


Abstract
Objectives: To determine the prevalence of depression and anxiety in adult multiple sclerosis patients attending tertiary facilities in Riyadh, Saudi Arabia.
Methods: This is a cross-sectional study conducted among MS patients in Riyadh City, Saudi Arabia. A self-administered questionnaire was distributed among MS patients at Prince Sultan Military Medical City in Riyadh, Saudi Arabia between April 2020 and January 2021. The questionnaire consisted of socio-demographic characteristics and the Hospital Anxiety and Depression Scale (HADS). Univariate using Chi-square test and multivariate regression analysis had been performed to determine the factors associated with anxiety and depression among MS patients.
Results: A total of 328 MS patients took part in the study. The most prevalent age group was 36–45 years old (38.4%), with over 70% of the participants being females. Anxiety and depression were shown to be prevalent in MS patients at 42.9 percent and 58.8 percent, respectively. According to statistical tests, being less educated and having partial to severe disability was linked to an increased rate of anxiety and depression, whereas being female was more prone to anxiety symptoms but not depression.
Conclusion: Depression was more frequent than anxiety. As a result, while assessing psychiatric diseases in the study group, depression/anxiety may be expected to be more frequent amongst those of greater disability.
Multiple sclerosis (MS) is a central nervous system demyelinating disease caused by an immunological response. Depression and anxiety are more common in patients with multiple sclerosis (PWMS) than in the general population,1-4 which is a well-known phenomenon. However, we believe that these illnesses are under-recognized in PWMS because several MS symptoms overlap with depression and anxiety, making detection more difficult. Fatigue, sleeplessness, anorexia, memory loss, and concentration problems are all common symptoms of depression, MS, or both.5,6 Furthermore, the symptoms of MS might mislead self-report rating scales designed to detect depression and anxiety, resulting in false positives or negatives.5,6 Moreover, depression in PWMS can impair their quality of life (QOL), medication adherence, and compliance, worsening their prognosis.7-9 Suicidal thoughts and attempts are also common.10-13 The hospital Anxiety and Depression Scale is a one-of-a-kind measure for detecting anxiety and depression while taking into account both disorders’ possible confounders, and it has been validated for use in PWMS.6
Depression is a significant mood illness that affects many people. It creates severe symptoms that impact how you feel, think, and handle day-to-day tasks like working, sleeping, and eating.14 In PWMS, the lifetime prevalence of depression in up to 50%,3 compared to 10.8% in the general population.15 The cause of depressive disorders in people with MS is unknown. However, it is assumed to be complex, with psychological, social, and neurological aspects - as well as immunologic and genetic factors - all having a part.16
Furthermore, depression can have a severe impact on these patients’ health by raising the severity of their symptoms and reducing their compliance with therapy and follow-up, both of which have an impact on their medical costs.9 In addition to a decreased quality of life (QOL), cognitive impairment, and an increased risk of suicide, especially when anxiety is present.7,10,11 Furthermore, PWMS have a 10-year lower life expectancy than the general population of the same age.2 Patients, caregivers, and care providers should not underestimate the impact of sadness and anxiety on PWMS. Improved identification, diagnosis, and treatment in medical offices, where people with mood disorders are frequently seen for the first time, can assist to improve these negative outcomes.17 Unfortunately, despite convincing evidence of its high incidence, greater influence on prognosis, and quality of life, depression and anxiety are still underdiagnosed and undertreated.13 The goal of this study is to find out how common depression and anxiety are among adult patients with multiple sclerosis in Riyadh, Saudi Arabia. We’ll also see if there’s a link between Hospital Anxiety and Depression Scale (HADS) score and patients’ demographical, socio-educational, and MS-related characteristics, as well as MS duration, Immunomodulatory type, and EDSS scores.
Methods
Procedure
The adult patients (aged 18 and up) currently being treated at Prince Sultan Military Medical City (n=328) were studied using primary and secondary data. The preliminary data was gathered via a survey, while the secondary data came from a review of the patient’s medical records. As a result, ethical approval #HP-01-R079 was received.
The Hospital Anxiety and Depression Scale (HADS), established by Zigmond and Snaith, was used to assess the anxiety and depression of MS patients.18,19 The Hospital Anxiety and Depression Scale is a 14-item questionnaire developed to test non-psychiatric, medically unwell outpatient populations for depression (7 questions) and anxiety (7 items) disorders. The HADS is a screening tool that does not provide a conclusive diagnosis; rather, it is the first step in a multistage process of identifying people who are at high risk for the disorder and evaluating them through clinical interviews. Each dimension has a possible score range of 0 to 21 points. Anxiety and depression were divided into 2 levels in this study. Patients were classified as anxious/depressed if their score was greater than 8, and not anxious/depressed if their score was less than 8.20,21 Meanwhile, multiple demographic and clinical variables were examined in the medical records, including (1) age, (2) gender, (3) age of onset, (4) duration of MS, (5) marital status, (4) educational level, (5) income in SAR, (6) type of MS, (7) treatment, and (8) degree of disability as measured by the Expanded Disability Status Scale (EDSS score).22 The EDSS score ranges from 0 to 10, with higher numbers indicating more disability.
Analytical statistics
The statistical program for social sciences, version 26 was used to analyze the data (SPSS, Armonk, NY: IBM Corp, USA). Categorical variable is provided as counts and proportions, whereas continuous variable is presented as mean standard deviation (SD) or median with interquartile range (IQR) if appropriate. The Chi-square test was used to investigate the link between anxiety and depression levels and the patients’ socio-demographic variables. The odds ratio and 95 percent confidence interval were also presented for significant results in a regression model to evaluate the significant independent predictor of anxiety and depression. A 0.05 (two-sided) p-value was used to signify statistical significance. The linear association between anxiety and depression scores was also assessed using the pearson correlation coefficient.
Results
This study recruited 328 MS patients. The details of their socio-demographic characteristics were given in Table 1. The most common age group was 36 – 45 years old (38.4%) with females (69.5%) dominating the males (30.5%) and mostly were Saudis (98.8%). Nearly three-quarters were married (74.4%) with approximately 61% were bachelor’s degrees. Furthermore, 72.3% of the subjects were living with multiple members of a family including a child younger than 16 years. With respect to their occupational status, a great proportion of them were civilians (89%) with 36.6% were earning more than 10,000 SAR per month. The most common MS phenotype was relapsing-remitting. In addition, nearly 60% indicated 10 years or less duration of MS.
- Socio-demographic characteristics of MS patients (n=328)
The prevalence of anxiety and depression was given at Table 2. Based on the results, it was found that the mean anxiety score was 7.02 (SD 3.43) with approximately 43% were considered as having anxiety symptoms while 57.1% were normal. With regards to depression, the mean depression score was 8.79 (SD 3.36) and based on the given criteria, nearly 60% were considered as having depressive symptoms and the rest were not depressed (41.2%).
- Anxiety and depression characteristics of sample (n=301)*
When measuring the relationship between the level of anxiety and depression in regards to the socio-demographic characteristics of MS patients, it was found that the prevalence of anxiety was more common among females (p=0.001) but gender differences in depression were similar (p=0.182). It was further observed that educated patients were more associated without the symptoms anxiety (p=0.006) and depression (p=0.022) while higher earner patients were more associated with anxiety (p=0.043). In addition, the disability index was positively related to anxiety (p=0.005) and depression (p=0.030). On the other hand, age group, marital status, number of family members, type of MS, and duration of MS did not show a significant relationship when compared to both anxiety and depression (p>0.05) (Table 3).
- Relationship between the level of anxiety and depression in regards to the socio demographic characteristics of the MS patients (n=301).
A multivariate regression model was subsequently performed based on the significant results presented in cross-tabulation. Accordingly, for anxiety, it can be observed that the odds of having anxiety were twice as higher in females than males (AOR=2.36; 95% CI=1.37 – 4.07; p=0.002). We also noticed that patients with bachelor’s or higher degrees were more associated with a decreased rate of anxiety (AOR=0.51; 95% CI=0.31 – 0.86; p=0.011). Furthermore, we have learned that patients with partial to severe disability were 1.8 times higher to being associated with anxiety (AOR=1.86; 95% CI=1.11– 3.11; p=0.018). On the other hand, for depression, patients with bachelor’s degrees or higher were more associated with a decreased rate of depression (AOR=0.55; 95% CI=0.33 – 0.91; p=0.019) and patients with partial to severe disability were 1.7 fold higher to being associated with depression (AOR=1.74; 95% CI=1.04 – 2.91; p=0.035) (Table 4).
- Multivariate regression analysis to determine the factor associated with anxiety and depression (n=301).
Discussion
The present study is conducted to determine the prevalence of depression and anxiety among MS adult patients living in Riyadh, Saudi Arabia. Based on HADS-D criteria, the findings of this study showed that nearly 60% of the study subjects were identified to have depressive symptoms. Consistently, several papers indicated that depression was more common among MS patients varying from 34% to 89.9%.23-26 Further, the current study also agreed that the depression of MS patients was higher than the general population such as the study carried out by Al Amri et al.,27 where the prevalence of depression among the general public in Saudi Arabia was only 17.1%.
In our study, the prevalence of depression was more common among patients with a disability while it was less among educated patients. This indicates that the greater the disability of the patients was associated with the greater chance of having depression, whereas the higher the level of education was associated with the decreased chance of having depression. A similar result has been reported by Bahatig et al.25 regarding the effect of depression on the overall health status of MS patients. Based on their accounts, the higher prevalence rate of depression was associated with poor health status. They further added that higher depression levels were more prevalent among MS patients who had been divorced, separated, or widowed. However, in this study, the prevalence of depression was similar between unmarried and married, which was consistent with the study carried out by Alsaadi and colleagues.28 Conversely, it is known facts that relapsing-remitting MS was the most common type of MS. Hence, in this study, the prevalence of depression was relatively higher among this group of MS patients (p=0.102).
Anxiety is another factor that greatly affected the MS population. However, unlike depression, the prevalence of anxiety in this study was lower. Based on the given criteria, 42.4% of the MS patients had anxiety symptoms. This result is not consistent with the study of Bahathig et al.25 They used General Anxiety Disorder (GAD-7) questionnaire to measure the anxiety level of MS patients. Based on GAD-7 criteria, moderate to severe anxiety had been detected in 51% of the subjects. In a study conducted in Iran,24 the prevalence of anxiety was even higher, as 73.6% reported anxiety ranging from moderate to severe. On the other hand, Alsaadi et al.28 accounted lower prevalence rate of anxiety as only 20% of the MS patients had a significant anxiety disorder. They further explained that the variability of rates depends on the study methodology since MS clinics, community samples, and health administrative databases are likely to have conflicting rates.
When compared to the general population, it can be noticed that the anxiety of the general public was lower than that of MS patients. For instance, in Saudi Arabia,27 reports indicated that only 10% of the general public detected anxiety symptoms. While according to the literature, the prevalence of anxiety was higher in other Arab countries.29-31 In Iran,32 29.2% identified as having mental disorders with only 4.7% being anxious. Incidentally, in Brazil33 their outcome showed similar results. Accordingly, 45% of the respondents exhibited anxiety symptoms.
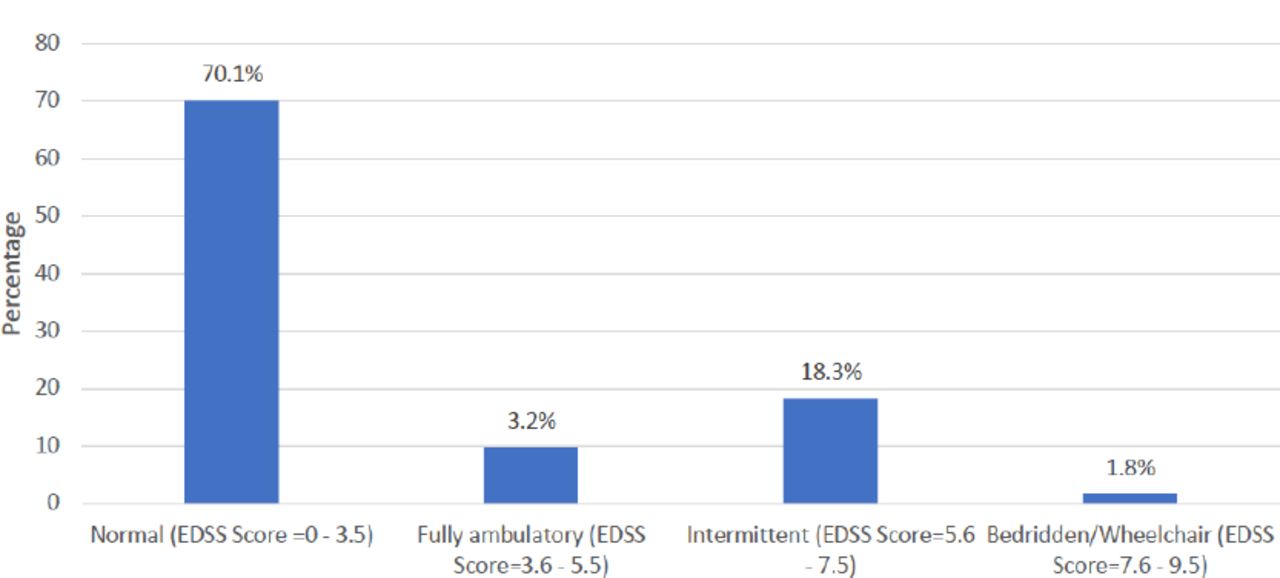
- The EDSS classification. EDSS - Expanded Disability Status Scale
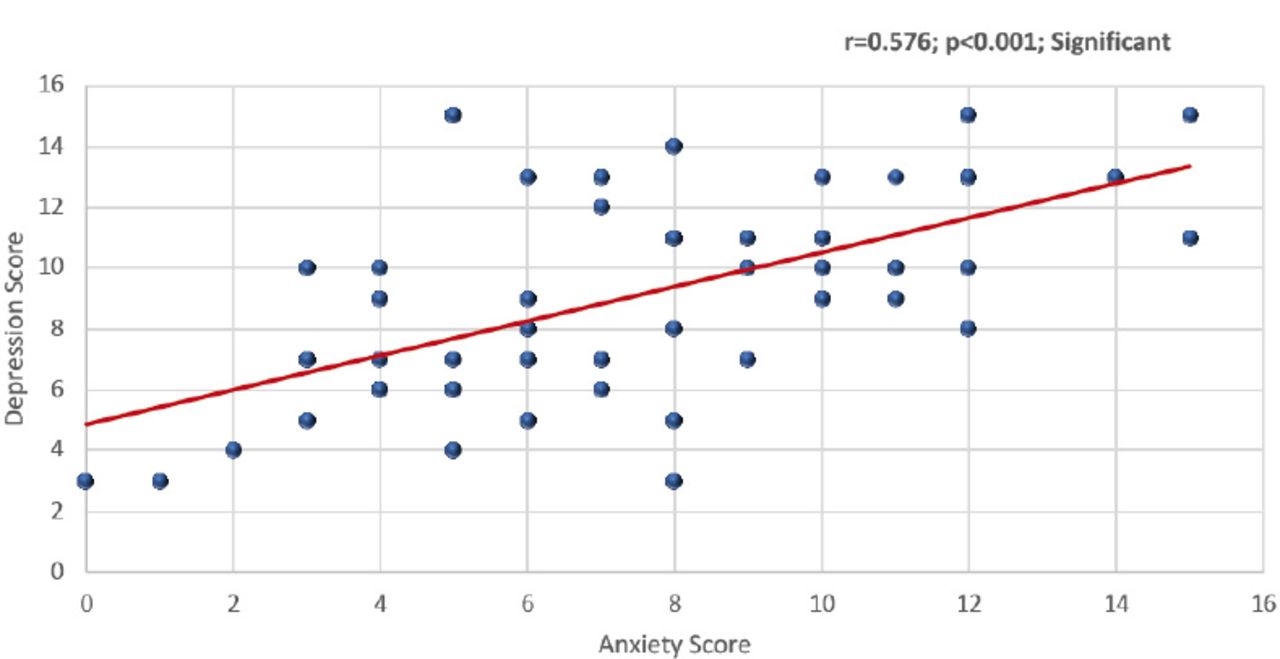
- Correlation (Pearson-r) between anxiety and depression score.
Moreover, we have learned that the prevalence of anxiety varies according to gender and educational level. The outcome of this study predicted that the increased chance of anxiety was more prevalent among female patients with poor physical health status, while patients with better education were less likely to be affected by the anxiety than those less educated patients. In a study by Bahathig and colleagues,25 they documented that the prevalence of anxiety was more common in patients with poor health, which was similar to our results. Conversely, some papers relate anxiety to economic status.34 Given that MS treatment is costly, only patients with an excellent economic situation were less affected by the burden of expensive treatment. Therefore, their mental status is not significantly affected, unlike those with inadequate financial income where every penny is accounted for; these patients are likely to abandon the cost-effective treatment, which could lead to the increase of mental health disorders, including anxiety and depression, resulting to poor quality of life. In our study, however, the prevalence rate of anxiety was not significantly different in monthly income (p=0.083), which was not consistent with the previous results. It may be because the health care system in Saudi Arabia provides comprehensive care for all individuals. It is imperative that patients with poor economic status may seek free treatment from the government to fend off the expensive treatment process of the disease since the treatment itself, hospital visits and rehabilitation are free.
Conclusion
The MS patients were significantly affected by depression, while anxiety was marginal. Patients with disabilities are likely to have a worst-case scenario in evaluating psychiatric disorders among the study population. Furthermore, this study agreed that MS patients are more susceptible to psychiatric disorders than the general population. Therefore, a more systemic psychiatric evaluation is essential to alleviate adverse outcomes among these groups of patients. Moreover, MS patients with deteriorating physical health are more vulnerable to mental disorders. Thus, periodic mental health evaluation is vital. Psychologists and psychiatrists have an important role in improving the quality of life among MS patients.
- Received August 10, 2021.
- Accepted November 17, 2021.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.