


Abstract
We report the case of a lady who presented with 3 weeks of visual floaters and optic disc swelling. Subsequent investigations revealed deep white matter changes on brain imaging, and enlarged mediastinal nodes. The presence of anti-CRMP-5 antibodies finally led to the diagnosis of a paraneoplastic syndrome, and mediastinal lymph node biopsy confirmed the diagnosis of small-cell lung cancer. The learning points from this case include that optic neuritis can be the only presenting feature of a paraneoplastic neurological syndrome, and the usefulness of anti-neuronal antibody measurement as a diagnostic marker of an underlying paraneoplastic disease process. The great challenge is to recognise these tumour-associated autoimmune system presentations early, as they often appear long before the primary cancer is evident. Prompt treatment leads to an earlier reduction in circulating auto-antibody possibly due to reduction in tumour size, and thus less likelihood of permanent neuronal damage.
Ocular paraneoplastic syndromes occur when the eye is not directly affected by the tumour or metastasis, but directly by the autoimmune response to onconeural antigens that cross react with antigens in the eye and visual pathway. Our case presented as swollen optic discs, but the underlying problem was small-cell lung carcinoma. It demonstrates that these ocular presentations can occur months before clear symptoms of the underlying malignancy might develop, and so a high index of suspicion might lead to improved prognosis due to earlier diagnosis.
Case Report
Patient information
A 75-year-old Caucasian female was referred to the Medical Ophthalmology Clinic from a neighboring ophthalmology unit with a 3-week history of floaters and progressive visual loss. Her medical history was noteworthy for rheumatoid arthritis (no immunosuppressive treatment) and hypertension. She had a significant smoking history (50 pack years). Systemic enquiry revealed that she had lost approximately 6 kg in weight unintentionally over the preceding month.
Clinical findings
Marked optic nerve head swelling was noted in the presence of vitreous cells. Her visual acuities were 6/60 and 6/24 in her right and left eyes respectively. Neurological examination normal. Steroid therapy in the form of oral prednisolone led to significant improvement. The swelling of her optic nerves significantly reduced as did the vitreous haze. Her vision had improved in her right eye to 6/24 and her vision in her left eye improved to 6/9.
Diagnostic assessment
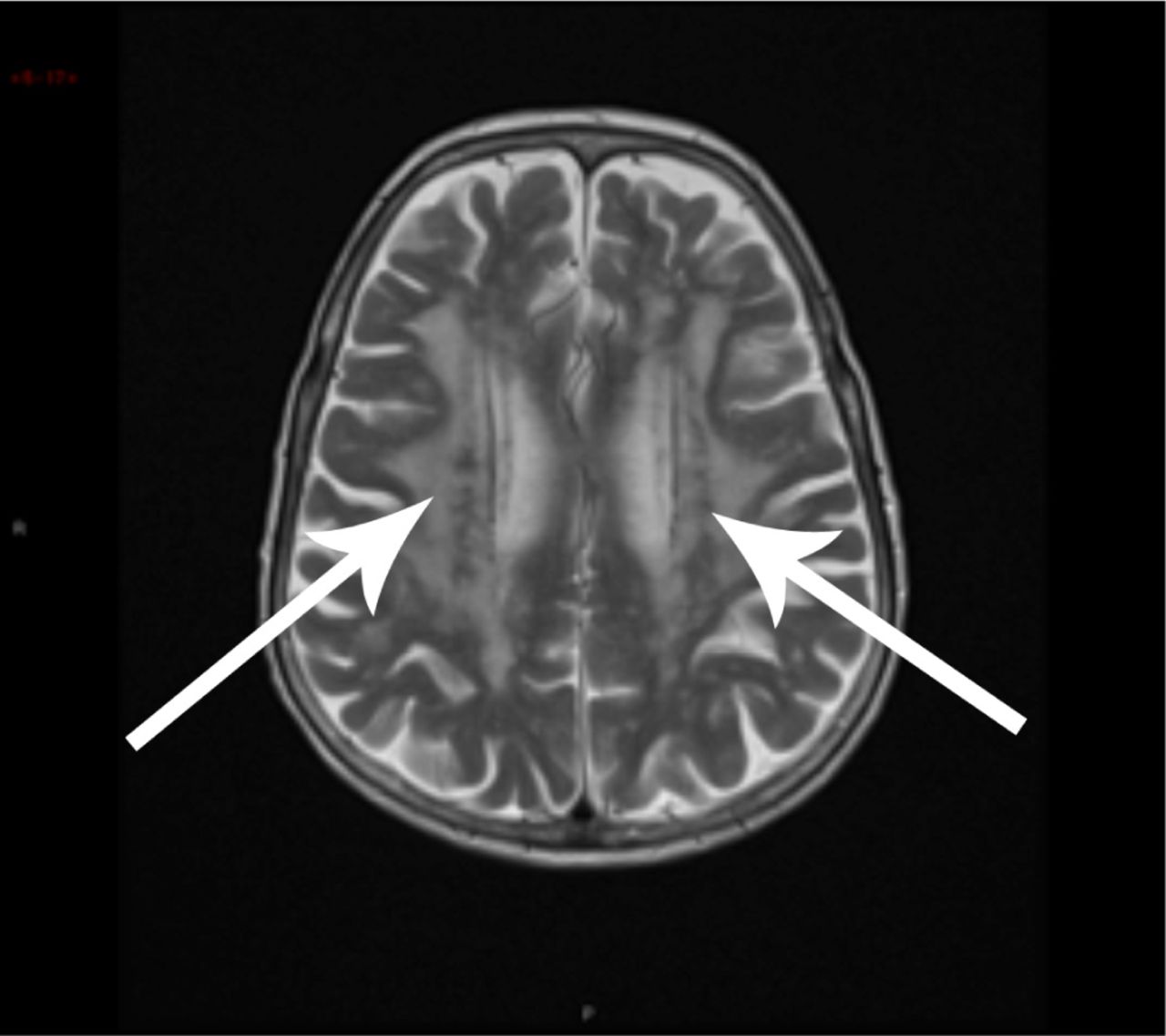
The MRI of head (Figure 1) with contrast showed no evidence of venous thrombosis, no meningeal enhancement or space occupying lesion, but the radiologist questioned whether the white matter lesions that had been noted initially were due to ischaemia. They were not typical of neurosarcoid but lumbar puncture was arranged. Serum ACE was not possible as she already took an ACE inhibitor for hypertension.

MRI head showing bilateral white matter changes.
Lumbar puncture
This showed an opening pressure of 4cm, and a CSF lymphocyte count of 7. There were unmatched oligoclonal bands, and normal cytology. The CT scan of thorax, abdomen and pelvis: no evidence of malignancy.
Bloods
normal CRP, ESR and FBC. Protein electrophoresis- normal.
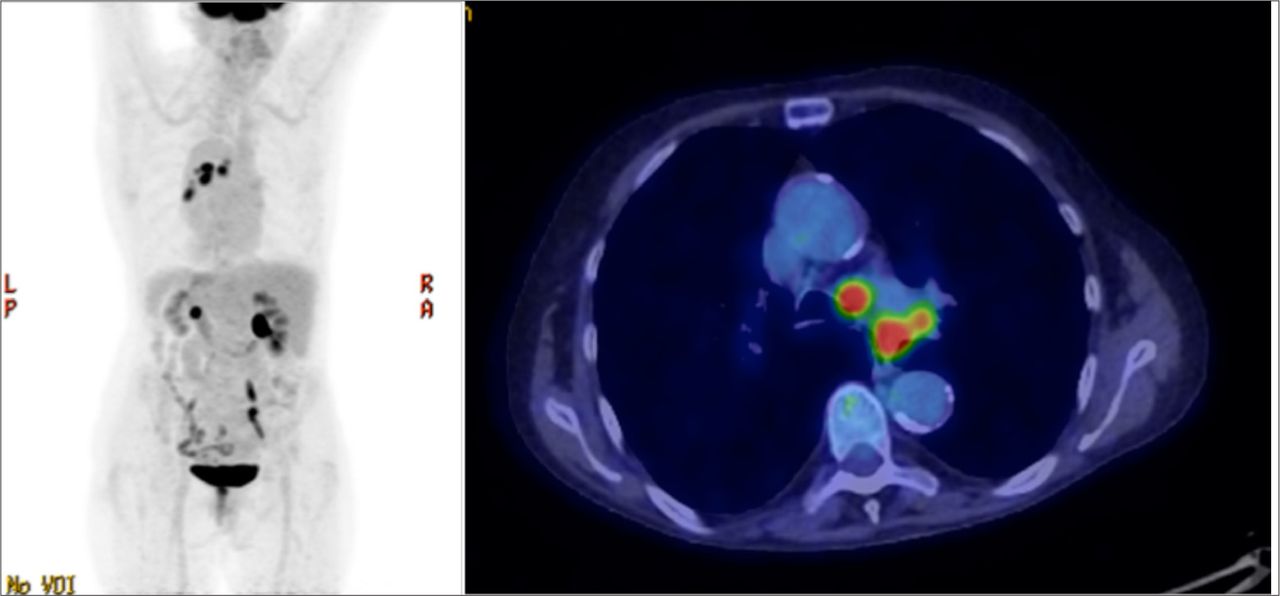
Her blood was also sent for antineuronal antibody serology, and showed that CRMP-5 and SOX-1 paraneoplastic antibodies were positive. Therefore, PET scan was arranged which showed mediastinal and left hilar lymphadenopathy (Figure 2) that the radiologist felt was not typical of lymphoma.

Left hilar and mediastinal lymphadenopathy.
Therapeutic intervention
Her case was discussed with the respiratory and thoracic teams and lymph node sampling by endobronchial ultrasound was organised, and the mediastinal nodes confirmed small cell lung cancer (TXN2M0) as the diagnosis.
Follow up and outcomes
She commenced Etoposide and Carboplatin chemotherapy. Her oral steroids were steadily reduced, and vision improved after chemotherapy began, with her right cataract to be dealt with later. She remains in clinical remission.
Discussion
Collapsin response-mediator protein, in particular CRMP-5, is a neuronal cytoplasmic antigen. Onconeural antibodies against this antigen are seen in tumour cells of small cell lung cancer and thymoma,1 and lead to cross reacting immune-mediated autoimmunity.2 Other auto-antibodies are possibly involved also,3 and in this case anti-Sox-1 was detected.
A wide variety of neurological syndromes have been associated with CRMP-5 antibodies and associated ophthalmic findings described, for example disc swelling and with associated uveitis.4,5 Cross et al6 described the triad of vitreous cells, retinal vessel leakage and optic neuritis linked to anti-CRMP-5 antibodies, and that positive serology could avoid the need for vitreous biopsy.
The great challenge is to recognise these tumour-associated immune system presentations, as they often appear long before the primary cancer is evident.7 It has been shown that early treatment sometimes results in rapid resolution of the ocular symptoms, and prompt treatment leads to an earlier reduction in circulating auto-antibody8 possibly due to reduction in tumour size,9 and thus less likelihood of permanent neuronal damage.
In conclusion, when confronted by patients like this, for example smokers with visual changes and swollen optic discs, then a high index of suspicion might lead to improved prognosis due to earlier diagnosis. Paraneoplastic syndromes should certainly be considered as part of the differential diagnosis and anti-CRMP-5 levels should be measured.
- Received February 20, 2020.
- Accepted June 14, 2020.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.