


Abstract
Meningiomas are benign, slow-growing tumors originating from arachnoid gap cells. They constitute 15%-20% of all intracranial tumors in adults and 04%-4% in the pediatric age group. Meningiomas in the posterior fossa in the pediatric period do not initially come to mind. In the case presented here, there was a cystic meningioma showing heterogenous contrast and obstructive hydrocephaly was observed associated with 4th ventricle pressure. the tumor was totally removed, then the ventriculo peritoneal shunt was applied.
Meningiomas are benign, slow-growing tumors originating from arachnoid gap cells. They constitute 15%-20% of all intracranial tumors in adults and 0.4%-4% in the pediatric age group.1 In both adult and pediatric cases, they are often seen in a convexity and parasagittal area where there is dense arachnoid granulation tissue and arachnoidal villi, and posterior fossa localization are uncommon in both patient groups.2 They are seen secondary to neurofibromatosis 2 in 20%-40% of cases.1-4 Clinical findings show differences according to tumor size and localization. Findings may develop associated with hydrocephaly in posterior fossa tumors. The case is here presented of a meningioma with posterior fossa localization, which is rarely seen in the pediatric age group.
Case Report
Patient information and clinical finding
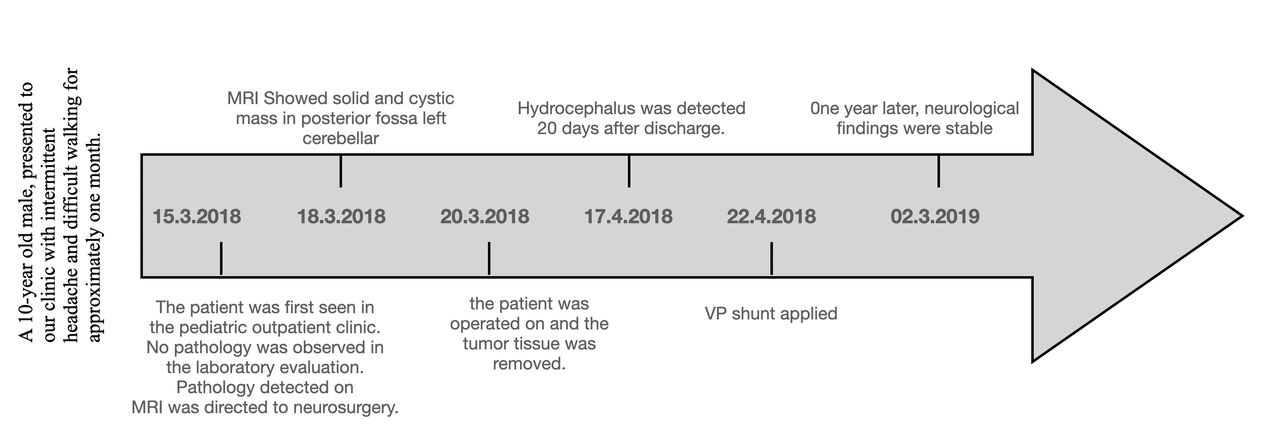
A 10-year old male presented at the Emergency Department with the complaints of intermittent headache and difficulty walking which had been ongoing for approximately 1 month. As deficiencies were determined in electrolyte levels before the radiological examination, the patient was admitted to the Pediatric Clinic for follow up (Figure 1).
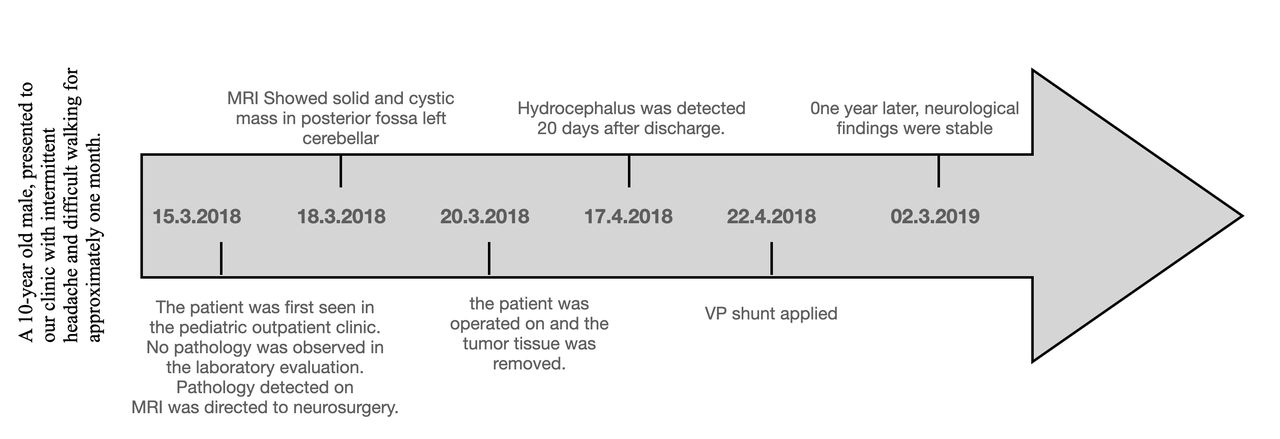
- Timeline picture of the clinical course of the patient.
Diagnostic assessment
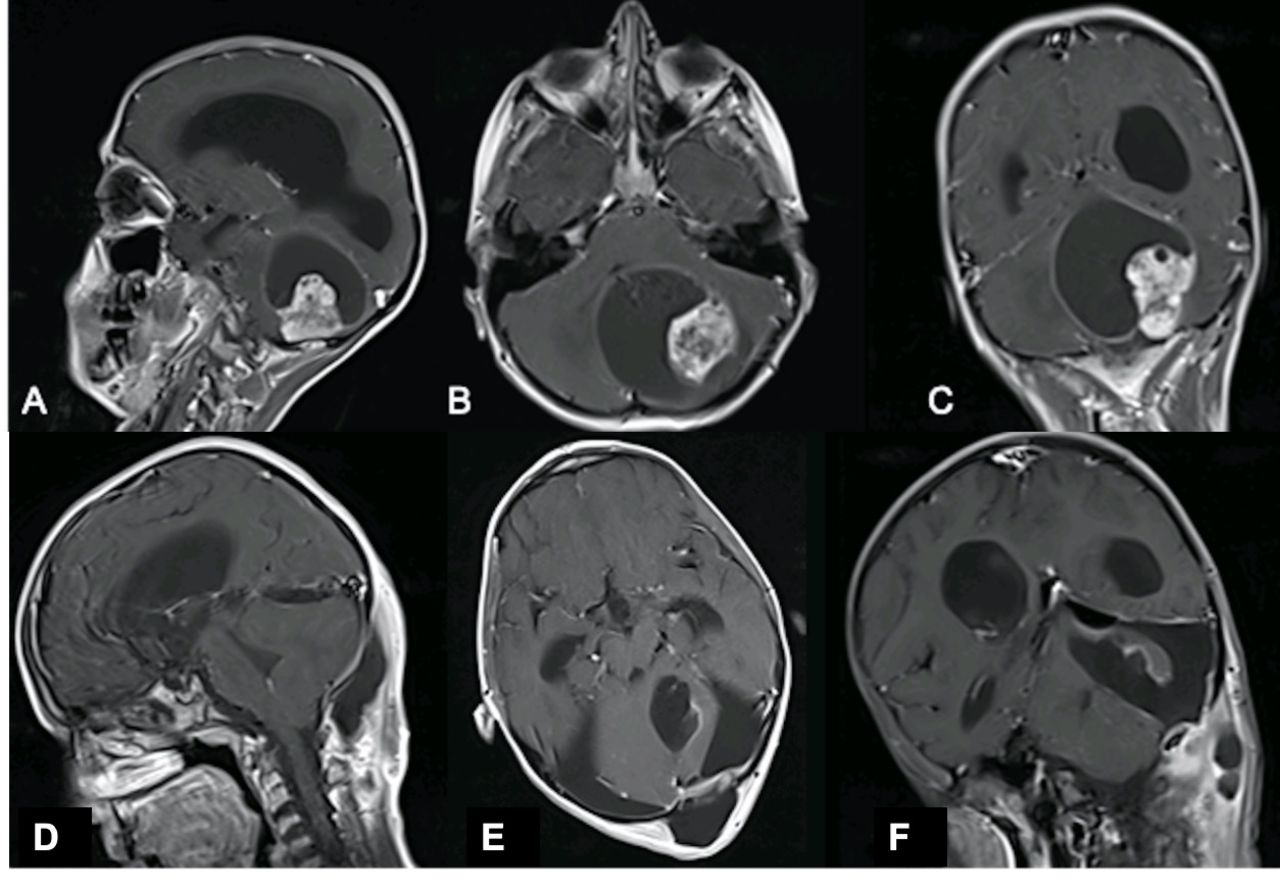
Symptoms continued despite the electrolyte levels brought back to normal limits, so cranial contrast magnetic resonance imaging was taken (Figure 2 ABC). In the left cerebellar hemisphere, a mass of approximately 60x55 mm was observed containing a solid cystic mass, 30x22mm in size with heterogenous contrast on the post-contrast series, and pressure was observed on the 4th ventricle and brain stem. The Evans index was measured as 0.43. It was decided to admit the patient for surgery.

- Preoperative magnetic resonance imaging with enhancement godolinium scan showing posterior fossa meningioma A) T1weight Sagital, B) T1weight axial, C) T1weight coronal images. Postoperative magnetic resonance imaging with enhancement godolinium scan showing complete resection of the tumor, D) T1weight Sagital, E) T1weight axial, F) T1weight coronal images
Therapeutic intervention
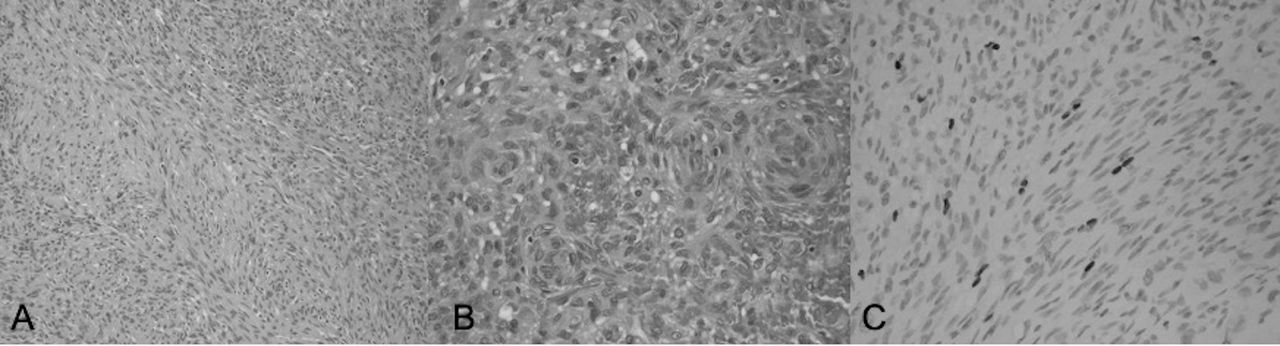
With the patient in the prone position, the head was fixed with a Mayfield headpiece then an occipitocervical mid-line skin incision was made and left paracentral craniotomy was applied. Cystic dark yellow colored tumor tissue, which had invaded the dura, was totally removed together with the invaded dura. The dura defect was closed by applying duraplasty. In this surgery, the 4th ventricle was seen to have provided the aqueductus sylvii and cerebrospinal fluid flow dynamics. Therefore, in the first stage, shunt surgery was not applied (Figure 2DEF). The histopathological examination was reported as consistent with a fibroblastic type grade 1 meningioma (Figure 3).

- Hystopathological examination of the tumor A) Tumor cells predominantly spindle (H&E, x200), B) Vortex structures in the focal area (H&E, x400), C) Ki67 proliferation index (İHK, x400)
Follow-up and outcome
As no residual mass was observed on the postoperative magnetic resonance imaging, the decision of the oncology council recommended follow up with no requirement for additional treatment. At 20 days after discharge the patient presented again with symptoms of hydrocephaly. The radiological findings supported hydrocephaly so a temporary ventricular catheter was applied. As the cerebro-spinal fluid samples taken were sterile, a ventriculo-peritoneal shunt was placed. After 3 days, the neurological findings were stable and the patient was discharged.
Discussion
Meningiomas are benign tumors originating from arachnoid cap cells, which may be seen particularly in adults and the advanced age group. They are rarely seen neoplasms in the pediatric age group, and show various clinical and biological differences from meningiomas in the adult population. The incidence in children varies between 0.4% and 4%.4-7 In the vast majority of cases, there is supratentorial localization and some develop secondary to neurofibromatosis.
They are generally seen at the end of the first decade of life or the beginning of the second decade. In series by Ravindranath, Menon and Pinto, the mean age at which meningiomas are seen has been reported to be 14.1 years, 15.5 years and 14.3 years, respectively.3,4,8 Although pediatric meningioma cases are very uncommon, meningiomas with posterior fossa localization are even more rare.2-4,8 In pediatric cases with posterior fossa localization, tumors such as medulloblastoma, pilocytic astrocytoma, ependymoma, and hemangioblastoma are the pathologies which first come to mind. Meningiomas in the posterior fossa in the pediatric period do not initially come to mind. In some intracranial meningioma cases, there are accompanying neurofibromatosis 2 syndromes. Menon et al reported concomitant neurofibromatosis 2 in 26% of cases in a series.3 In the current case, it is noteworthy that there was posterior fossa localization and it was not seen together with neurofibromatosis.2 In adult meningiomas, there is female gender predominance, whereas in pediatric cases, the incidence is higher in males. The current case was aged 10 years and male.
Clinical findings such as headache, vomiting, ataxia, epileptic seizures and visual impairments vary according to the size and localization of the lesion. In supratentorial pediatric meningiomas, epileptic seizures and visual problems are common symptoms.3,4,8 In posterior fossa meningiomas, there is an increased risk of hydrocephaly associated with aqueduct stenosis and 4th ventricle pressure. For patients presenting with findings of acute hydrocephaly, an external ventricle catheter is placed in the first step, then it is more appropriate to apply a ventriculo-peritoneal shunt when necessary after tumor surgery.1
There are no typical imaging findings suggestive of meningioma in children. On computed tomography, calcification and lesions of different densities may be seen. In pediatric meningiomas, hyperostosis and calcification on CT are seen especially in tumors associated with neurofibromatosis 2.9 Cystic changes may be seen in 2%-20% of pediatric meningiomas. Perilesional edema is determined in 40%-50% of cases.4,8 Calcification is seen at a lower frequency than in adult menigiomas.5,7
Contrast involvement is seen in almost all meningiomas. Although homogenous contrast involvement is more frequent, there may be irregular contrast in a third of cases. On magnetic resonance imaging, hypointensity is seen most often on T1-weighted slices, and hyperintensity is most often determined on T2-weighted slices. Contrast involvement is determined in the vast majority of cases.3,4,8
In the case presented here, there was a cystic meningioma showing heterogenous contrast and obstructive hydrocephaly was observed associated with 4th ventricle pressure. In histopathological examination, it has been reported in literature that grade 1 meningothelial, transitional, psammomatous, and fibroblastic meningiomas are most often seen. The total rate of atypical and malignant meningiomas is below 5%. The current case was evaluated as grade 1 fibroblastic as a result of the histopathological examination.
Different treatment modalities such as surgical excision, radiotherapy and embolization are used in intracranial meningiomas. Total excision is the gold standard to obtain long-term remission of intracranial meningiomas.2,9 However, in pediatric cases, total excision may not always be possible, especially in large meningiomas, and multiple lesions because of massive blood loss and hypothermia.9 Radiotherapy is generally applied in residual lesions, recurrent meningiomas or malignant type meningiomas.9 Adjuvant radiotherapy together with tumor excision in children is only considered in malignant meningioma cases.10 However, radiotherapy is a treatment option which is avoided in cases aged <3 years because of the possibilities of severe morbidity.1 There are insufficient studies related to the benefits of preoperative embolisation.9
Complications may be seen associated with surgical treatment such as cerebro-spinal fluid fistula, seizure, loss of strength, cranial nerve involvement and infection. In meningiomas with foramen magnum and posterior fossa localization, mortality may develop as a result of respiratory failure associated with subcranial nerve damage.3,4,8,10
In conclusion, meningiomas are rarely seen tumors in childhood, and of these, meningiomas with posterior fossa localization are even more rare. Clinical and radiological findings and gender distribution are different from those of adults. Surgical excision is the gold standard treatment for these tumors, and in cases with accompanying hydrocephaly, there may be a need for ventriculo-peritoneal shunt. Radiotherapy can be considered for recurrent and residual malignant meningiomas in patient over the age of 3 years.
Case Reports
Case reports will only be considered for unusual topics that add something new to the literature. All Case Reports should include at least one figure. Written informed consent for publication must accompany any photograph in which the subject can be identified. Figures should be submitted with a 300 dpi resolution when submitting electronically. The abstract should be unstructured, and the introductory section should always include the objective and reason why the author is presenting this particular case. References should be up to date, preferably not exceeding 15.
Acknowledgment
We would like to sincerely thank Dr. Khalid Omar Alahmadi, for his review of the radiology images. We would also like to thank Falcon Scientific Editing [https://falconediting.com] for editing and reviewing this manuscript for English language.
Footnotes
Disclosure. The authors declare no conflicting interests, support or funding from any drug company.
- Received December 14, 2020.
- Accepted October 12, 2020.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.