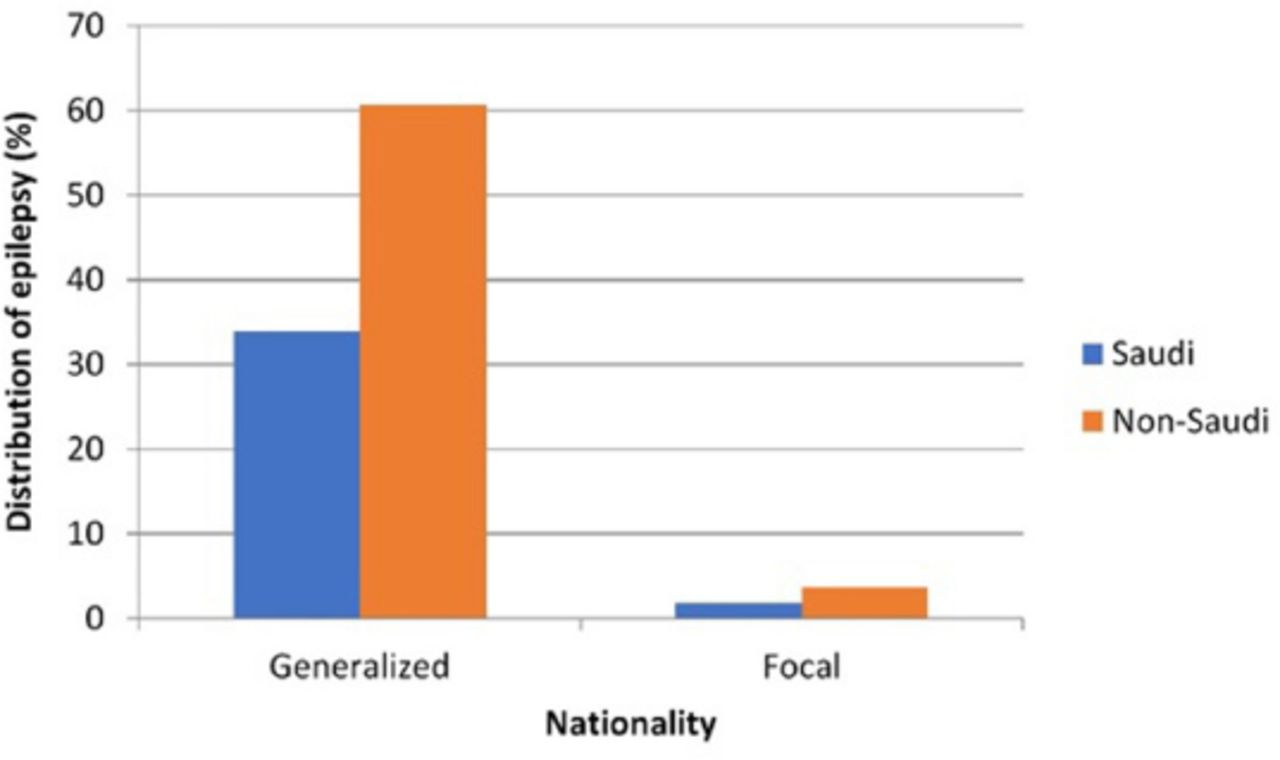
Table 2 demonstrates a higher proportion of epilepsy among males (67.2%) compared to females (32.8%) and among non-Saudi participants (64.3%) compared to Saudi participants (35.7%), as shown in Figure 3 and Figure 4.
Distribution of epilepsy by gender and nationality .
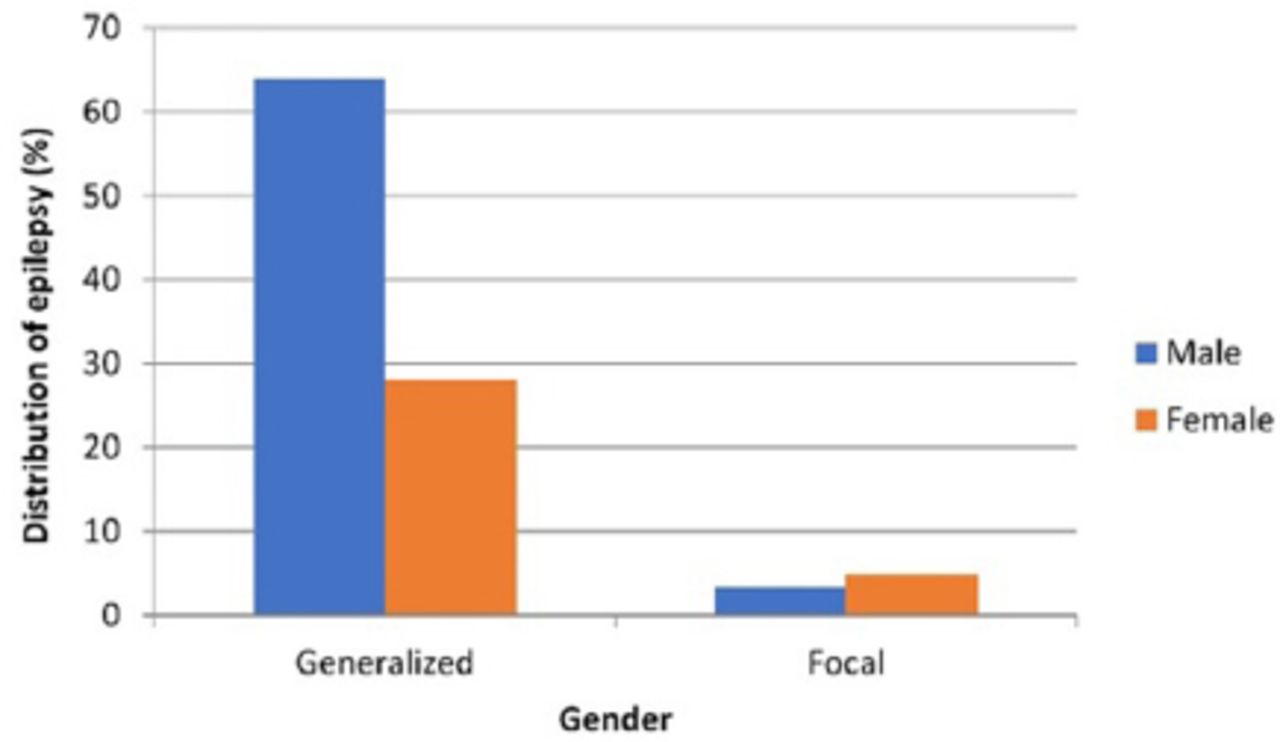
Distribution of epilepsy type by gender (%).
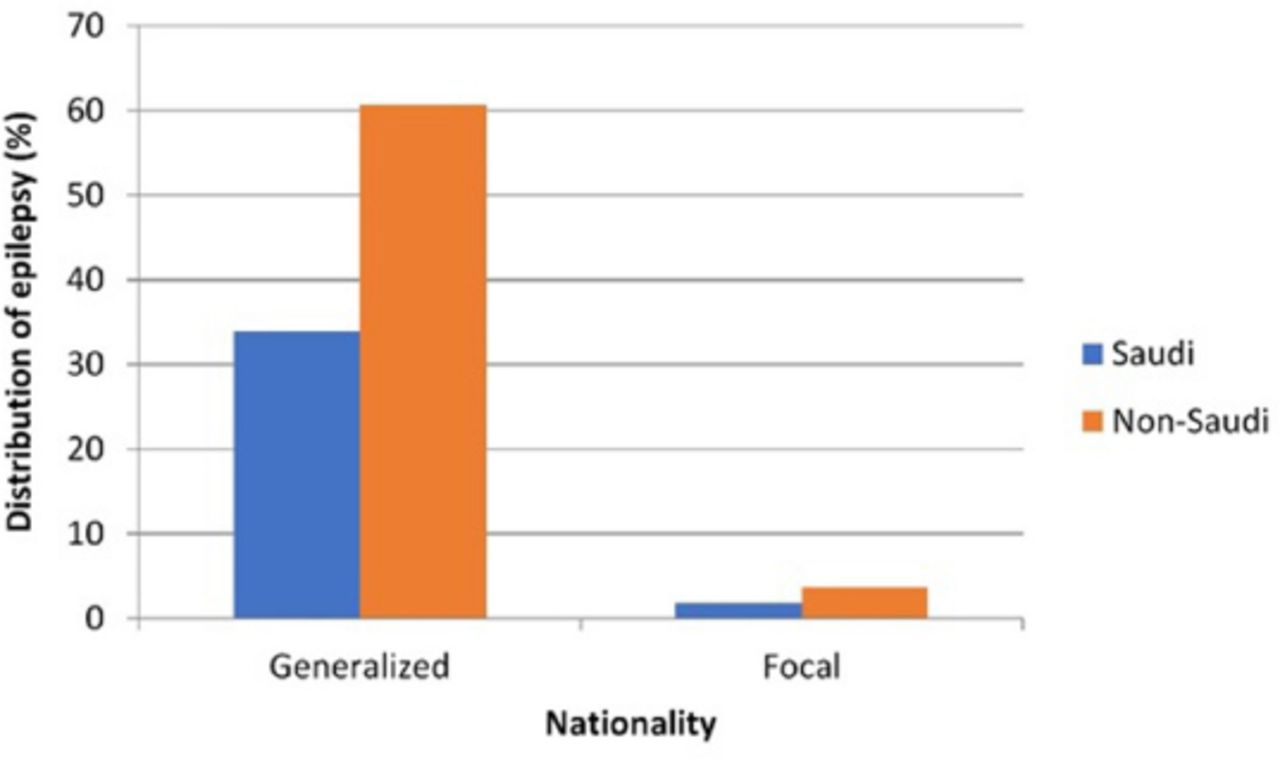
Distribution of epilepsy type by nationality (%)
Discussion
The SE among children is life-threatening, and it needs immediate medical attention.1 Therefore, epidemiological studies are required to estimate their prevalence and etiologies, thereby helping in its management. The morbidity rate of SE among infants and children is much higher than that among adults; however, the mortality rate is higher in adults compared to the former.2 The prevalence of SE varies from 10 to 73 per 100,000 people, and the majority of the reported cases are reported among children of less than 2 years.3 Considering this fact, we included children in the age group of 28 days to 14 years. In our study, etiological factors such as prolonged febrile seizure, electrolyte imbalance, central nervous system infections, neoplastic, hydrocephalus, and other factors are attributed to SE among children. The effect of etiological factors in the development of SE varies according to demographic history and population structure. The CNS insult, fever, and infection,15 poisoning (ingestion), positive blood cultures, low anticonvulsant levels, abnormalities in neuroradiology, electrolytes, and metabolism (inborn error)16,17 have been reported as the major causes of SE among children. Although febrile seizures were found to be the commonest cause of status epilepticus in our study (30% of cases), in another study conducted at King Abdulaziz Medical City (KAMC) in Riyadh city of Saudi Arabia, febrile causes found to constitute 15% of total cases presenting with pediatric status epilepticus. This difference is attributed to the fact that referral centers usually have a low number of febrile SE as KAMC.11 In a Japanese study, children below the age of 15 (49.3%) were found to be affected by SE due to febrile seizure;7 on the other hand, other European research studies have shown that the occurrence of SE can be attributed to cerebrovascular pathology (34–60%).18,19 In another study, 17% of the total included SE cases were caused either due to metabolic disorder or CNS infection.20 In developing countries such as Brazil, South and Central America, Kenya, Ethiopia, and countries in Africa, infections were reported as the major causative factor for SE.20-24 However, our results show that prolonged febrile seizure, electrolyte imbalance, hydrocephalus, CNS infection, neoplasim, and trauma are the major causes of SE. Nevertheless, it was not possible to point out the exact cause of 13.6% of the SE cases. Prolonged febrile seizures were responsible for 25% of the SE cases in cities of the USA. Interestingly, children with normal brain function were more affected by SE. However, in some older children who had an earlier incidence of seizures, SE caused only a few complexities related to the brain.25
Compliance with medicine could be observed in 58.6% of the SE patients; however, 6.9% were not taking any medicine. Non-compliance to medication were the main cause of SE in a study conducted in Colombia.1 In Saudi Arabia, non-compliance is common,26 and another Saudi study among adolescents revealed that 38% are non-compliance to medicine.27 No Saudi studies regarding compliance were conducted among children. The SE among male children were more prevalent than female at KAUH. Although SE was found to be more prevalent in male patients than female patients, this difference is not significant at early stages; however, with advancing age, a significant difference was observed between male and female patients.28,29 This result differs from the previous Saudi study in KAMC, which showed no difference between males and females.11
Further, SE incidence was more prominent among children of non-Saudi origin than those of Saudi origin. Ethnic origin as a causative factor of epilepsy was also found in an American study, which demonstrated that the non-Hispanic black population’s mortality rate was higher than that of the Hispanic population.30 The mortality rate of children with SE varied from 0% to 3% and was less compared to adults. However, it adversely affects the development of the nervous system of children.31 As a proper etiological study is essential to identify the major factors responsible for the development of SE in a particular demographic population, detection at the incumbent stage will help better manage pediatric SE, as in most cases, the first seizure triggers the progression of SE.
This study’s main limitation is the study’s retrospective nature and the relatively small sample size, as this is a retrospective hospital-based cross-sectional study. Thus further evaluation for the outcomes could not be established. Despite these limitations, we think it provides useful insight into SE’s etiologies and gender and ethnic differences. Further prospective designed studies are suggested.
In conclusion, this study is the first of its kind to be conducted at KAUH, Jeddah, KSA in order to determine the etiological factors of SE. This report will be helpful to clinicians for the management of SE, particularly among non-Saudi children. However, further studies need to be conducted in Jeddah and nearby regions to acquire a comprehensive understanding of the factors associated with SE.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received July 15, 2020.
- Accepted September 14, 2020.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.




{kind=link}
{kind=link}
{kind=link}
{kind=link}