


Abstract
Objectives: To evaluate the cognitive status with a simple practical test, clock drawing test (CDT), in a larger multiple sclerosis (MS) patient group and in comparison, with controls.
Methods: We included 171 patients (17–65 years) with MS and clinically isolated syndrome (CIS) and 98 healthy controls who applied between date 2018-2020 years in Neurology Department of Pamukkale University. The CDTs were applied to all subjects. In addition, the cognitive functions of the patient group were evaluated with the neuropsychological test battery.
Results: The CDT scores were significantly lower in relapsing-remitting MS (RRMS) group than the control group (p<0.005). Progressive MS patients’ CDT scores were significantly lower than RRMS and CIS (p<0.0001). According to our results, the CDT showed progressive deterioration in MS better than another practical and free tests. Additionally, the CDT scores were statistically better in patients whose disease began with sensory symptoms than whose disease started with motor and brainstem symptoms (p<0.0001).
Conclusion: The CDT cognitive impairment prediction performance is 60%, CDT is a useful, easy-to-administer, practical test that can be used in cognitive assessment in MS and CIS.
In multiple sclerosis (MS), cognitive impairment can be seen in the early period independently of neurological deficits. This situation causes many challenges, including morbidity, problems with work, and social dysfunction. The cognitive destruction in the early period occurs due to axonal loss secondary to inflammation and the neurodegenerative process in white and grey matter effected in the temporal and frontal cortex.1,2 Hence, both white and grey matter are responsible for cognitive impairments. In MS, particularly learning, memory, conceptual reasoning, speed of information processing, attention, and executive functions are affected, but language functions like fluency, repetition, and expression are generally preserved.3 Multiple factors like age, disease duration, disease course, affective disturbance, and disability can change cognitive status without clear correlation. Some studies have shown that with the increase of disease duration, cognitive deterioration can be seen. However, in several studies the cognitive process-time relationship has not been demonstrated.4 Therefore, even if the duration of the disease is short and the neurological deficit is minimal, a neuropsychological evaluation should be performed in the early stage. However, it is very important to be able to do this with a short, reliable, practical, and cost-effective test. The MMSE desktop test, which is very commonly used, is not sensitive enough. Although neuropsychological tests are very sensitive and specific, they are not practical because they take a long time and are not cost-effective. The clock drawing test (CDT) is a useful test in terms of abstract thinking, integrative functions, and visuo-spatial construction.5 Barak et al6 reported the sensitivity of the CDT as 93.4% and the specificity as 85.8% in early cognitive evaluation in MS. The CDT is an effective and practical method, since it evaluates the wide spectrum of cognitive functions and is not affected by the language, ethnicity, and educational background of individuals.7 We already know that the CDT was used to evaluate cognition in people with MS in small groups8 and without controls.6 However, in our study, we aimed to evaluate the effect of the CDT on cognition in comparison with neuropsychological tests in larger patients and healthy control groups and at the onset of symptoms of the disease.
Methods
Study design
We included 171 patients, aged between 17–65 years between 2018-2020, with definite MS and clinical isolated syndrome and 98 healthy controls age and gender matched at the Neurology Department of Pamukkale, University Medical Faculty in our study. All patients (n=171) were prospectively examined, their demographical information recorded, and the expanded disability status scale (EDSS) calculated. The exclusion criteria were, (1) relapse for the previous 30 days, (2) Persistent optic neuritis (3) having other chronic systemic and neurological diseases, (4) chronic drug or alcohol abuse, and (5) EDSS >8.
Standard protocol approvals, registrations, and patient consents
Informed written consent forms were obtained from all the enrolled participants in our study with the guidelines recommended by Medical Ethics Committee of Pamukkale University.
Clock drawing test
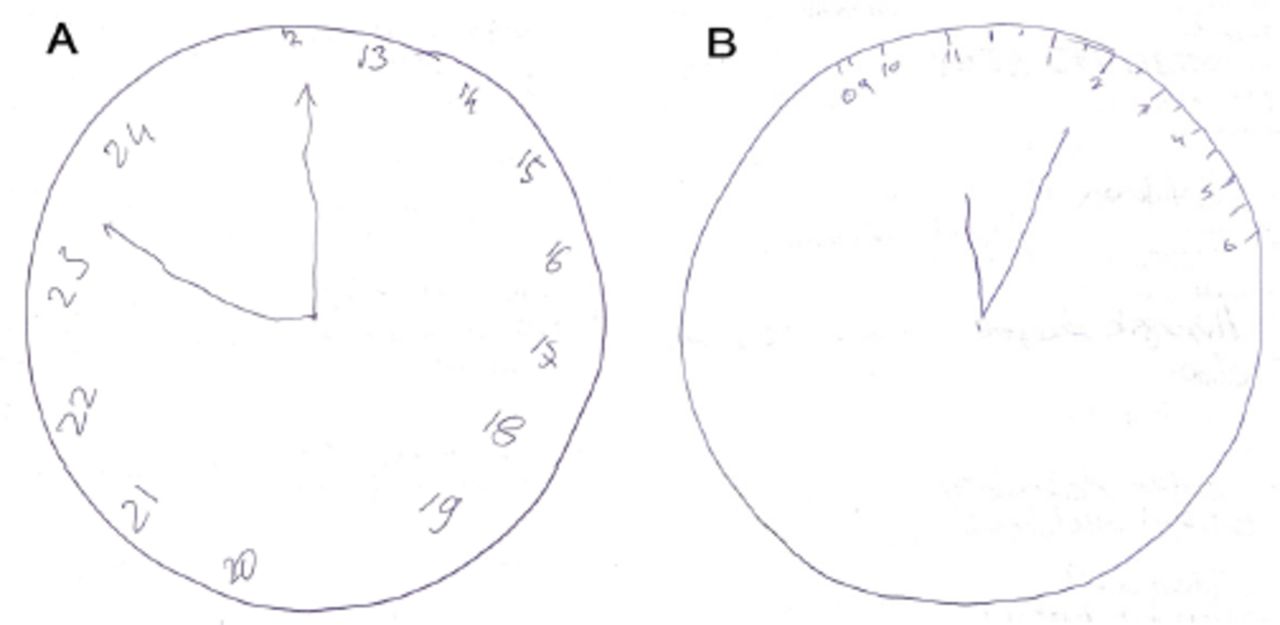
Both patients (n=171) and controls (n=98) were given a blank sheet of paper, asked to draw circle, and place numbers as on a clock, and set the time at ten after eleven. The CDT was evaluated by an experienced neurologist according to 4-point and 10-point scoring methods.9,10 Some examples of the patients’ CDTs are shown in Figure 1 A & B.
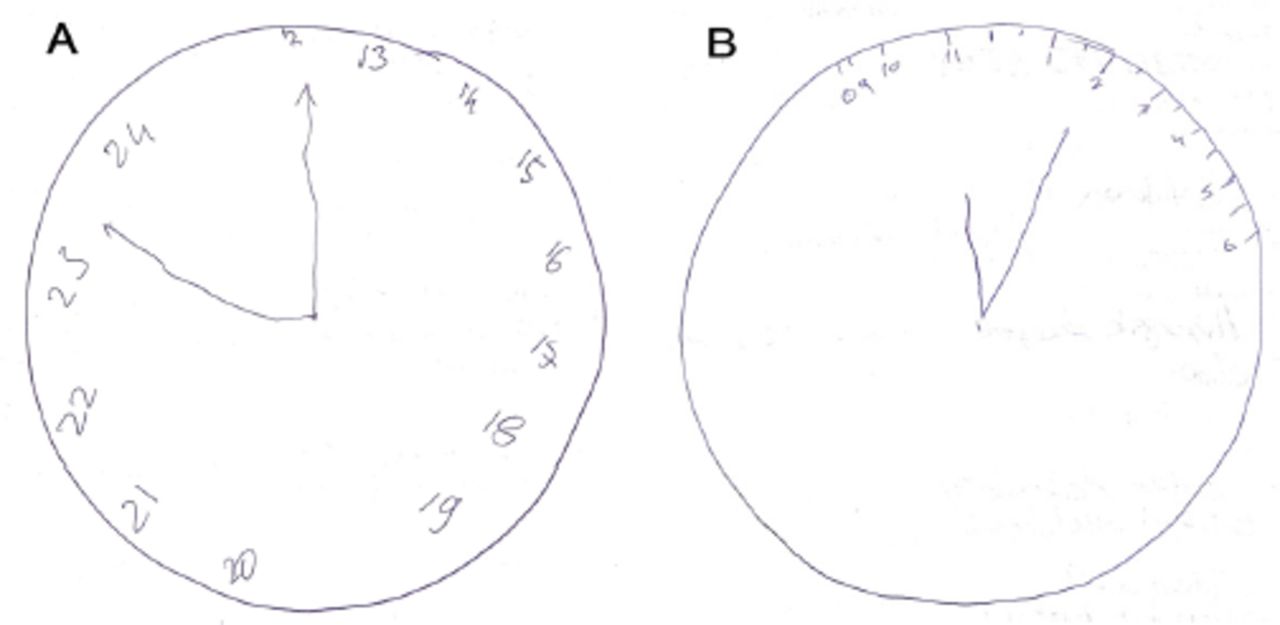
- The samples of clock drawing tests of patients, A) A 46-year-old female who was diagnosed secondary progressive multiple sclerosis. B) A 53-year-old male who was diagnosed primer progressive multiple sclerosis
Neuropsychological assessment
The cognition evaluation in the patients was performed in detail by an experienced psychologist with the neuropsychological test (NPT) battery, which have reliability and validity studies for Turkish patients. The battery contains a variety of cognitive domains: for verbal learning and memory the ‘California verbal learning and memory test’ and ‘Verbal fluency test’; for non-verbal learning and memory the ‘Weschler visual memory scale’; for executive functions and selective attention the ‘Stroop color naming test’; and working and immediate memory were assessed with the written ‘Symbol Digit Modalities Test (SDMT).’ The MMSE was also evaluated and compared with other neuropsychological tests and the CDT.
The presence of depression was shown using the Beck Depression Inventory. Nineteen patients with severe depression who had scores over 30 were excluded from the study. Finally, 152 patients were subjected to statistical analysis.
Statistical analysis
All statistical analyses were performed using SPSS 25.0 (IBM SPSS Statistics 25 software (Armonk, NY: IBM Corp.)). The continuous variables were defined by the mean±standard deviation and median (minimum maximum values) and categorical variables were defined by number and percent. The Kolmogorov-Smirnov test was used for the determination of normal distribution.
For independent group comparisons, we used the independent samples t-test when parametric test assumptions were provided, and the Mann-Whitney U test and the Kruskal-Wallis variance analysis (post hoc: Mann-Whitney U test with Bonferroni correction) were used when parametric test assumptions were not provided. Spearman’s correlation analysis was performed to investigate the relationships between the continuous variables. The difference between categorical variables was analyzed with the Chi Square analysis. Statistical significance was determined as p<0.05.
Results
One hundred and seventy-one patients who were diagnosed with definite MS and CIS were evaluated, but we excluded 19 patients who had major depression. Finally, 152 patients were involved in the study along with 98 controls that did not have any neurological or psychiatric diseases. There were no significant differences in age, gender, and education levels between the patients and controls. The patients’ mean age was 39.06±10.91 years and the controls’ mean age was 41.18±13.75 years. Forty-four (28.9%) of the patients were male and 108 (71.1%) were female. The demographical, clinical findings are shown in Table 1. Ten (6.6%) patients had been diagnosed with clinical isolated syndrome, 119 (78.3%) patients with relapsing remitting MS, and 23 (15.1%) patients with progressive MS. The mean MS disease duration was 10.42±6.47 years and the mean EDSS score was 2.13±1.69. The education levels were examined into 3 groups according to their education periods; 74 (48.7%) patients had a low education level, 31 (20.4%) patients a middle level, and 47 (30.9%) had a high education level. Most of the patients’ first attack was sensorial (30.9%), motor symptoms (27%), optic neuritis (23%), brain stem symptoms (14.5%), followed by others (4.6%). Except for 11 patients, all of them were taking MS treatments and most were treated with interferon beta-1a (47%).
- Demographic and clinical findings of population.
One hundred and thirteen patients (63.2%) mentioned cognitive symptoms. According to the neuropsychological tests, verbal fluency was affected in 133 patients (87.5%). The verbal short-term memory test performance was normal in 75 patients (49.3%), 65 patients (42.8%) had medium, and 12 patients (7.9%) had poor performance. According to the Beck Depression Inventory, 54 patients (35.5%) had depression and we excluded 19 patients who had severe depression. The Stroop test was affected more, compared with other cognitive tests, where the disease had progressed in patients with MS (p<0.0001, r=0.507). Apart from the Stroop test, another test that deteriorates mostly in correlation with EDSS is the visual memory tests (p<0.0001, r=-0.425). The CDT has been shown to give an indication of the cognition of patients with MS, most strongly regarding visual memory (p<0.0001, r=0.625).
In the 4-point and 10-point scoring methods, the CDT scores were significantly different between the patients and the controls (p=0.003, p=0.002). The mean CDT scores based on the 4-point in patients were 3.01±1.11 and according to the 10-point they were 7.57±3.2. In both the 4-point and 10-point scoring methods in the CDT, a statistically significant difference was found in patients with SPMS compared with the RRMS and CIS types (p<0.0001). However, we did not find any significant difference in the CDT between the controls and patients in the early stage of the disease (p=0.6, p=0.7) (Table 2). There was a significant negative correlation between age, disease duration, number of attacks, the EDSS, and CDT (r=-0.238, p<0.0001, r=-0.226, p=0.005, r=-0.190, p=0.019, r=-0.475, p<0.0001). In addition, there was a significant positive correlation between the education level and the CDT (p<0.0001). The correlation strength between the CDT and EDSS’ (p<0.0001, r=-0.475) was more than the correlation between the MMSE and EDSS’ (p<0.0001, r=-0.231). Also, significant correlations were determined between the CDT and all cognitive domains. There was a positive correlation between verbal fluency, verbal learning, verbal short-term memory, visual learning, visual memory, the Symbol Digit Modalities Test, MMSE and the CDT. There was a negative correlation between the Stroop test, Beck Depression Inventory, and the CDT (Table 3).
- The comparison of the clock drawing test scores.
- The significant correlation between CDT and all cognitive domains.
According to the multivariate linear regression model, the CDT had a statistically significant effect on the digit span test, Stroop test, visual memory tests independent of disease duration, the EDSS score, and education levels that were determined.
In the ROC analysis, the 4-point scoring CDT diagnosis prediction performance was found AUC=60.1% (SE=0.036) of the patients and in the 10-point CDT was found AUC=60.9% (SE=0.036) of the patients than the controls, both of 2 CDT methods were similar.
The CDTs were statistically better in those who had sensory attacks as the first attack than those who had motor attacks and brainstem attacks (p<0.0001) (Table 4).
- The relation between CDT and onset symptom of disease.
Discussion
In this study, we aimed to show the importance of the CDT to determine cognitive status in patients with MS. In clinical practice, the CDT is a quick and practical test. We also compared CDT with MMSE that is the other quick and practical test. We obtained good results from the CDT. The CDT is more valuable than MMSE when evaluating clinical progression in patients with MS. In some studies similar to ours, cognitive impairment was among the important causes of MS disability.11,12 Cognitive impairment has been shown to lead to occupational disability, social disability, and poor quality of life in patients with MS.13 It is well known that among patients with MS, women are in the majority, and the same is true in our population.14
It has been reported that RRMS was seen most frequently in approximately 85% of the patients, and in our population, approximately 78% of the patients had been diagnosed with RRMS. At the onset of the disease, our patients’ most common symptoms were sensory symptoms in the arms and legs, as also shown in other studies.15 Ninety-six patients (63.2%) had cognitive complaints in our study. Executive functions, visuo-spatial functions, free verbal recall, and verbal memory losses are generally observed cognitive impairments in patients with MS.13 In our study, the Stroop test was the most affected area in the cognitive evaluation with the progression of MS disease. These were followed by visual memory and verbal fluency tests. The Stroop test is used to evaluate executive functions by measuring selective attention, cognitive flexibility, and processing speed. The CDT evaluates for visuospatial organization and executive functions.6 This was also shown in our study, and the CDT provided information that patients MS were mostly affected by visual memory areas.
The CDT results were significantly different between the patient and control groups in our study. However, in the early period of the illness, we could not find a difference between the patients with MS and the control groups in the CDT as in Kirac et al.8 Studies have also defined cognitive involvement differently according to MS types. It has been reported that cognitive loss is more pronounced in PPMS and SPMS than in RRMS.16 We also showed that the CDT findings were significantly impaired in progressive MS compared with those with RRMS and CIS.
Age, disease duration, disability, and education level are also important factors for cognitive impairment in MS.3 We also found that the CDT values decreased with the increase of EDSS, age, and disease duration, while the CDT values increased with the increase in education level.
Heled et al17 have showed the relationship between clinical status and cognitive impairment using EDSS and neuropsychological tests in a longitudinal study. High EDSS scores indicated higher cognitive impairment.Also, Mocca et al18 reported that one neuropsychological domain could be a predictor clinical status. The MMSE is a frequently used, practical, and inexpensive test to determine cognition, but its specificity and sensitivity are very low. Its sensitivity was found to be 28% in MS-related cognitive loss.19 In our study, the correlation between the EDSS and CDT scores of the patients was found to be much stronger than the correlation between the EDSS and MMSE scores. This can be related that the CDT reveals disease clinical status more strongly than the MMSE.
It is not yet possible to define a uniform cognitive impairment in patients with MS, but it has been shown that some cognitive areas are more affected. In MS, while generally language functions, semantic memory, short-term memory, and recognition are preserved, sustainable attention, processing speed, executive functions, and visuo-spatial organization are impaired.13 In our study, the CDT was found to be effective in cognitive areas related to processing speed, sustained attention, executive functions, and visual memory regardless of variables such as disease duration, EDSS, and education level.
In our study, we researched the relationship between cognitive function and the first attack type, which we know, was not covered in previous studies. The CDT results were statistically better in those whose disease had started with a sensory attack, compared with those whose disease had started with a brainstem and motor attack. It is known that patients with MS who have sensory symptoms at onset have a better clinical course.20 In our article, we support this information by examining the relationship between attack and cognitive status.
Previous studies have also investigated the effectiveness of the CDT in MS patients6,8 but our advantages over those studies are firstly, the comparison of the patient group with the control group, secondly, the higher population number, and thirdly, the comparison of the CDT in the patient group with a test battery with more effective and reliable results such as the NPT.
Our study also had some limitations. First of all, we could not do the NPT with the healthy control group because it requires a lot of time and costs. In addition, the number of patients with progressive MS and CIS in our patient population was quite low. Finally, the comparison of the test findings and imaging findings of patients with cognitive impairment would have made the study stronger. In further studies, a more homogeneous patient group and the determinacy of the CDT for cognitive impairment can be investigated together with brain imaging.
Conclusion
The CDT is a very practical, inexpensive, and reliable method for detecting cognitive impairment in MS patients. The CDT has a stronger determination in detecting progression in patients with MS than the MMSE. Additionally, the CDT results showed that cognitive impairment was significantly less affected in people with sensory first-attack symptoms compared with other types of symptoms in onset MS.
Acknowledgment
We would like to thank ‘Scribendi Editing and Proofreading Service (www.scribendi.com)’ for English language editing and contributions to our manuscript.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received February 14, 2022.
- Accepted August 2, 2022.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.