


Abstract
Parkinson’s disease (PD) is a progressive widespread neurodegenerative disorder affecting the brain. It is characterized by dopaminergic neuron degeneration in the substantia nigra pars compacta (SNpc). Current therapeutic options ease the symptoms of PD; however, they have multiple undesirable effects and do not slow the disease progression. Exercise by itself has many positive impacts on general health. In this review, the positive impact of different forms of exercise were found to improve motor and non-motor symptoms in PD. Exercise effects is mediate by multiple mechanisms, including the upregulation of brain-derived neurotrophic factor, α-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid receptor, and autophagy regulating proteins; and downregulates proinflammatory cytokines. In this review, the significance of exercise in PD, as well as in the prevention and maintenance of the disease was discussed. Many questions are left unanswered in this manuscript, including potential genetic factors underlying response to exercise. Therefore, further high-quality studies on humans are needed.
Parkinson’s disease (PD) etiology is not fully resolved, notwithstanding over 2 centuries of PD research. Parkinson’s disease is connected to multiple epidemiological variables, including gender, age, race/ethnicity, environmental factors, and genetic factors. Degeneration of dopamine-producing neurons in the substantia nigra pars compacta (SNpc) is one of the 2 most important neuropathological features of PD. The second feature is the formation of Lewy bodies (LBs) containing aggregates of α-synuclein1,2 and ubiquitin.3 In the nigrostriatal pathway, the dopaminergic neuron’s cell body is in the SN, and their axons and terminals extend to the striatum. As an outcome of dopaminergic neuronal loss that expresses a high level of neuromelanin, clinical symptoms appear. In PD patients, neurodegeneration was concurrent with a reduction in the messenger ribonucleic acid (mRNA) level of dopamine transporter by 57% in comparison to an age-matched control.4,5 In addition, patients with PD subjected to FP-CIT PET/CT scan showed a reduction in dopamine transporter density in the SN by 25% and the striatum by 41%.6 Approximately 80% of striatal dopaminergic neurons are depleted at the start of clinical features, and around 60% of dopaminergic neurons in the SNpc were degenerated.7
Understanding the pathogenesis of PD necessitates a thorough knowledge of the SNpc anatomy, and the structural alterations in it. In this context, the SN is functionally and morphologically subdivided into pars compacta (ventral and dorsal tier) and pars reticulata.8 The ventral tier SN axons arborize to the striatal striosomes that arborize to the ventral tier SN. The dorsal tier arborizes to the matrix that projects to the pars reticulata and the ventral tier. The striosomes and matrix are histochemically distinctive compartments of the striatum. Death of the SNpc dopaminergic neurons in PD occurs mainly in the ventral tier. However, dorsal tiers are affected in healthy aging.9 Nigrostriatal pathway’s dopaminergic neurons contain 2 subtypes of dopamine receptors (D1 and D2). In the direct pathway, inhibitory dopaminergic neurons projecting to the globus pallidus interna (Gpi) express the D1 receptor. The indirect pathway contains dopaminergic neurons that express D2 receptors, which stimulate the GPi indirectly. In normal individuals, both pathways are in equilibrium. However, dopaminergic neurons degeneration in the SNpc causes a reduction of dopamine receptors in the striatum, causing an imbalance between the 2 pathways. As a result, motor impairment occurs.10
Variety of medication are used to treat PD among them is levodopa, which is a dopamine precursor.11 However, less benefit was observed on cognitive function, and the prolonged use of levodopa is associated with several undesirable side effects, including dyskinesia and motor fluctuation.12 Several other treatment alternatives are still under investigation including natural products such as mucuna pruriens.11,13 Deep brain stimulation of the subthalamic nucleus or the GPi is considered a standard surgical option, but up to 50% of patients who undergo this procedure suffer from complications, including speech difficulties, abnormal gait, depression, and cognitive decline.14
Exercise is a general term for a planned, organized, and regular physical activity.15 The advantages of physical exercise on health are well acknowledged; nevertheless, the mechanism by which exercise produces these benefits remains unknown. Over the last decade, the importance of exercise on neurorehabilitation in multiple neurodegenerative disorders has been established.16 In PD, exercise has become an essential element in the treatment plan.17 Multiple factors can contribute to the efficacy of exercise in PD, such as the specificity, intensity, frequency, difficulty, and complexity. In PD, exercises are often designed to incorporate motor and cognitive functions through dual tasking. These modalities include but are not limited to, treadmill exercise,18,19 Tai chi,20 tango dancing21,22 boxing,23 and cycling.24,25 The aim of this review is to elucidate the influence of physical exercise on PD, focusing of the following objectives: (1) The impact of different forms of physical activities on the motor and non-motor symptoms of PD; and (2) The mechanisms of action mediating these effects.
Motor performance in Parkinson’s Disease (PD) and the impact of exercise
Parkinson’s disease can cause a wide range of motor abnormalities. Parkinson’s disease is characterized by 4 cardinal signs: (1) Tremor by a frequency of 4 to 6 Hz. (2) Rigidity of muscles. (3) Akinesia/bradykinesia (i.e., slowness in voluntary movement initiating). (4) Postural instability. In addition to these signs, dystonia, fatigue, inability to execute delicate motor tasks, reduce arm swing while moving forward, speech issues such as voice softness, lack of facial gestures, micrographia (small size and cramping in handwriting), dysphagia, and loss of libido have all been reported in Parkinson’s disease.26,27
Physical exercise is generally recommended alongside the pharmacological treatment of PD. Epidemiological reports have frequently shown that regular aerobic exercise with moderate intensity has a significant impact on reducing the risk of developing the disease.28 Because of the lack of specificity in most research regarding the frequency, intensity, and length of exercise, Alberts and Rosenfeld examined available data from animal and human studies to conclude that 30-40 minutes 3 times a week, reaching 60-80% of heart rate reserve or 70-85% of heart rate max, may slow the decline of the disease.28 For example, Ergun et al29 studied the outcome of aerobic walking on motor control, non-motor signs and symptoms, and the cognitive functions of PD in a randomized clinical trial. Subjects were required to complete 45 minutes of exercise 3 times a week for 6 months. The study concluded that aerobic walking in a community setting improved the maximum oxygen consumption, gait speed, axial functions, and rigidity scores on the Unified Parkinson’s Disease Rating Scale (UPDRS), which in turn enhanced motor function, fatigue, mood, executive function control, and quality of life in patients with PD.29 In another clinical study, the effect of cycling on bradykinesia, rigidity, and morbidity was investigated in 16 subjects with a mild to moderate idiopathic form of the disease.30 The treated group received a total of 6 sessions of high cadence cycling with a day off between sessions, and each session was 60 minutes long. Meanwhile, control subjects received 6 stretching sessions with a day off between sessions. The UPDRS was used to assess motor function and morbidity after each cycling or stretching session. The cycling group showed an overall improvement, while no change was observed in the UPDRS of the stretching group.30 It was also reported that aerobic exercise becomes effective in PD patients suffering from depression when combined with Qigong and Tai chi.31 Exercise as a non-drug therapy has been found to improve not only the physical health of early-staged PD patients but also motor learning ability by enhancing the plasticity of motor structures and muscle hypertrophy (Table 1).32,33
- Effect of exercise on different PD symptoms.
Recent accumulating evidence suggest a bidirectional pathway between the brain and the gut forming the gut-brain axis, which led to a shift in the paradigm in PD. Studies suggested that aging influence the alteration in gut microbiome composition of butyrate-producing bacteria that are responsible for the propagation of α-synuclein.34,35 Not unexpectedly, exercise was suggested as a possible factor mediating a change in gut microbiome in several neurodegenerative disorders including PD. Preclinical studies explored the possible mechanism wherein physical exercise modulates the microbiota. Exercise have shown to increase the activity of antioxidant enzymes (catalase and glutathione peroxidase), while decreasing pro-apoptotic proteins and inflammatory cytokines. As a result, exercise can lead to an overall decrease in inflammation.35,36 Unfortunately, human clinical studies exploring the impact of exercise on the gut microbiota in PD are still limited.
Gait and balance in PD and exercise
Gait abnormality is an important characteristic feature of PD and worsens as the disease worsen. Gait dysfunction in PD is very complex and changes as the disease stage progresses. A decrease in the speed of gait, stride and step length, and a sudden brief freeze in the middle of the gait cycle are all features of gait abnormalities in PD patients. Numerous studies have found that physical exercise training either with body weight support or without it can improve wide range of gait parameters. Transitional movements are challenging for patients with PD, especially whenever the center-of-mass shifts away from their base-of-support, such as getting up from a chair, turning, and stairs negotiation.37 Progressive resistance training twice a week was found to improve posterior displacement after 10 weeks.38 In addition, treadmill exercise was found to positively impact stride time and swing time variability, leading to a more stable gait rhythm.39,40,41 Different forms of exercise were also found to improve gait,39 and reduce the number of falls.42,43 For example, walking and Nordic walking exercise exhibited an enhancement in different gait parameters, including speed, stride length, gait variability, and maximum speed in patients with moderate motor symptoms.44 Individuals with early-stage PD who received body-weight-supported treadmill exercise incorporated with gait training were found to engage in gait training faster than their normal speed.18 Over 24 sessions (3 sessions a week), as the speed gradually increased, patients had improved gait parameters and balance. Moreover, the levels of dopamine 2 receptor (D2) in the caudal basal ganglia in those patients showed an increased following a PET scan with 18F-fallypride.18 These improvements in motor functions with increased D2 receptors might contribute to the effect of exercise on neuroplasticity and induce modification of the indirect pathway of automaticity, deriving an abnormal inhibitory effect. The addition of an external cue that facilitates more complexity during gait training, such as music, demonstrated a trivial but significant improvement in the patient’s balance and stride length.45,46,47 Advanced technology, such as virtual reality (VR) using a computerized simulation, was implemented into rehabilitation to provide personalized training.48 The VR provided participants with real-time interaction with virtual images and objects.49,50 There is growing evidence that VR can be used as rehabilitation to improve gait and balance in multiple neurological disorders such as post-stroke and PD. The VR rehabilitation was found to improve gait and balance significantly.51,52,53 The VR produced a similar impact on long- and short-term effects on gait and balance.43,54 Moreover, VR training exercises reduced the risk of falls.55 VR training using consoles such as the Nintendo Wii™ showed an improved performance in daily activities after 14 sessions. However, no improvement was observed with Wii-based cognitive exercise.56
Non-motor symptoms
The degeneration of dopaminergic neurons in the basal ganglia not only affects motor function but also causes cognitive impairment, which appears in the early stages of the disease and worsens as the disease progresses.57,58,59 Aside from well-documented motor symptoms, most patients suffer from PD-associated non-motor symptoms, including cognitive impairment, mood disorders, sleep disturbance, fatigue, and anxiety.60,61,62
Cognitive impairments vary from minor changes to mild cognitive impairments, which do not significantly impact daily activity, to dementia, which substantially impacts the daily quality of living of the patient. The incidence of PD dementia was anticipated to be approximately 0.5% when patients are over 65 years old. Previous clinical trials have found that dancing and treadmill exercise could prevent declining of cognitive function and may be able to improve it.63 It is well established that different forms of physical activity improve neuroplasticity; for example, aerobic exercise combined with strength exercise improved frontal lobe-based executive function more than aerobic exercise alone.64 Executive functions improved by exercise include judgment, planning, and problem-solving.63 Combining treadmill exercise with VR reduces the activation of the inferior frontal gyrus and Brodmann area 10 times more than treadmill exercise alone enhances the efficiency of the cognitive network.65,66
Patients with PD suffer from disruptive sleep, which is one of the most common non-motor features of PD.67 Around 37% of PD patients have high awakened frequency and sleep fragmentation throughout the night.68 Sleeping disorders associated with PD could develop due to the degeneration of specific neurons, leading to an alteration in sleeping control neurotransmitters. However, pharmacological treatment with dopaminergic agonists used in the management of PD symptoms was found to worsen the symptoms of sleeping disorders. Regular exercise was found to improve the quality of sleep in young and old patients; however, older patients’ sleep-onset latency was weaker. Acute exercise was proven to improve sleep time and onset latency and decrease rapid eye movement sleep without impacting total sleep time.69 Even though the impact of exercise was small, it was affected by the time of day that the exercise was completed. Three to 8 hours before sleep had better outcomes. In addition, exercise duration played a role in the quality of sleep, with longer exercise periods having better results.69
Depression is a major issue in patients with neurodegenerative disorders, especially in PD, affecting around 44%-51.7% of patients.70,71 Despite depression being a common non-motor symptom in PD, only a few studies have examined the impact of exercise on depression in patients with PD. However, aerobic exercise was found to have positive psychological outcomes in adults who exercised for 12 weeks.72 Participants in this study displayed a significant improvement in depression, as evaluated by the Beck Depression Inventory.72 In a different study, half an hour of walking on a treadmill for 10 days was sufficient to have a significant effect on major depression.73
Mechanisms underlying the impact of exercise
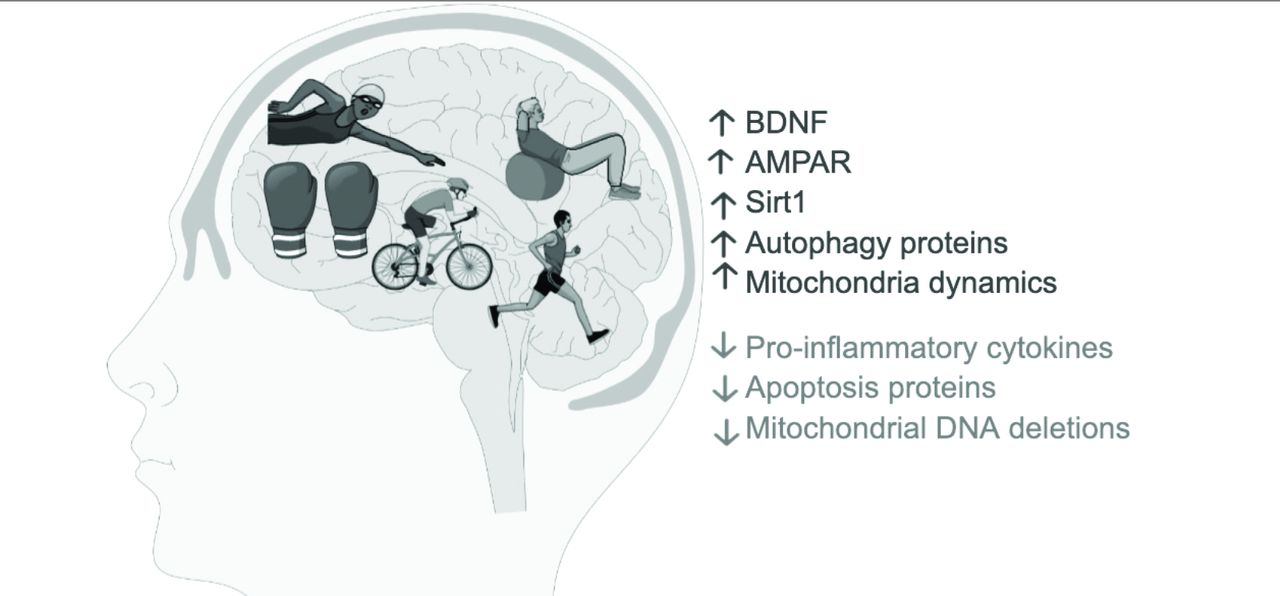
The exact mechanism by which exercise impacts PD symptoms is still unknown; however, multiple mechanisms have been proposed that could improve motor and non-motor symptoms (Figure 1). The impact of skilled exercise on motor behavior is believed to be due to an improvement in the prefrontal-striatal circuit neuroplasticity via increasing the level of brain-derived neurotrophic factor (BDNF) in the striatum and the SN.74,75 This effect is initiated by binding to tropomyosin receptor kinase B (TrkB).76 Treadmill exercise has a neuroprotective effect in PD animal models by increasing the activity of Sirt1, which reduces neuroinflammation and improves mitochondrial function.77 As mentioned previously, neuroplasticity has a significant role in PD treatment by exercise. The effect of high-intensity treadmill training on neuroplasticity is induced by increasing the expression of the α-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid receptor (AMPAR) subtype glutamate receptor 2 (GluR2) since the glutamatergic system is known for its role in motor learning.78 On the other hand, GluR1 was previously reported to be elevated in the surviving synapse during the disease development, causing over-excitation. Exercise can counteract the converse expression of GluR1 by increasing the expression of GluR2 in the synapse.78 The PD is characterized by the upregulation of inflammatory factors in the brain and skeletal muscle cells, leading to muscle atrophy via overexpression of IL-1β, TNF-α, and NFκB.79,80 Physical exercise reduces the expression of pro-inflammatory cytokines in aging skeletal muscle cells.81 Also, regular exercise was found to reduce the rate of generation of reactive oxygen species (ROS) via its ability to increase the antioxidant capacity of the cells.82
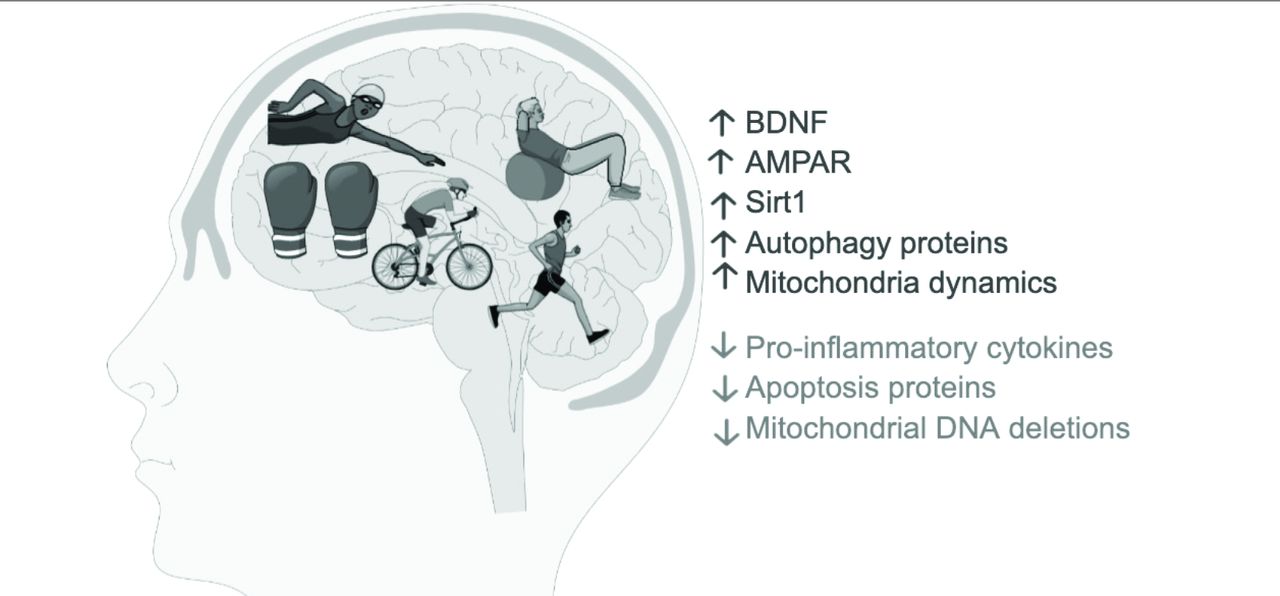
- Proposed mechanisms that may contribute to improvement of PD symptoms. PD - Parkinson’s disease
In addition to the abovementioned mechanisms, other mechanisms that can slow down the progression of the disease include the inhibition of astrocytes and microglia after treadmill training, as demonstrated in the PD animal model induced by rotenone.83 Another study demonstrated the neuroprotective effect of treadmill training by increasing the protein expression of autophagy-regulating proteins, such as LC3-II, P62, and Beclin1, and decreasing the protein expression level of apoptosis proteins caspase-3 and BAX.84,85
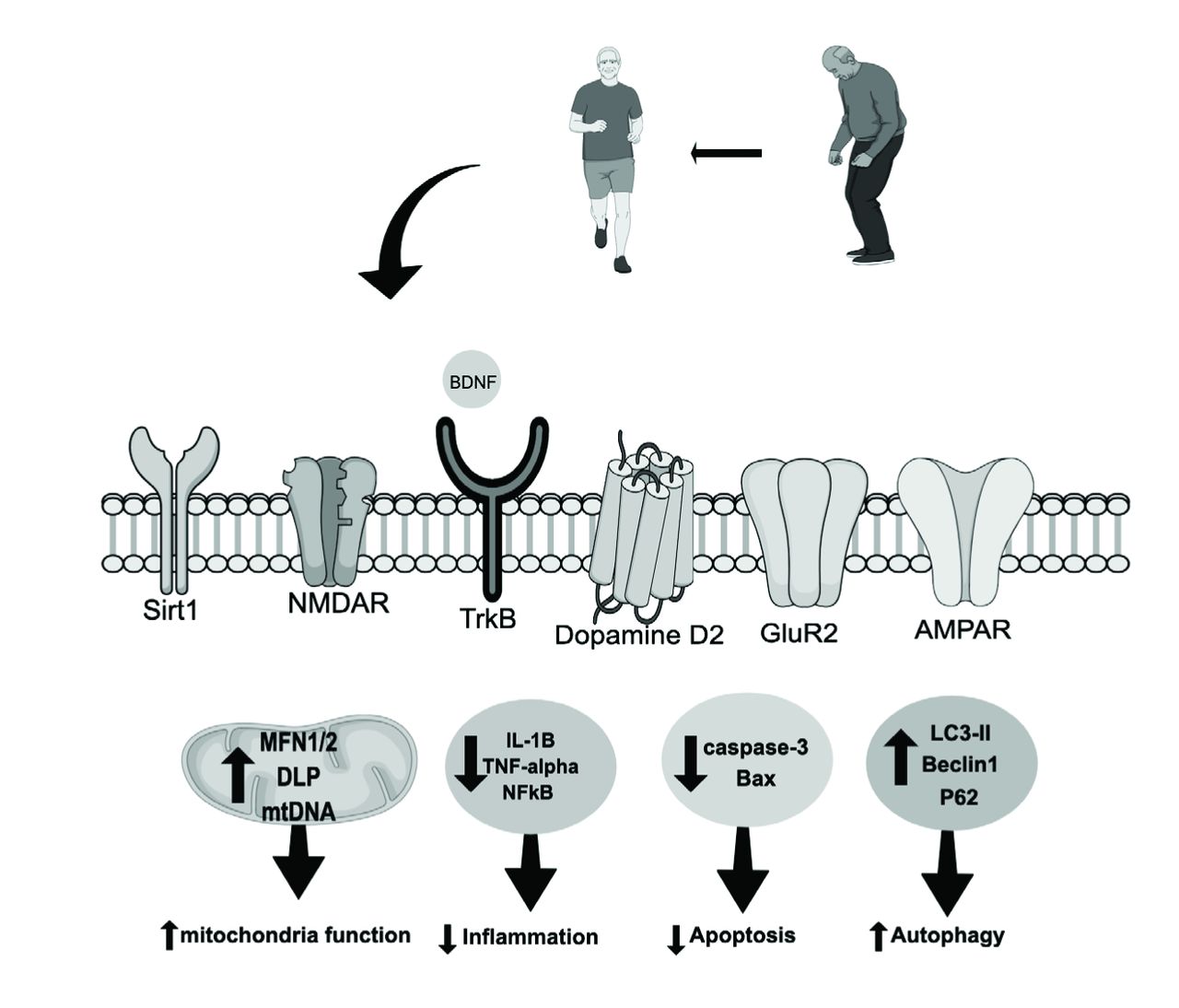
Mitochondria are organelles that regulate multiple cellular functions, such as adenosine triphosphate (ATP) production. The dysfunction of mitochondria is associated with multiple neurological conditions, including PD.86,87 Mitochondria are dynamic organelles that become disrupted in PD; however, physical activity improves mitochondrial fission and fusion by upregulating mitofusin 1/2 (MFN1/2) and dynamin-like protein (DLP).88,89 In addition, exercise rescues mitochondrial DNA depletion by increasing the mitochondrial DNA copy number and decreasing the frequency of point mutations (Figure 2).90

- Mechanisms influenced by exercise in PD. Physical exercise increases the level of neurotrophins in the brain. This upregulation decreases pro-apoptotic proteins, increasing autophagy, reducing neuroinflammation. In addition, exercise upregulates mitochondrial fission and fusion proteins, and increasing mtDNA copy number.
Conclusion
Collective evidence has revealed the importance of exercise in PD. This review shed the light on the importance of exercise as an effective method the lower the risk of developing the disease. Different forms of physical exercise promote improvement of motor symptoms such as bradykinesia, gait, and balance. Additionally, exercise could alleviate not only motor symptoms but also nonmotor symptoms such as cognitive impairments, judgment, depression, and sleep disorder. Meanwhile, the positive impact of exercise is associated with type of exercise, duration, and intensity. The therapeutic and protective effects of exercise is mediated by improving mitochondrial function, increasing the production of GDNF, decreasing pro-apoptotic proteins, and decreasing neuroinflammation.
Acknowledgments
The author would like to thank proof-reading-service (https://www.proof-reading-service.com) for English language editing.
Footnotes
Disclosure. The authors declare no conflicting interests, support or funding from any drug company.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.
- 92.
- 93.
- 94.
- 95.
- 96.
- 97.
- 98.




{kind=link}
{kind=link}