


Abstract
New-onset psychosis in children represents a complex presenting symptom. Psychosis can be attributable to a combination of factors and etiologies, and all possible causes must be systematically examined. There is growing evidence that a proportion of psychosis/psychiatric manifestations in children may be immune-mediated, and physicians should consider this etiology in each presentation of first-episode psychosis. Immune-mediated encephalopathies/encephalitis are increasingly being recognized in children with antibodies to N-methyl-D-aspartate receptor, Leucine-rich glioma-inactivated 1 or other central nervous system antigens such as Contactin-associated protein-like 2, glutamic acid decarboxylase, alpha-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid or Gamma-aminobutyric acid B. In this study, we describe 3 cases of immune-mediated encephalopathy/encephalitis with prominent psychiatric symptoms at presentation, and suggest a practical diagnostic and treatment approach for children with acute psychosis of an immune-mediated cause.
New-onset psychosis in children represents a complex presenting complaint. Psychosis is defined as the presence of disruptions in thinking, accompanied by delusions or hallucinations, along with an alteration in the thought process.1,2 Psychosis can be attributable to a combination of factors and etiologies, and all possible causes must be systematically examined. The onset of psychosis is an important diagnostic clue. An acute onset occurs more commonly with an underlying medical cause rather than primary psychiatric disorder. Even patients with symptoms suggestive of a primary psychiatric cause should undergo a full evaluation to exclude possible organic etiologies of psychosis,1,4 examples of which are summarized in Table 1. Several immune-mediated causes of acute psychosis are well known, such as neuropsychiatric manifestations associated with systemic lupus erythematosus or post-streptococcal infection, others are newly described.4 Immune-mediated encephalopathies/encephalitis are increasingly being diagnosed in children with antibodies to N-methyl-D-aspartate receptor (NMDAR), Leucine-rich glioma-inactivated 1 (LGI1), Contactin-associated protein-like 2 (CASPR 2), glutamic acid decarboxylase (GAD), alpha-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid (AMPA) or Gamma-aminobutyric acid B (GABAB).4-7 In this study, we describe 3 cases of immune-mediated encephalopathy/encephalitis with prominent psychiatric symptoms at presentation, and suggest a practical diagnostic and treatment approach for children with acute psychosis of an immune-mediated cause.
Common causes of acute onset psychosis in children.
Case Report
Patient 1
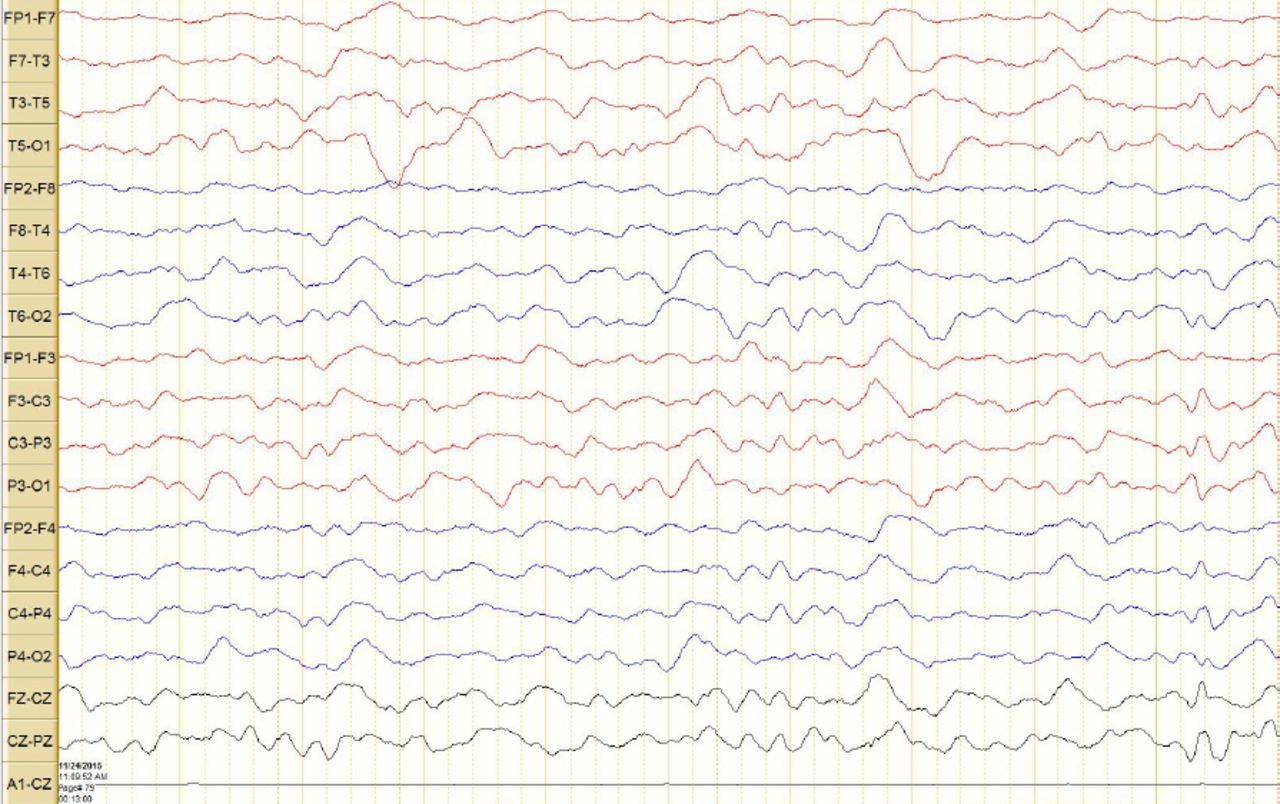
A 3-year-old female who was previously well. She presented with a 5-day history of behavioral change, in the form of incomprehensive talking visual and auditory hallucinations, and short attention span. She had sleep disturbance, labile mood, and decreased appetite with loss of sphincter control. There was no history of recent illness or drug ingestion. One month prior to this episode, she had one attack of unprovoked generalized tonic-clonic brief seizure. Her father had hypothyroidism that was, well controlled on treatment. On physical examination, she was agitated, hemodynamically stable, and afebrile. She had hallucinations and abnormal facial movements, but otherwise there was no neurological deficit. The electroencephalogram (EEG) showed slow background activity (Figure 1). A full work-up including metabolic screening, toxicology screening, brain MRI, cerebrospinal fluid (CSF) analysis, and septic screening were all negative. The antibodies anti-AMDAR, LGI1, CASPR2 and GAD were all negative. Her thyroxine (T4) and thyroid stimulating hormone (TSH) were normal, but thyroid antibodies were elevated: thyroglobulin=383 (normal range< 115 IU/ml), and thyroid peroxidase= 195 (normal range< 34 IU/ml). The working diagnosis was hashimoto thyroiditis, and she was treated with intravenous immunoglobulin (400 mg/kg/day for 5 days). She showed a quick improvement in her condition, and returned to her baseline within 2 weeks. The thyroid antibodies normalized within 3 weeks.

Electroencephalography showing diffuse slow background activity without epileptiform discharges.
Patient 2
A 9-year-old boy presented with a history of behavioral changes associated with aggressiveness and excessive crying for one week. He then started to develop a series of seizures and status epilepticus. On examination, he was encephalopathic, with a Glasgow coma scale of 9/15, hemodynamically stable, and afebrile. There was facial dyskinesia. Results of brain MRI were normal, and CSF showed 24 cells/mm3 normal range <5, mainly mononuclear. The anti-NMDAR antibodies were high in the CSF (1:30; normal range<1:1) and serum (1:160; normal range<1:10). Other work-up including septic work-up, toxicology, and metabolic screening, were negative. He was considered to have anti-NMDAR encephalitis, and treated with intravenous immunoglobulin, steroids, Rituximab, and anti-epileptics. The outcome was good, and he returned to normal within 9 months of treatment.
Patient 3
A 7-year-old girl was referred because of acute psycho-behavioral changes, 2 weeks after febrile illness. She started to be aggressive, and, hyperactive, with associated sleep disturbances. She, also, became more argumentative and stubborn. She lost the ability to control her urine and stool. Peri-oral movements were also observed. There was no history of headache, vomiting or drug ingestion. Her vital signs were within normal limits. A systemic examination including neurological examination was normal. She looked anxious, with aggressive behavior. The MRI brain was normal, as was toxicology and metabolic screening. The EEG showed slow background activity without epileptiform discharges. LGI1 antibodies titers were elevated at 334 pmol/l (N<85). Other antibodies including NMDAR, CASPR2, and GAD were all negative. She was diagnosed with LGI1 antibodies encephalitis and started on intravenous immunoglobulins and pulse methylprednisolone with a good outcome.
Discussion
We describe 3 patients with immune-mediated encephalopathy/encephalitis who presented in the initial phase with predominant psychiatric symptoms. The presenting symptoms included mainly psycho-behavior changes, aggressivity and hallucinations. Immune-mediated encephalopathies/encephalitis are increasingly being recognized in children with antibodies, mainly to NMDAR, but also to LGI1, CASPR2 (previously attributed to voltage- gated potassium channel antibodies complex) or other CNS antigens.5,7 Most of the patients present with a combination of recurrent seizures/status epilepticus, decreased level of consciousness, and motor neurological deficits. Neuropsychiatric manifestations, however, often predominate in the early phases. Such a presentation may cause a crucial delay in diagnosis and institution of immunotherapy. A recent large cohort-based study of patients with immune-mediated encephalitis revealed that 4% of patients presented with isolated psychiatric episodes.8 Support for this paradigm comes from another study involving 43 children with a first episode of acute psychosis. Antibodies to the dopamine D2 receptor were identified in 3 children, and to the NR1 subunit of the NMDAR in 6 children, whereas no such antibodies were found in a group of 43 healthy control children.9 The mechanisms of psychiatric manifestations in antibodies mediated encephalitis are still not clear. The NMDA-receptor blockade in vivo produces schizophrenia-like symptoms in healthy individuals. Ion channel disturbance and hyponatremia have also been described as features of schizophrenia, previously attributed to medication-induced or psychogenic polydipsia.8,9
The findings from this study have several practical implications. There is growing evidence that a proportion of psychosis/psychiatric manifestations in children may be immune-mediated, and psychiatrists should consider this etiology in each presentation of first-episode psychosis. If positive, these patients should be considered for treatment with immunotherapy. On the other hand, several antipsychotic drugs, such as haloperidol, must be used with caution in these conditions, as they have been observed to exacerbate motor symptoms in patients with anti-NMDAR encephalitis. We therefore recommend that all patients with a new-onset psychosis, or neuropsychiatric manifestations including seizures, autonomic dysfunction, movement disorders, or rapid deterioration of the level of consciousness should be evaluated for a possible antibody-associated encephalitis. This assessment should include, as a minimum, a neurological examination and early testing for antibodies against the NMDAR, LGI1, CASPR2, AMPA, GAD, GABAB antibodies, and thyroid antibodies. CSF examination is usually required. The EEG can be useful: and encephalopathic pattern or extreme delta brushes pattern should prompt early referral. MRI of the brain may be normal (although the finding of temporal lobe or limbic system signal changes is very suggestive of an immune-mediated encephalopathy). The aim of these recommendations is the early identification and improved treatment for patients with this disorder.
In conclusion, immune-mediated encephalopathy/encephalitis can present with pure psychiatric features. Autoimmune mechanisms have been recently implicated in a number of neuropsychiatric disorders, classically linked to a pure psychiatric disease. Delay in diagnosis and treatment with immunomodulatory drugs can lead to permanent sequelae. In cases of acute psychosis in children, a multidisciplinary approach to diagnosis and management is needed.
Footnotes
Disclosure
Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received December 6, 2015.
- Accepted January 3, 2016.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.