


Abstract
Objectives: To study each atypical feature in atypical meningioma versus other grade 2 meningiomas and its possible relation to recurrence.
Methods: This is a retrospective study of patients with WHO grade 2 meningioma operated in our institution between 01/2008 and 12/2020. The rate of recurrence, reoperation and readmission were recorded during the follow-up period. A statistical analysis was done to determine the significance of each pathological feature in regard to recurrence.
Results: A total of 74 patients were included as WHO grade 2 meningioma with 60 (81%) patients having an AM and 14 (19%) patients with chordoid or clear cell meningioma. The mean age was 51 years±14. The most common location was meningioma abutting the frontal lobe (convexity). Major atypical features were more noted in the AM, however, there was no significant difference between AM and other types of meningioma. Increased Nuclear cytoplasmic ratio and cellularity were found significantly more in AM. The recurrence rate was 16.2%. No specific pathology feature (major or minor) nor the type of Grade 2 meningioma was significantly related to recurrence.
Conclusion: The types of WHO grade 2 meningiomas have similar prognosis and recurrence rates. There is no significant difference between the atypical features in indicating a more aggressive nature or risk of recurrence in grade 2 meningiomas.
The 2021 WHO classification of meningiomas describes grade 2 (atypical) meningiomas as having one major feature (4-19 mitotic figures / 10 high power field or brain invasion) or 3 out of 5 minor features (Small cells with high N/C ratio, Large and prominent nucleoli, Patternless or sheet-like growth, Foci of spontaneous or geographic necrosis).1 Grade 2 meningiomas compromise about 19-35% of all meningiomas2,3,4 and are considered to have a less benign nature than grade 1 meningiomas with more rapid disease progression and morbidity,5,6 and associated with higher recurrence risk.7 Clear cell meningiomas and chordoid meningiomas are considered to be a rare variant of meningioma.8,9
Many meningiomas with one or 2 atypical features, but not enough to fulfill the criteria to be atypical meningioma are reported as grade 1 meningioma. The significance of each atypical feature on the prognosis or how it affects and changes the natural history of the disease is not yet clear. In this study, we try to study each atypical feature in atypical meningioma versus other grade 2 meningiomas and its possible relation to recurrence.
Methods
Study design
This is a retrospective study of 74 who grade 2 meningioma diagnosed between January 2008 and December 2020 at King Saud University Medical City, Riyadh, Saudi Arabia. Data were collected from patients electronic and paper bases and final pathology reports. Patients with a confirmed pathological diagnosis of WHO grade 2 meningioma and underwent tumor resection in our center were included. Patients with no confirmed diagnosis, different meningioma grade, spinal meningioma and those with missing data/ follow-up were excluded. Borderline meningioma reports between grade 1 and grade 2 or between grade 2 and grade 3 were reviewed by a neuro- pathologist in our institute and the 2021 WHO classifications were applied to determine the final diagnosis.10
Data collection
Demographic data including age at diagnoses, gender and comorbidities were collected. The size and location of the tumor was determined from preoperative imaging, tumor size was defined by the largest diameter in centimeters, which is then subdivided to 2 groups, Tumors <5cm and ≥5 cm. The extent of resection was determined by the first postoperative imaging. Recurrence was determined by radiological evidence on follow- up imaging. Follow- up period was determined by their last documented out- patient clinic visit.
Postoperative assessment
The extent of resection was determined based on the first post operative MRI. Patients with evidence of subtotal resection on MRI received radiotherapy. Patients with gross total resection on MRI were observed with serial images. Patients with suspicion of recurrence on follow up MRI were discussed in our institutional tumor board and received radiotherapy after consensus.
Histopathology
All 74-pathology reports were reviewed to meet the 2021 WHO classification of tumors of the central nervous system as follows: fulfilling either 1 of 2 major criteria or 3 of 5 minor criteria. The major criteria are: 4 - 19 mitotic figures/10 high power fields and brain invasion. The minor criteria are: increased cellularity, small cells with high nuclear- cytoplasmic ratio, large and prominent nucleoli, patternless or sheet-like growth, foci of spontaneous or geographic necrosis.18 Ki-67 index (MIB-1) was also calculated.
Statistical analysis
Data entry and statistical analysis were performed using the Statistical Package for Social Sciences (SPSS) software version 26.0 (IBM Corporation, Armonk, NY, USA). Descriptive statistics (e.g. number, percentage, mean, range, standard deviation) and analytic statistics using Chi-square test, Fisher exact test and independent samples t-test were applied. P-values ≤0.05 were considered as statistically significant.
Ethical statement
The research was conducted ethically, with all study procedures being performed in accordance with the requirements of the World Medical Association’s declaration of Helsinki.
Results
A total of 74 patients with WHO grade 2 meningioma were included which represented almost one-third of all meningioma cases done in the period between January 2008 and December 2020 (35.2%). Age ranged from 9 to 83 (Mean 51.7±14.2) years. Forty- eight patients (64.9%) of patients were females and 26 (35.1%) were males. Sixty patients (81.1%) were diagnosed with atypical meningioma (Figure 1), 12 patients (16.2%) were diagnosed with chordoid meningioma (Figure 2), and 2 patients (2.7%) were diagnosed with clear cell meningioma (Figure 3). Tumor size was <5 cm in 49 patients (69%) and 5 cm or more in 25 patients (31%). Complete tumor resection (gross total resection) was achieved in 44 patients (62%) while the other 27 patients (38%) had partial resection. The mean follow-up period was 40.7 (±37.7) months with a median of 27 months (Table 1).

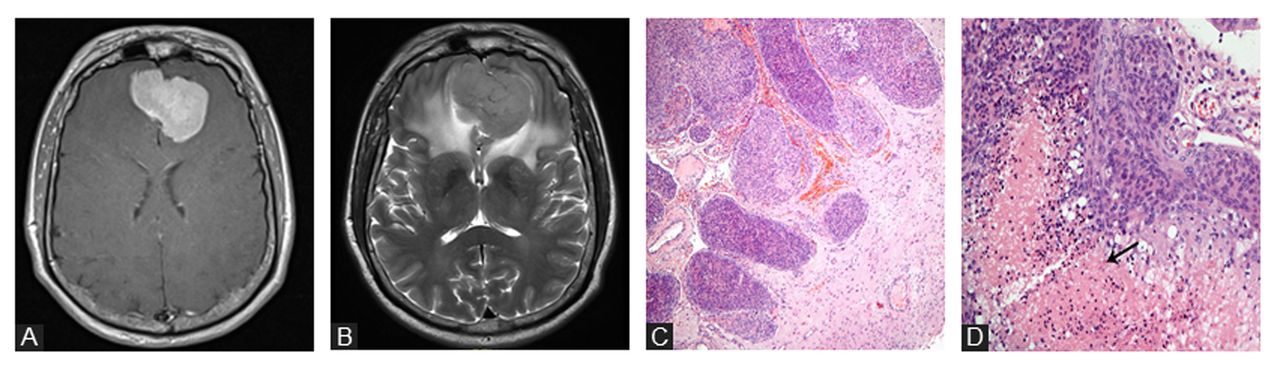
- A case of 47 years old male with Atypical meningioma A) Contrasted axial T1 weighted MRI of olfactory groove meningioma. B) T2 weighted MRI showing the meningioma with surrounding edema. C) A Hematoxylin and eosin (H&E)stained slide showing a meningioma invading the brain tissue in a finger-like pattern (H&E, X200). D) H&E stained slide showing an atypical meningioma, the tumor shows dense cellularity, small cell changes and necrosis (arrow, H&E, X200).

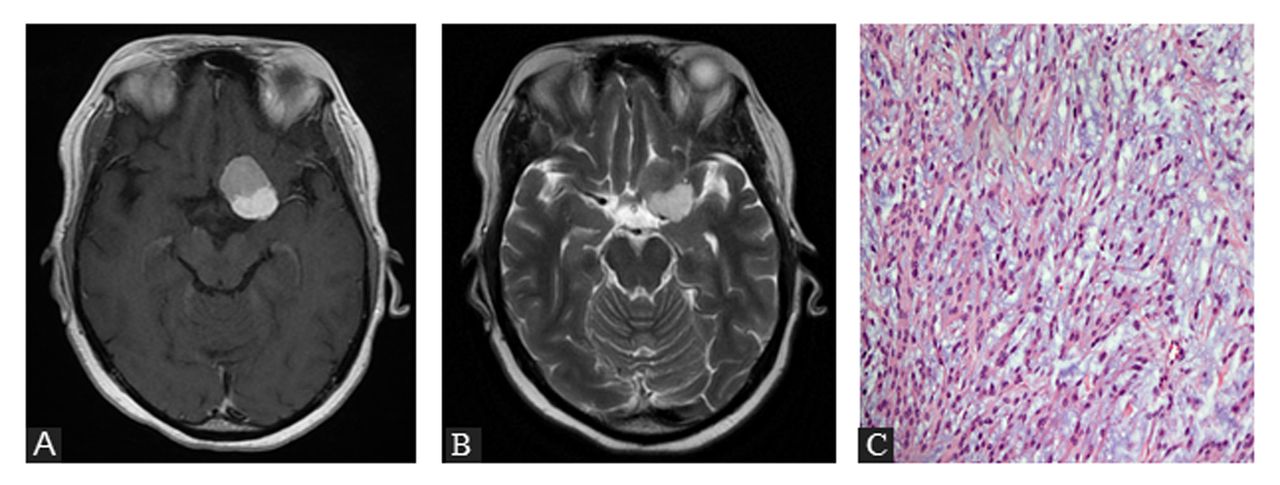
- A case of 39 years old female with Chordoid meningioma A) Contrasted axial T1 weighted MRI and B) T2 weighted MRI of a left paraclinoid meningioma. C) H&E stained slide showing a chrodoid meningioma with characteristic cords arrangement of the tumor cells in a stroma that is rich in myxoid material, mimicking a chordoma (H&E, X200).

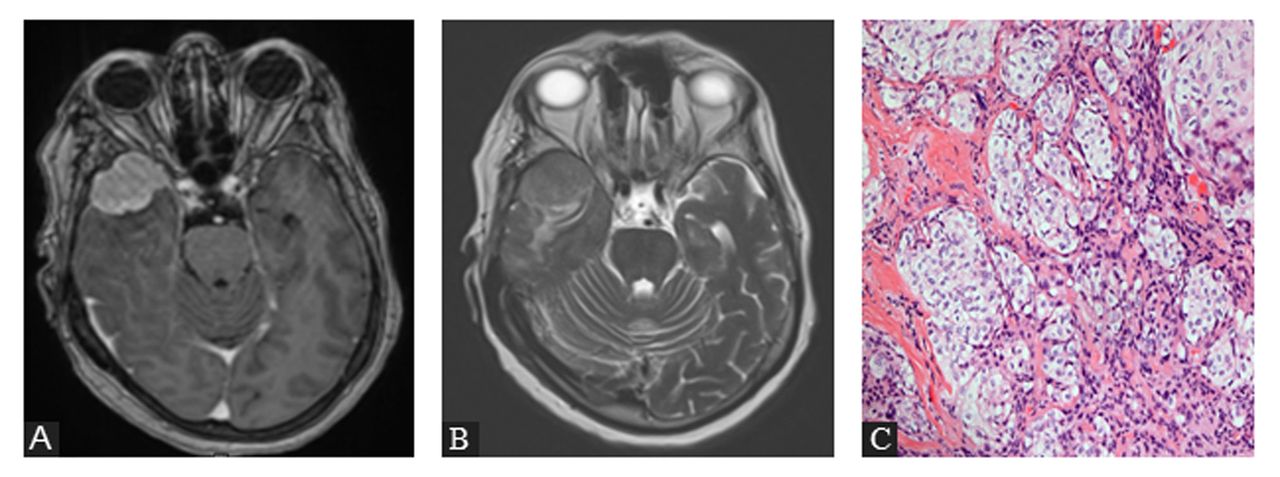
- A case of 75 years old female with Clear Cell Meningioma A) Contrasted axial T1 weighted MRI and B) T2 weighted MRI of a sphenoid wing meningioma. C) H&E stained slide showing a meningioma with features of clear cell subtype (H&E, X200).
- Demographic data of 74 patients with WHO grade 2 meningioma.
Most lesions were located in the skull base (46.6%) and convexity (31.5%) while midline meningiomas were found in 15 patients (20.5%) (Table 2).
- Meningioma location in 74 patients with WHO grade II meningioma.
Histopathological features and type of WHO grade 2 meningioma
Increased nuclear- cytoplasmic ratio was found more in patients with atypical meningioma with p-value 0.008, as well as increased cellularity (p=0.044) compared to chordoid and clear cell meningiomas. No significant difference in the number of patients with atypia (4 patients), mitotic figures (7 patients), loss of architecture (31 patients), brain invasion (14 patients), bone invasion (3 patients), necrosis (20 patients) and increased Ki-67 (40 patients) between all three types of WHO grade 2 meningioma. (Table 3)
- Pathologic features for atypical, chordoid and clear cell meningioma in 74 patients.
Characteristics associated with recurrence
A total of 12 patients (16.2%) of the 74 patients had evidence of radiological recurrence, with mean age of 51years (p=0.75). Nine patients (75%) were females, and 3 patients (25%) were males. Complete resection was achieved in 5 of the recurrence patients and partial resection was done in 7 of the recurrence patients (p=0.134). No significant association was found with histological subtype, size of the primary tumor or location of the tumor. (Table 4)
- Relationship between pathology features and recurrence rate in patients with WHO grade 2 meningioma.
Pathological factors associated with recurrence
None of the pathological features examined in our study were significantly associated with recurrence rate in patients with WHO grade 2 meningioma. Ten patients (16.6%) diagnosed with atypical WHO grade 2 meningioma had evidence of recurrence compared to 2 patients (14.2%) with chordoid or clear cell meningioma (p=0.564). Recurrence rate in sheet- like growth (22.5%), increased cellularity (13.6%), high nuclear- cytoplasic ration (13.6%), necrosis (20%), increased mitotic figures (25%), brain invasion (14.2%) and increased Ki- 67 (18.2%) were not statistically significant (Table 5).
- Factors associated with recurrence in WHO grade 2 meningioma.
Discussion
Grade 2 meningiomas have a less benign course compared to grade 1 meningioma.11 This is determined by a single or multiple histopathological features identified after resection of the tumor. The change in meningioma grade from grade 1 to 2 or from grade 2 to grade 3 determines the postoperative course of management and prognosis.12,13 However, the impact of each histopathological feature on the prognosis, and recurrence in particular is not fully understood.
Patient related characteristics and recurrence
The recurrence rate for grade 2 meningiomas widely varies. It has been reported as low as 4.3%,14 and as high as 69%.15 In our study, 12 patients (16.2%) had evidence of radiological recurrence at mean follow-up period of 40.7 months.
Previous studies have shown that age, male gender, the size of surgical resection, and higher Ki-67 index have an impact on the prognosis of grade 2 meningioma patients.5,16 Other studies have shown that WHO histopathological grade and the extent of surgical resection are considered to be the strongest prognostic factors of recurrence.17
The location distribution of grade 2 meningioma is comparable to grade 1 meningioma,18 with the most common location being in the convexity.19,6 A study by Ruiz et al. demonstrated that convexity location is a protective prognostic factor against recurrence in grade 2 meningiomas.11 In our study, most patients had skull base meningioma (46.6%), followed by convexity (31.5%) and midline meningioma (20.5%), with recurrence rate being 7% in skull base meningioma, 4.1% in convexity meningioma and 5.5% in midline meningiomas with no significant association with recurrence. Generally, larger size tumors are linked with higher recurrence rate.19,16 However, few studies reported that smaller size grade 2 meningiomas are also associated with high recurrence rates.21,6 In this study, the majority of the cases were less than 5 cm3 (71%). Of those, 6 cases had recurrence, with no significant association.
Maximum safe tumor resection and dural attachment remain the treatment goals for meningioma, with complete resection of the tumor being associated with lower recurrence rates in many studies.22,23,16 Few studies have shown no difference in recurrence rate and extent of resection.24 In our study, 58.3% of patients with recurrence had partially resected tumors, with no statistical difference found.
In our study, patients who underwent radiation therapy postoperatively were found to have significantly less recurrence rate compared to those who did not. (p=0.008) Adjuvant radiation therapy has been associated with decreased disease recurrence and progression in higher grades of meningioma in multiple studies.25
Histopathologic features and recurrence
The pathologic subtype of meningiomas mainly determines the prognosis and recurrence rate. Higher atypical features are associated with higher recurrence rates.26 In recent WHO classifications (2016 and beyond), brain invasion has been identified as a standalone criterion for atypical meningioma. Multiple studies have shown that brain invasion increases the risk of a recurrence even when the meningioma exhibits benign characteristics.13,15 In our study, brain invasion was seen in 21.7% of all patients, with one patient experiencing recurrence (p=0.91).
Increased mitotic rate can be seen in up to 70% of grade 2 meningioma papers.2,27 In our study, only 13.4% of meningiomas showed increased mitotic rate. Detecting mitotic figures can be difficult for a variety of reasons, including pyknotic cells and mitotic figure instability during fixation, which results in poor accuracy.2 Studies have shown that increased mitotic activity is associated with recurrence of atypical meningiomas.21,6 In our study, increased mitotic rate was not significantly associated with recurrence.
Increased cellularity, nuclear- cytoplasmic ratio and necrosis are minor atypical features of grade 2 meningioma. Few studies on the significance of each of those factors alone have shown no significant association with recurrence.27 Other studies found that necrosis and sheet like pattern of cells can be associated with higher recurrence rates.28 In our study, no significant association with recurrence was found between each minor criterion and recurrence.
This study is limited by its retrospective design and the collection of pathological features from previously reported pathology results. Inconsistent reporting by the neuro- pathologist might cause some features, especially minor features, to be missing in the final report. Patients labeled as WHO grade 1 meningioma with 1-2 features were not included in this study. Another limitation is the discrepancy in the number of patients in each subtype, however, the number of patients in each subgroup is consistent with the epidemiological distribution of WHO grade 2 meningiomas.4 Only operated patients were included in this study, with a small sample size for the considered pathology. Many patients were not included due to unavailable records or loss of follow-up. The average follow-up time of 40.7 months (median: 27 months) may be insufficient to detect recurrence in a not so aggressive pathology such as meningioma. Larger studies looking at each isolated criterion in meningiomas and its relation to recurrence are needed.
Conclusion
The types of WHO grade 2 meningiomas (atypical, chordoid or clear cell) have similar prognosis and recurrence rates. There is no significant difference between the atypical features in indicating a more aggressive nature or risk of recurrence in grade 2 meningiomas.
Acknowledgement
We would like to thank editage (www.editage.com) for English language editing.
- Received September 11, 2023.
- Accepted December 25, 2023.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.