


Abstract
Objectives: To report cases of cerebral phaeohyphomycosis at a tertiary hospital in Riyadh, Saudi Arabia. Phaeohyphomycetes are a widely distributed group of fungi whose cell walls contain 1,8 dihydroxynaphthalene-melanin. Cerebral infections caused by these fungi are uncommon and primarily associated with neurotrophic phaeohyphomycetes.
Methods: In January of 2020 we looked back to identify cases of culture-positive cerebral phaeohyphomycosis from our medical records at King Faisal Specialist Hospital and Research Center in Riyadh, Saudi Arabia. Data on demographics, potential risk factors, clinical presentation, treatment, and outcomes were analyzed.
Results: Twelve cases of cerebral phaeohyphomycosis were identified, of which 4 were caused by Rhinocladiella mackenziei and the other 8 were caused by various phaeohyphomycetes. There were 2 cases caused by Neoscytalidium dimidiatum, and one case each caused by the following: Acrophialophora fusispora, Chaetomium atrobrunneum, Exophiala dermatitidis, Exerohilum rostratum, Fonsecaea pedrosoi, and Cladophialophora bantiana. Most patients (10 of 12) had underlying immunosuppression. R. mackenziei caused a brain-only infection manifesting as abscess formation. Four patients survived for more than a year after therapy. Surgical evacuation and triazole therapy with posaconazole or itraconazole, alone or in combination with other antifungal agents, were associated with success.
Conclusion: Cerebral phaeohyphomycosis is an uncommon fungal infection that primarily affects immunocompromised patients and is associated with poor prognosis. R. mackenziei is the most prevalent fungus in our facility and has been linked to a universal mortality.
Fungi are widespread, are present in the soil, and decompose organic matter. The presence of 1,8 dihydroxynaphthalene-melanin in the cell walls of phaeohyphomycetes is characteristic of many different genera of fungi. Phaeohyphomycosis refers to various diseases, such as cutaneous, subcutaneous, cerebral, and disseminated diseases.1
In 1974, the term phaeohyphomycosis was coined by Ajello et al2 to describe subcutaneous and systemic infections caused by fungi that produce dark-brown septate hyphae in lesions.2 Melanin has been proposed to act as a virulence factor in these species through various mechanisms. By neutralizing free radicals and hypochlorite, it protects fungi from phagocytic cells and exerts oxidative burst effects. Furthermore, melanin can bind to hydrolytic enzymes, preventing their action on the fungal plasma membrane.1 However, factors other than melanin levels may be at play. Chitin has also been proposed as a possible virulence factor for cell-wall enrichment.1
Certain species of these fungi have been reported to cause brain abscesses with rare involvement of other sites and are considered neurotrophic.1 Cladophialophora bantiana is the most common dematiaceous fungus reported to cause brain infection.2 Rhinocladiella mackenziei has been detected in Middle Eastern residents, particularly those in the Gulf region.1 In addition to a few imported cases in the United Kingdom and France, Pakistan and Iran have reported more recent cases.3-6 In the United States, an outbreak of meningeal phaeohyphomycosis caused by Exerohilum rostratum was linked to contaminated methylprednisolone solution injected primarily into the back.7 However, reporting infections caused by these fungi is not required; thus, there is no accurate estimate of their incidence and prevalence.8 Here, we report our experience with several cases of cerebral phaeohyphomycosis from a single center.
Methods
A retrospective, single-center cohort study was conducted at King Faisal Specialist Hospital and Research Center in Riyadh, Saudi Arabia from January 1999 to December 2000 based on a review of electronic medical records and medical charts. Cases with a positive culture of phaeohyphomycetes recovered from brain biopsies or cerebrospinal fluid (CSF) were identified using a microbiology database. The diagnosis was based on fungal microbiological recovery. Morphological identification of the growth characteristics and slide culture served as the primary diagnostic test at the species level. Two additional cases were confirmed via polymerase chain reaction (PCR) amplification and ribosomal RNA sequencing. A review of the data included the following: demographics; potential risk factors including underlying condition, surgeries, steroid therapy, and other immunosuppressive therapies; and clinical presentation, treatment, and outcome. For the descriptive analysis, Microsoft Excel and IBM Statistical Package for Social Sciences (SPSS) Statistics version 22 (IBMCorp, Armonk, NY, USA) for Mac were used. This study was approved by the review board of our institution. The authors confirm that the ethical policies of the journal, as outlined on the author guidelines page, have been adhered to. A literature review of similar cases was also conducted.
Results
We identified 12 cases of cerebral phaeohyphomycosis through brain tissue cultures and one patient with persistently positive CSF cultures. The histopathology of all patients, except one, was positive for fungal hyphae. Two cases were confirmed via PCR amplification and RNA sequencing (Table 1). The patients were from various regions of Saudi Arabia, with the exception of 3 patients from the same region.
Of the 12 patients, 8 were men and 4 were women. In terms of the causative agent, four cases were caused by Rhinocladiella mackenziei, and 2 by Neoscytalidium dimidiatum. Meanwhile, the remaining six cases were caused by various phaeohyphomycetes: Acrophialophora fusispora, Chaetomium atrobrunneum, Exophiala dermatitidis, Exerohilum rostratum, Fonsecaea pedrosoi, and Cladophialophora bantiana (Table 1).
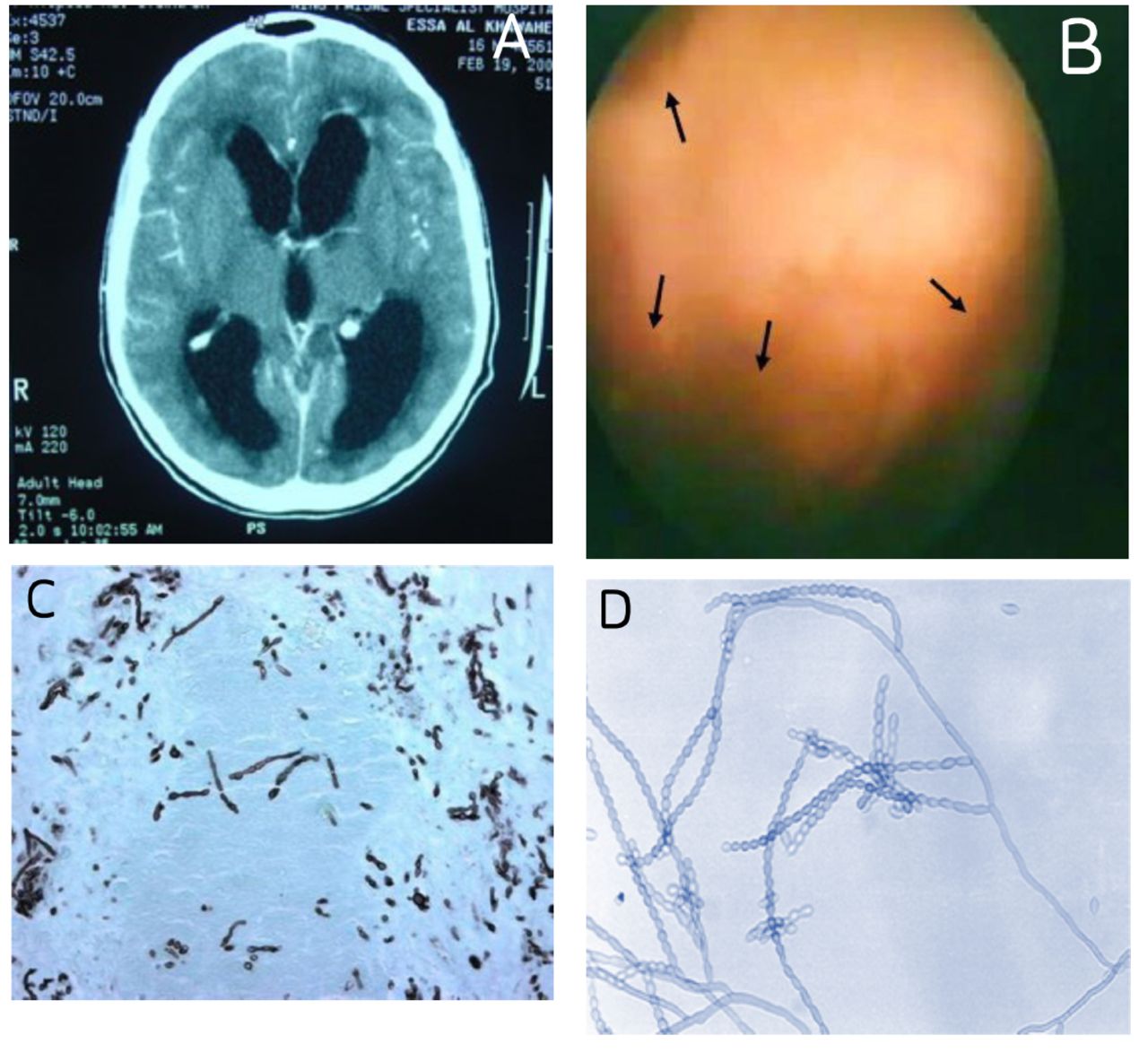
Ten patients were immunocompromised because of organ transplantation or cancer, and one was diagnosed with chronic granulomatous disease (CGD). A young patient with C. bantiana infection had no discernible immune deficiency despite a comprehensive immunological evaluation (Figure 1).

- Radiographic, ventriculoscopic, and histopathological morphologies of Cladophialophora bantiana A) A patient with hydrocephalus due to a brain infection caused by Cladophialophora bantiana. B) Ventriculoscopy revealed extensive ventriculitis, with fungus incorporating the lateral ventricles (arrows). C) Gomori methenamine silver histopathology stain of the brain revealed septate hyphae, and D) fungal culture revealed the characteristic morphology of C. bantiana.
Of the 4 patients infected with R. mackenziei, 2 received kidney transplants, one received a liver transplant, and one was immunocompetent. R. mackenziei caused an infection that occurred solely in the brain, resulting in abscess formation. Other phaeohyphomycetes involved different organs, such as sinuses, or disseminated multiorgan involvement.
After diagnosis, 4 patients survived for more than a year. One patient with CGD survived for 10 years after receiving suppressive antifungal therapy. One of the 4 patients with R. mackenziei infection survived for over 3 years on antifungal therapy. Nine of the 12 patients were treated with medical therapy and surgical resection. Most patients underwent surgery and received antifungal combination therapy (Figure 2). Surgery was combined with the triazole antifungal agents posaconazole or itraconazole to treat survivors.
Discussion
Phaeohyphomycosis causes a wide range of diseases, including those that are cutaneous, subcutaneous, cerebral, and disseminated,8 with a mortality rate of 70% in cerebral and disseminated diseases.9 C. bantiana is the most common phaeohyphomycete that causes cerebral infections. More than 80 cases of cerebral phaeohyphomycosis caused by C. bantiana infection have been reported worldwide, and nearly half of these cases involve immunocompetent individuals.8 E. dermatitidis is the second most common phaeohyphomycete that causes cerebral infections.9 Only one case of each was identified in our study. One case was caused by E. rostratum, a common saprobic fungus on plant debris that rarely causes clinically significant infections, except in immunocompromised patients, although localized infections have been reported.10
In 2012, the Centers for Disease Control and Prevention (CDC) in the United States reported an outbreak of fungal meningitis caused by direct inoculation of methylprednisolone contaminated with E. rostratum into human tissue. The contaminated injection was identified and removed from clinical use, ending the outbreak.7 Our E. rostratum-infected patient was pregnant and had no history of injections or immunocompromised status. We also encountered a case caused by F. pedrosoi, a well-known cause of chromoblastomycosis in tropical climate zones, particularly in South America.11 N. dimidiatum (syn. Scytalidium dimidiatum) is a fungus that causes onychomycosis and tinea pedis but rarely causes cerebral infection.12 It caused a fatal infection in 2 of our patients who had recently received kidney transplants. C. atrobrunneum has been reported to cause cerebral infection in patients with hematological malignancies, as observed in our patient with acute myeloid leukemia. In addition, the fungus was repeatedly cultured in the CSF.13 Meanwhile, A. fusispora is a rare cause of phaeohyphomycosis, with only 5 cases and 2 cases of brain abscesses reported in medical literature, including our case.14 Cases of cerebral phaeohyphomycosis are typically sporadic and unrestricted by geography, except for those caused by R. mackenziei, which are typically restricted to the Middle East. Recently, Iran, Pakistan, the United Kingdom, and France have reported cases.3-6 To the best of our knowledge, as of July 10, 2022, 37 cases of R. mackenziei have been reported,15,16 12 of which originated in Saudi Arabia (Table 2).17-26
- Cases of R. mackenziei reported in Saudi Arabia.
R. mackenziei affects immunocompromised and immunocompetent individuals. Nine of the 12 reported cases in Saudi Arabia were immunocompetent. In our cases, 3 patients were immunocompromised and one was immunocompetent. Recent reports have primarily focused on immunocompromised individuals. Only 2 cases of prolonged survival with R. mackenziei have been reported in Saudi Arabia and the United Kingdom.5,26 The patients in both cases underwent surgical excision and posaconazole antifungal treatment.
The geographical restriction of R. mackenziei remains unclear. The fungus has not been isolated from nature, and its Middle Eastern distribution suggests a preference for the saprophytic phase in arid climates.21 In addition, diagnosis of phaeohyphomycosis is challenging because it depends on the histopathology and culture. Phaeohyphomycosis is characterized by darkly pigmented hyphae, which can be observed more clearly with Masson-Fontana melanin staining. However, this stain can also be positive for hyaline fungi, indicating a low specificity. PCR amplification and molecular sequencing have assisted in the classification and identification of fungi including black molds. In contrast, application of serology in the diagnosis of phaeohyphomycosis has not been reported. Cases with favorable outcomes suggest that medical and surgical treatment are the treatment of choice for cerebral phaeohyphomycosis.1
Typically, amphotericin B and the triazoles itraconazole and posaconazole are used for treatment. Microdilution methods for in vitro antifungal susceptibility testing have not been standardized, and it is difficult to determine the best therapy without validated minimal inhibitory concentration breakpoints. The comparison of various antifungals has only been performed in animal models. In a study conducted on murine models, posaconazole was superior to amphotericin B and itraconazole.28 Amphotericin B treatment is generally ineffective. When surgery is impossible, combination therapy with extended-spectrum triazole and flucytosine, which has in vitro activity against many black molds, has been suggested.14 There is limited data on echinocandins as antiphaeohyphomycete agents.
Few animal studies of combination antifungal therapies have demonstrated positive outcomes.29,30 In most of our patients, combination therapy was used; however, surgical resection was necessary for success.
Despite the findings, our study has some limitations. First, it is based on a case series; therefore, its findings cannot be generalized. Additionally, no comparison group was included in the description of the findings. However, we believe that our case series adds to the limited knowledge on intractable serious infections, significantly contributing to medical literature.
Conclusion
Rare and fatal cerebral phaeohyphomycosis is a fungal infection with a poor prognosis. R. mackenziei is the predominant fungus at our facility and is associated with a universal mortality, except in some cases treated with a combination of surgical and antifungal therapies.
- Received October 23, 2022.
- Accepted March 15, 2023.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.