


Abstract
Ipsilateral hemiparesis is rare after a supratentorial stroke, and the role of reorganization in the motor areas of unaffected hemisphere is important for the rehabilitation of the stroke patients. In this study, we present a patient who had a subclinical remote infarct in the right pons developed ipsilateral hemiparesis and contralateral lower limb paresis caused by a new infarct in the left anterior cerebral artery territory. Our case suggests that the motor areas of the unaffected hemisphere might be reorganized after stroke, which is important for the rehabilitation of stroke patients.
Supratentorial stroke causes hemiparesis on the contralateral side of the body, since corticospinal tracts project predominantly to the contralateral side of the body. Ipsilateral hemiparesis caused by supratentorial stroke is rare, and there are only some case reports, and no population based series were found.1 There are some reasons for the ipsilateral hemiparesis, of which the cortical reorganization within the motor areas of the unaffected hemisphere is important for the rehabilitation of the stroke patients.2 We describe one ipsilateral hemiparesis patient, where cortical reorganization may play an important role in post-stroke recovery.
Case Report
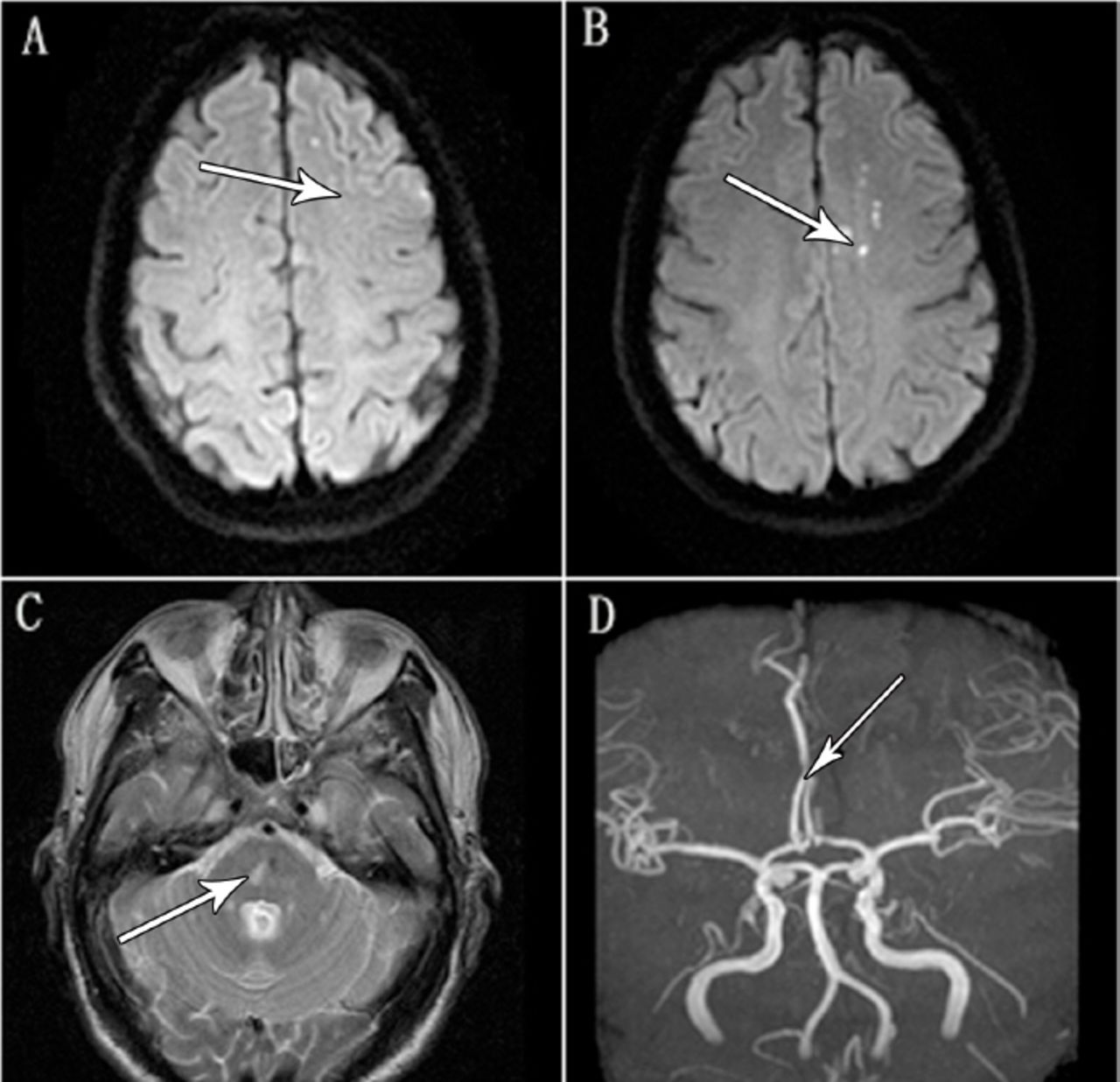
A 58-year-old right-handed man with a history of diabetes mellitus (type 2) and tobacco abuse was admitted to our hospital because of sudden worsening of left-sided hemiparesis and right lower limb paresis. He presented 3 days after the onset of symptoms. He also had difficulty in drinking water and urine incontinence since the onset of the disease. Upon admission, he was alert. His blood pressure was 150/90 mm Hg, and his pulse rate was 80 beats/minute. Neurological examination showed that he had dysarthria and difficulty in drinking water, his left upper limb and left lower limb were graded as 3/5, and his right lower limb were graded as 4/5, using the Medical Research Council of the United Kingdom grading system. He had no weakness with his right upper limb. His left nasolabial fold was shallow, mouth was deviated to the right side, tongue was deviated to the left side when protruded. Left Babinski’s sign is positive, and right Babinski’s sign is negative. Brain MRI and Diffusion weighted imaging showed acute infarction in the left anterior cerebral artery territory (Figure 1A & 1B), there was a remote infarct in the right pons (Figure 1C). Brain MRA showed that there was obstruction of the left anterior cerebral artery (Figure 1D). Cervical computed tomography (CT) angiography showed that there was plaque in the left internal carotid, and the lumen was narrowed mildly (not shown). Cardiogram, dynamic electrocardiogram and 2-D echocardiogram showed unremarkable results. The patient’s weakness improved after 7 days, but not resolved completely. The patient was discharged to a rehabilitation hospital.

Brain MRI and DWI showed A and B) acute infarction in the left anterior cerebral artery territory, C) there was a remote infarct in the right pons, and D) brain MRA showed that there was obstruction of the left anterior cerebral artery. DWI - Diffusion weighted imaging,. MRA-magnetic resonance angiography.
Discussion
Ipsilateral hemiparesis caused by supratentorial stroke is rare, and there are only 10 cases reported up to now.1 Nearly 50% of the patients had remote infarcts previously.1 Almost all the published articles reported the ipsilateral hemiparesis. The summary of these cases is listed in Table 1. However, our case had contralateral lower limb paresis besides the ipsilateral hemiparesis. There are various reasons for the ipsilateral hemiparesis according to the related published articles. Ipsilateral projection from the primary motor cortex is one of the causes.3 It is known that the secondary motor area in the precentral insular cortex innervate the face and the limbs bilaterally, so the lesions that affect the secondary motor area may cause ipsilateral hemiparesis; or cortical reorganization within the motor areas of the unaffected hemisphere after a remote infarct.4 It is reported that some patients may lack the decussation of the pyramidal tracts, which is a congenital anomaly, and these patients may also have other cerebral malformation. Terakawa et al5 reported one patient who was found to have a right basal ganglia hemorrhage on cranial CT and MRI developed sudden onset right hemiparesis. Functional magnetic resonance imaging (fMRI) showed the activation in the motor cortex ipsilateral to the finger movements, but not on the contralateral side. The authors also performed sensory-evoked potentials and found that the cortical response is ipsilateral to the side of stimulation. These results showed that this patient has uncrossed pyramidal tracts, which project ipsilaterally from the primary motor cortex. This patient also had congenital scoliosis. Kang and Choi6 described a patient who was found an acute infarct in the right middle cerebral artery territory developed ipsilateral hemiparesis. Transcranial stimulation of the cerebral motor cortex produced motor-evoked potentials exclusively on the ipsilateral side. This patient also had agenesis of the corpus callosum. These results suggest that the anomalies of the decussation of the cortico-spinal tracts can be found in association with other cerebral anomalies. Ng et al7 reported a left corona radiate infarct patient who developed left motor stroke. They performed the diffusion tensor imaging tractography and found that the uncrossed corticospinal tract could explain the ipsilateral deficit. This patient also had progressive scoliosis. Another possible reason for the ipsilateral hemiparesis is that cortical reorganization within the motor areas of the unaffected hemisphere after a remote infarct.4 Song et al2 reported 2 left corona radiate infarct patients who developed left hemiparesis. Previously, both of the patients had right-sided corona radiata ischemic infarcts and experienced contralateral hemiparesis. fMRI showed that in both of the patients, right-hand movement could activate the left sensorimotor cortex. However, left-hand movement could activate bilateral sensorimotor cortex. It is suggested that functional neuronal reorganization of the left motor areas developed after right corona radiate infarct, and a new infarct in the left corona radiate caused ipsilateral hemiparesis. Ago et al8 reported a similar case, fMRI showed the ipsilateral motor area activation. Etiology of stroke may be helpful for further investigation. There are various etiologic stroke classification systems up to now, the most important goal of which is to obtain some subgroups with distinct phenotypic, therapeutic and prognostic characteristics. The Trial of ORG 10172 in Acute Stroke Treatment (TOAST) system is one example of causative systems. This system is based on clinical features, diagnostic information (CT, MRI), extracranial carotid ultrasonography, and cerebral angiography. In the past 2 decades, the TOAST system is used as the gold standard classification system. The TOAST system includes 5 major subtypes: cardiac embolism, large artery atherosclerosis, small artery occlusion, stroke of another determined cause, and stroke of undetermined cause.10 In the TOAST system, our case is a large artery atherosclerosis patient.
Case summary of ipsilateral hemiparesis after supratentorial stroke.
In our case, the possible reason may be the cortical reorganization. The brain MRI showed that there was a remote infarct in the right pons, which may cause cortical reorganization in the left motor areas. Reorganized left motor areas could at least partly innervate left limbs, and a new left supratentorial infarct caused ipsilateral hemiparesis. The lesions showed by brain MRI in our case did not include the secondary precentral insular cortex. Although we were not able to obtain an fMRI result, our patient had contralateral lower limb paresis, which suggested that the pyramidal tracts crossed to the contralateral side. Our case supports that the motor areas of brain could be reorganized after stroke, which is important for the rehabilitation of stroke patients.
In conclusion, ipsilateral hemiparesis is rare but possible after a supratentorial stroke, and the possible reasons, including the reorganization of the cortical motor areas, are important for the rehabilitation of stroke patients.
Footnotes
Disclosure
This study was funded by Education Project of Zhejiang Province Office (Y201328272) and Medical and Health Science Project of Zhejiang Province (2016KYB096), Hangzhou, China.
- Received September 9, 2015.
- Accepted February 24, 2016.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.