


ABSTRACT
Schwannomas are benign tumors originating from Schwann cells, with seminal vesicle schwannomas being exceedingly rare. This report describes a 54-year-old man with an incidental discovery of a right-sided seminal vesicle mass during a routine ultrasound examination. Further imaging, including MRI and contrast-enhanced CT scans, revealed a well-defined, encapsulated mass with heterogeneous signal intensity suggestive of schwannoma. Histopathological examination confirmed schwannoma, marked by positive S-100 and NSE expression and a Ki67 index of 5%. The patient underwent successful laparoscopic resection without complications and remained asymptomatic for over a month. This case underscores the importance of integrating MRI and histopathological findings to accurately diagnose seminal vesicle schwannomas and guide appropriate surgical management, highlighting the need for increased clinician awareness of this rare tumor.
Schwannoma, also known as neurilemmoma, is a benign tumor of the peripheral nerves composed of Schwann cells. This type of tumor represents the most common benign peripheral nerve tumor in adults and can affect individuals of any age and occur in various parts of the body.1 These tumors are more commonly found in regions such as the head, neck, and mediastinum, whereas their occurrence in the seminal vesicle is exceedingly rare, with fewer than 30 cases reported in the literature.2 This tumor affects individuals in middle to young adulthood and often presents with nonspecific symptoms. Symptoms typically appear only when the tumor has grown significantly enough to compress adjacent organs. Most cases are discovered incidentally during imaging for unrelated conditions, often mimicking other pelvic masses. This rarity of seminal vesicle schwannomas often poses diagnostic challenges due to limited awareness among clinicians and radiologists. In this report, we describe a case of seminal vesicle schwannoma, highlighting unique characteristics identified through magnetic resonance imaging (MRI) and corroborated by histopathological examination of the biopsy specimen.
Case Report
Patient information
A 54-year-old male was incidentally found to have a right-sided seminal vesicle mass by ultrasound during a routine physical examination (Table 1). Subsequent contrast-enhanced computed tomography (CT) scan revealed a lesion at the anterior margin of the right seminal vesicle gland. The patient reported no urinary symptoms and had no significant medical history, including drug allergies, genetic diseases, or psychiatric disorders. Concerned about disease progression, he sought care at our hospital.
- Timeline table.
Clinical findings
Physical examination was unremarkable except for a mildly enlarged prostate with no palpable nodules on digital rectal examination.
Diagnostic assessment
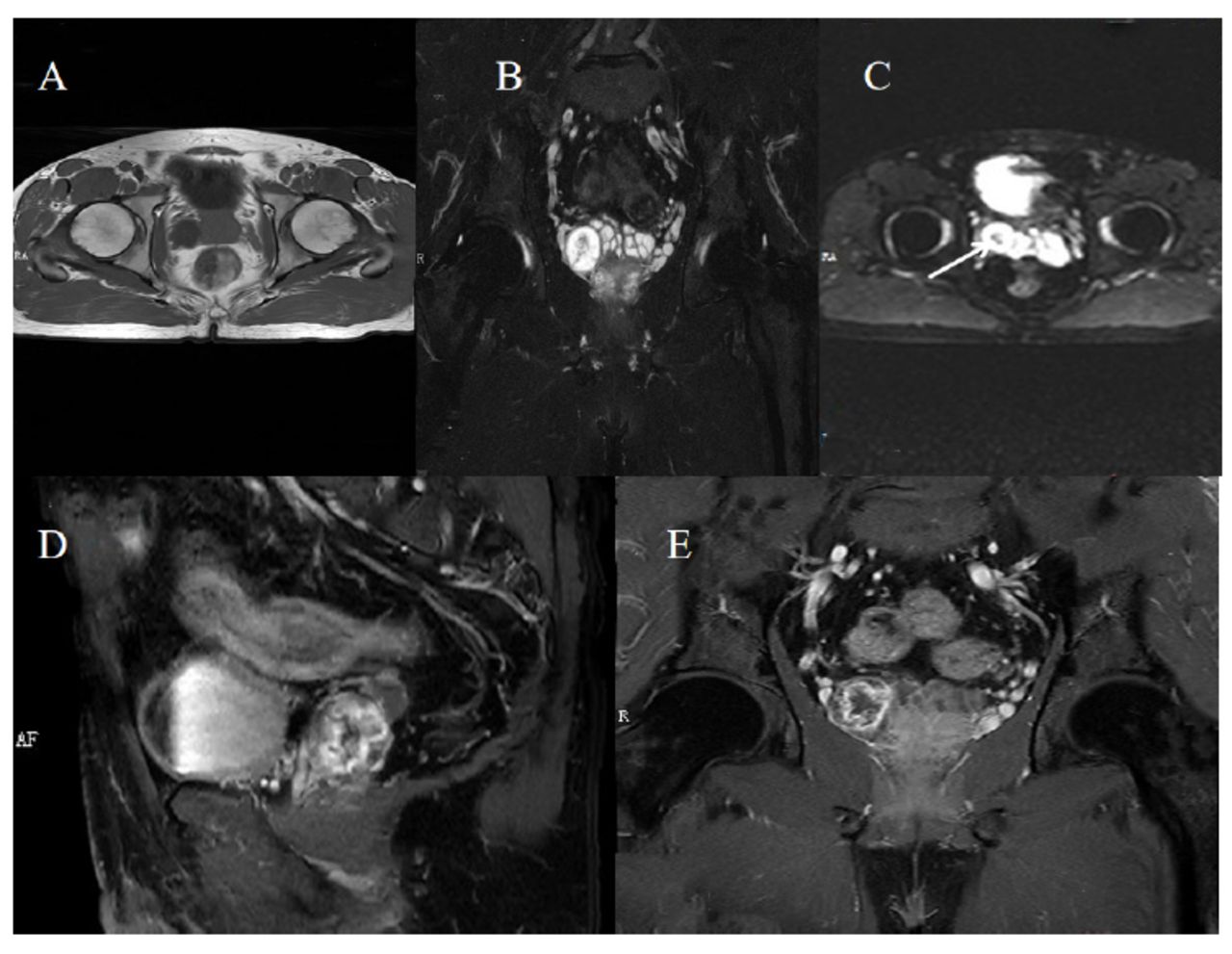
Laboratory tests, including blood biochemistry, complete blood count, and tumor markers, were normal. CT scan revealed a round, low-density nodule in the right seminal vesicle with a heterogeneous internal structure, showing higher central and lower peripheral densities. Contrast-enhanced CT showed progressive lesion enhancement and displacement of nearby venous structures. MRI revealed a round lesion with low signal intensity on T1-weighted images and high peripheral signal intensity with intermediate to low central intensity on T2-weighted, fat-suppressed images, displaying characteristics such as the “entering-and-exiting-nerve sign” and the “fascicular sign” (Figures 1A-B). Diffusion-weighted imaging (b50) showed low signal intensity (Figure 1C). The lesion measured approximately 21 mm × 24 mm and exhibited multifocal linear enhancement suggestive of vascular structures on contrast-enhanced scans (Figures 1D-E), distinct from the prostate gland. The B50 sequence shows intermediate signal intensity in the central area, suggesting hemorrhage.

- Contrast-enhanced MRI scan. A) Pelvic MRI transverse section T1 sequence. B) Coronal T2 sequence shows the linear, sheet-like low signal intensity of nerve fibers. C) The B50 sequence shows low signal intensity in the central area, suggesting hemorrhage. D and E) Contrast-enhanced scans of the T1 sequence show heterogeneous enhancement with intact capsule structure and punctate vascular-like enhancement.
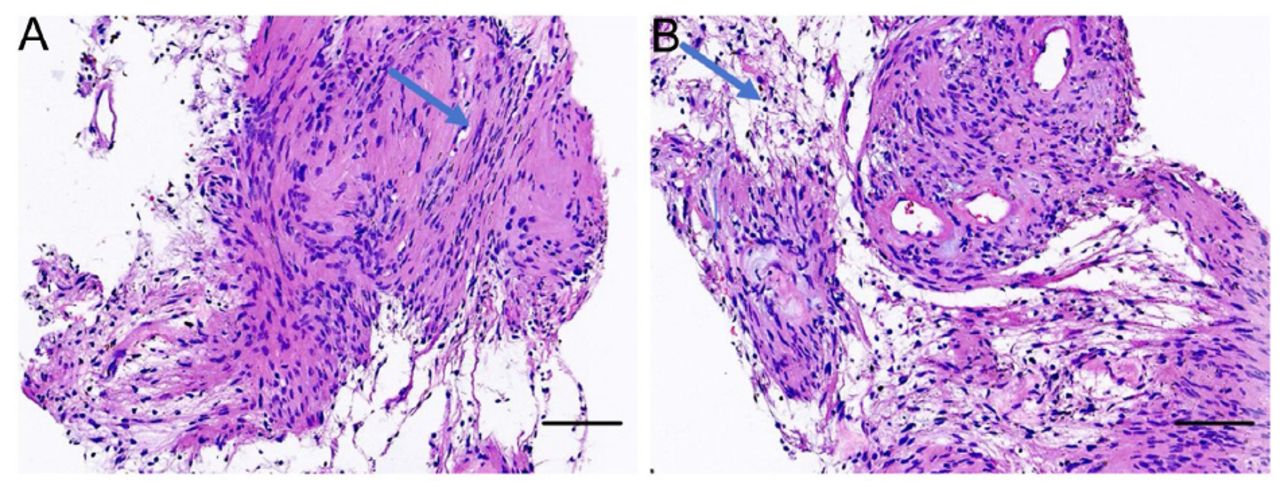
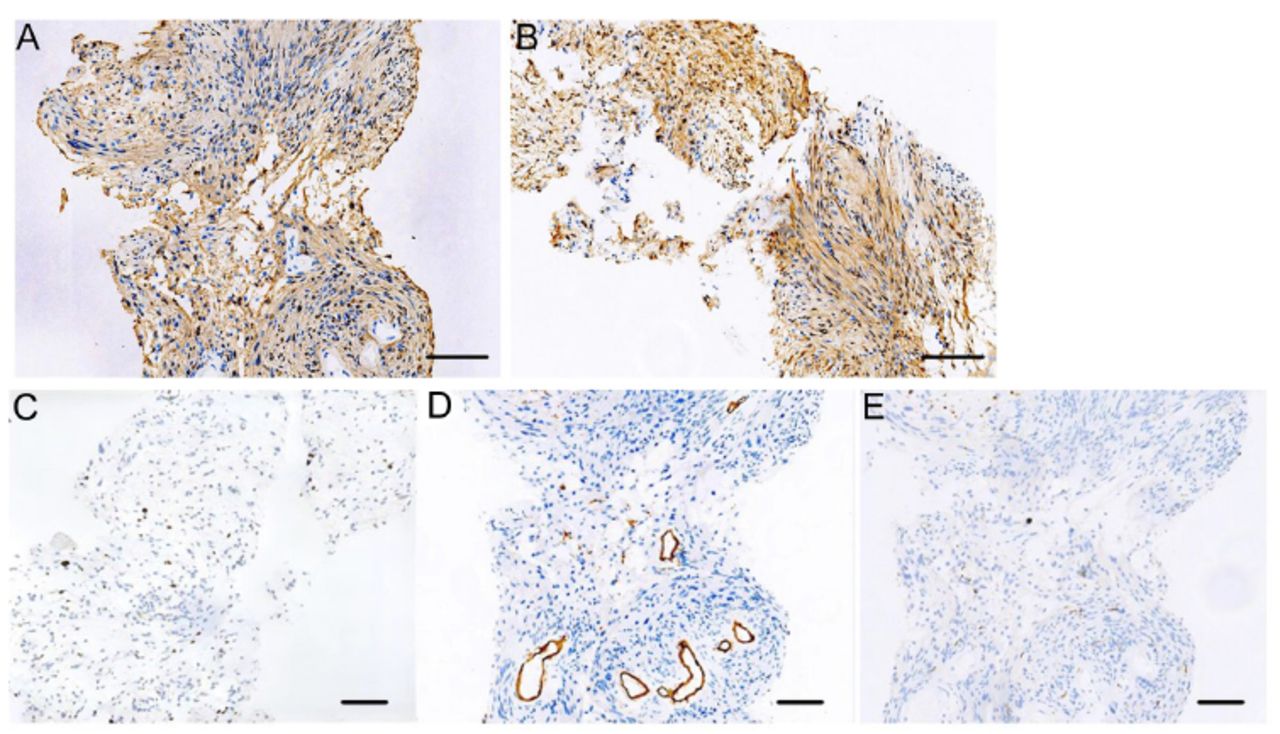
Due to diagnostic uncertainty, a percutaneous biopsy was performed. HE-stained histological examination showed spindle cell proliferation (Figure 2), indicative of a schwannoma characterized by locally active cellular growth. Immunohistochemical analysis of the biopsy specimen demonstrated positive expression of S-100 and NSE, a Ki67 index of 5%, and negative expression for CD34 and Desmin (Figure 3). The patient was comprehensively diagnosed with schwannoma based on the patient’s MRI features, positive S100 and NSE staining, low Ki67 expression, and negative CD34 and Desmin results.

- The HE-stained image of the lesion tissues. Arrows indicate the dense area A) and the sparse area (B). In the dense area, tumor cells were spindle-shaped with indistinct cell boundaries. The nuclei of tumor cells were elongated and arranged in a palisade pattern. The tumor cell nuclei were round and deeply stained in the sparse area, with no significant atypia, and mucinous degeneration was observed in small areas. Additionally, a few fibers and striated muscle tissues were visible in the puncture specimen. Scale bars are 100μm.

- Immunohistochemical staining of the lesion tissues. The images demonstrate strong positive expression of S-100 A) and NSE B), a Ki67 index of 5% C) and a negative expression for CD34 D) and Desmin E) Scale bars are 100 μm.
Therapeutic intervention
The patient underwent laparoscopic resection of the tumor at a tertiary hospital. The surgery was successful, and no complications were observed. Postoperative diagnosis confirmed the presence of schwannoma.
Follow-up and outcomes
The patient remained asymptomatic during a month-long follow-up period, with no signs of recurrence or complications (Table 1).
Discussion
This case of a 54-year-old male with an incidentally discovered right-sided seminal vesicle schwannoma adds valuable insights to the limited body of knowledge. This case underscores that tissue biopsy remains the definitive diagnostic tool, and imaging studies are crucial in diagnosing this condition.
Although pelvic masses are often detected via ultrasound or CT scans, distinguishing schwannoma from other diseases can be challenging, even with contrast-enhanced CT scans. However, MRI enhancement can provide valuable information about tumor size, location, extent, and the presence of specific features. Previous case studies have indicated that seminal vesicle schwannomas typically display progressive enhancement on MRI.3 However, the lesion in this case demonstrated heterogeneous enhancement due to cystic changes. The signal characteristics on the MRI enhancement T1 sequence of schwannomas depend on the proportion, arrangement, and distribution of Antoni A and Antoni B areas rather than their location. In this case, the peripheral area of the lesion showed low signal intensity on T1WI and high signal intensity on T2WI, whereas the central area showed slightly high signal intensity on T1WI and low signal intensity on T2WI. The enhanced scan demonstrated a peripheral/biphasic pattern, with mixed high and low signals within the lesion, indicating a combination of Antoni A and Antoni B areas and partial cystic changes. These imaging characteristics may aid in diagnosis and suggest the presence of a schwannoma.
The differential diagnosis of peripheral nerve sheath tumors in the seminal vesicle region includes seminal vesicle cysts, secondary tumorous lesions of the seminal vesicle gland, and seminal vesicle cystadenoma. Depending on their contents, seminal vesicle cysts can exhibit variable signal intensities on MRI. They typically do not show enhancement with MRI contrast, distinguishing them from schwannomas, which may show heterogeneous enhancement. Secondary tumorous lesions of the seminal vesicle gland, often secondary to prostate cancer, present with loss of the normal structure of the seminal vesicle gland, changes in MRI signal intensity, and an indistinct boundary between the seminal vesicle and the primary prostate lesion. In contrast, the schwannoma, in this case, had well-circumscribed margins. Seminal vesicle cystadenoma presents as a unilateral, multilocular, cystic-solid mass located posterior to the bladder, with a well-defined border. While this can appear similar to a schwannoma on imaging, the histopathological findings of positive S-100 and NSE expression and a low Ki67 index in our case were vital in confirming the diagnosis of schwannoma. Therefore, combining imaging features and histopathological results is crucial in accurately diagnosing seminal vesicle schwannoma and differentiating it from other potential diagnoses.
Comparing this case with previously reported cases highlights essential diagnostic and therapeutic challenges. Our case, like many others, presented with nonspecific symptoms. Previous studies4 also reported incidental findings during routine imaging, underscoring the often asymptomatic nature of these tumors. Advanced imaging techniques, particularly MRI and contrast-enhanced CT scans, played a crucial role in identifying the lesion characteristics in our patients. This is consistent with findings emphasizing the importance of transrectal ultrasound and intraoperative sonography.2 Histopathological confirmation, as demonstrated by positive S-100 and NSE staining in our case, remains the gold standard for diagnosis, aligning with other reports.5 Surgical resection is the preferred treatment for seminal vesicle schwannomas. Our patient underwent successful laparoscopic resection, echoing the minimally invasive approaches reported in the literature.6 These techniques offer favorable outcomes with reduced recovery times. The absence of complications and symptom resolution over a one-month follow-up in our patient underscores the efficacy and safety of laparoscopic surgery for this condition.
Moreover, the intra-tumoral hemorrhage observed in our case of seminal vesicle schwannoma, characterized by a low MRI signal on the b50 sequence and confirmed by hemosiderin deposition, reflects a chronic and stable bleeding process. The case reported by Funston et al. remains the only documented instance of a seminal vesicle schwannoma with intra-tumoral hemorrhage, similar to our case.7 Although their report does not explicitly classify the hemorrhage as chronic, the absence of acute clinical symptoms and the description of a focal hemorrhagic area suggest that it could also represent an old hemorrhage. In contrast, Mandl et al. describe a vestibular schwannoma with repeated hemorrhages of varying ages, as evidenced by mixed MRI signal intensities, reflecting both acute and chronic bleeding.8 This dynamic hemorrhagic behavior necessitated more vigilant management to mitigate potential neurological impacts, unlike the stable hemorrhagic presentation in our case, which allowed for planned surgical intervention. These findings underscore the significance of advanced imaging and histopathological assessment in discerning the nature of hemorrhage, guiding optimal clinical management strategies for schwannomas.
Surgical resection is the primary treatment for seminal vesicle schwannomas, particularly in cases with hemorrhage that leads to mass effect or symptomatic presentations due to the potential for recurrence if not completely excised. Open surgery has been used effectively, but it comes with higher morbidity and longer recovery times, as seen in cases where resection was combined with low anterior resection for rectal cancer.7 Minimally invasive approaches, such as laparoscopic and robotic-assisted surgeries, are highly favored for their reduced postoperative pain, quicker recovery, and lower complication rates. Successful laparoscopic resections have been reported for smaller, well-defined schwannomas, providing precision and safety while minimizing trauma.9 Robotic-assisted surgery offers enhanced dexterity for complex cases, reducing tissue damage and ensuring complete tumor removal.10 In our case, laparoscopic resection was chosen due to the tumor’s characteristics and the presence of chronic hemorrhage, which required careful surgical planning to preserve surrounding structures. This aligns with literature recommendations for complete schwannoma excision to prevent recurrence and manage associated hemorrhage.7 While conservative management may be considered for asymptomatic patients or those with surgical risks, it requires close monitoring for changes in tumor behavior. The minimally invasive nature of laparoscopic surgery, combined with favorable outcomes reported in similar cases, supported its selection in our patient’s management plans.
Conclusion
This case shows the importance of integrating MRI and histopathological findings to accurately diagnose seminal vesicle schwannomas and guide appropriate surgical management, highlighting the need for increased clinician awareness of this rare tumor.
Footnotes
Disclosure. The authors declare no conflicting interests, support or funding from any drug company.
- Received July 9, 2024.
- Accepted November 6, 2024.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.