


Abstract
A 56-year-old woman experienced persistent excruciating pain with peroneal nerve injury in the anterior aspect of the lower leg after knee surgery. In our pain clinic, we diagnosed the patient with complex regional pain syndrome and performed lumbar sympathetic neurolysis (LSN) with absolute alcohol at the 3rd lumbar vertebra (L3). After the next follow-up, she complained of continuous dull low back pain, anal dysregulation, and fecal incontinence. We performed magnetic resonance imaging (MRI) to rule out other existing pathologies of back pain. On MRI, the nucleus pulposus was moderately extruded to the central zone with inferior sequestration at L2/3, and moderate central canal stenosis was observed at L2/3. She underwent partial laminectomy with discectomy at L2 level. We were not sure of the cause of disc herniation, but we strongly suspected that LSN at the L3 vertebral level was related to the pathology. Therefore, we discuss this unusual case.
Lumbar sympathetic blockade or neurolysis (LSN) is effective for the management of intractable lower-extremity pain.1 However, it is associated with several complications because of the complicated anatomical structures of the spine. Complications include bleeding, infection, impairment of the genitofemoral nerve and spinal nerve roots, and intravascular injection of local anesthetics or chemical agents. Unexpectedly, we observed cauda equina syndrome with an extruded intervertebral disc after LSN. This is a rare case and has not yet been reported in the literature. The intervertebral discs are large and avascular structures, and the cells depend on the diffusion of blood vessels at disc margins for supplying nutrients with oxygen and removing metabolites. Impaired matrix synthesis and breakdown of matrix components may lead to disc degeneration.2 We assumed that lumbar vessels injured by LSN cause vasoconstriction and result in reduced blood supply to the vertebral bodies. This pathophysiology may induce acute intervertebral disc degeneration followed by herniation of the nucleus pulposus.
Here, we describe a rare and disastrous cauda equina syndrome caused by LSN, in terms of its possibility and pathophysiology.
Case Report
Patient information
The patient is 56-year-old female.
Clinical findings
The patient undergone arthroscopic meniscal repair 3 years ago. Postoperatively, peroneal nerve injury developed due to hematoma in the anterior aspect of the lower leg. Subsequently, she developed neuropathic symptoms and signs such as allodynia, hyperalgesia, skin color change, and edema in the left lower extremity. The temperature gradient of each leg was >2°. In the three-phase bone scan, the delayed phase showed hot uptake in the left knee and the proximal tibia. In the electromyogram and nerve conduction velocity examination, peroneal axonotmesis and abnormal spontaneous activities were observed in the left tibialis anterior and extensor digitorum brevis. We diagnosed her with complex regional pain syndrome (CRPS). We repeated the epidural nerve block 3 times at the L4/5 interlaminar space for pain control and central desensitization without any relief. Therefore, we decided to perform lumbar sympathetic neurolysis to attenuate the severe lower leg pain.
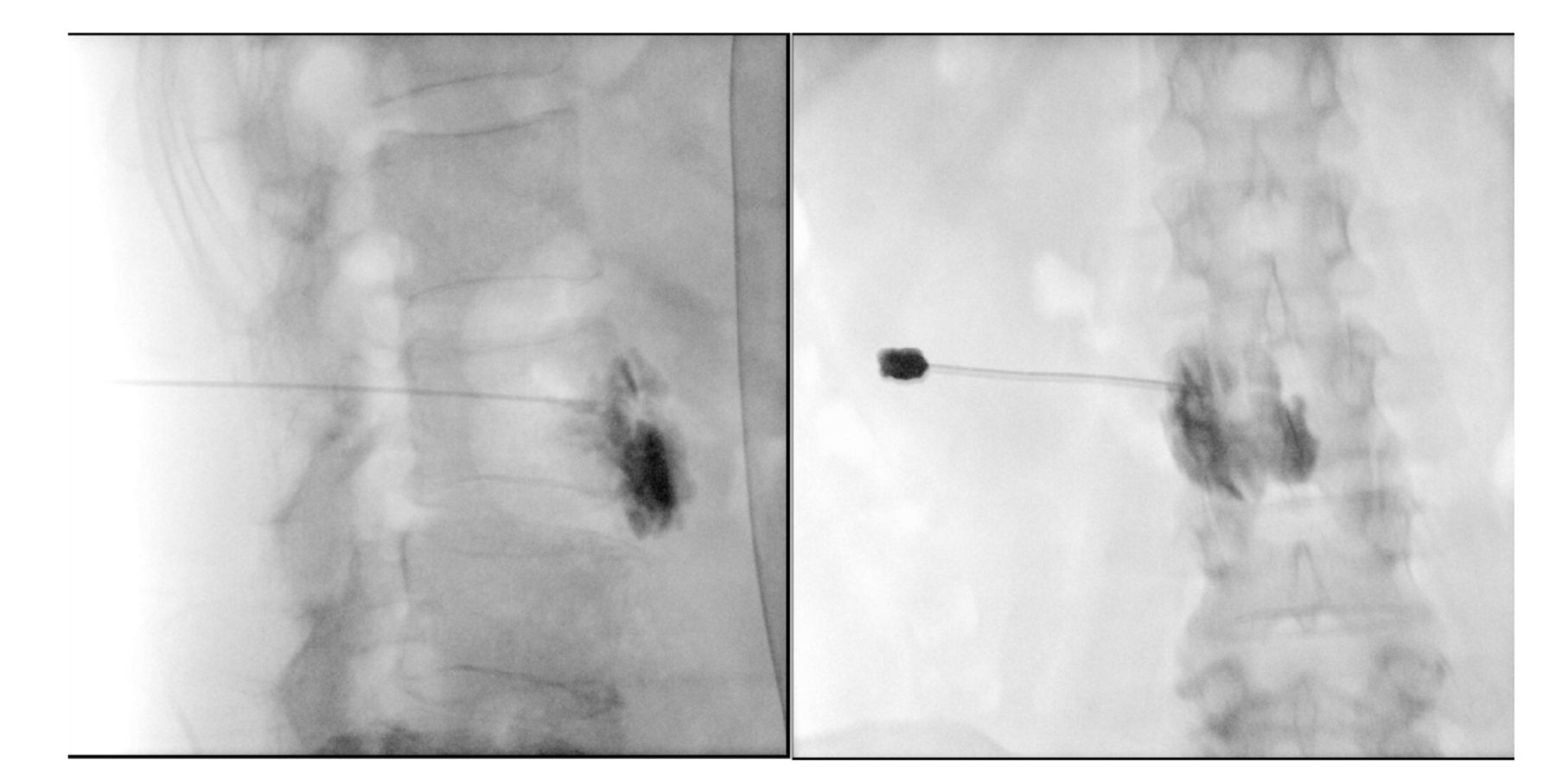
Lumbar sympathetic neurolysis was performed at the 3rd lumbar vertebra. The patient was placed on a radiolucent table. The 16-cm 22-gauge Quincke needle was advanced to reach the anterolateral side of the 3rd lumbar vertebrae. When the tip of the needle touched the side of the vertebral body, it was advanced slowly by scratching the surface bone. In the lateral view, the tip was confirmed to be anterior to the vertebral body (Figure 1). We, after confirmation of non-blood aspiration and spread of contrast medium, administered the pure alcohol (4 mL). The patient did not complain of pain or discomfort during alcohol administration. After the procedure, she experienced left low leg warmth, and her vital signs were stable. One month later, she visited our clinic for follow-up and complained of lower back pain, anal numbness, and fecal incontinence.

- The radiography of lumbar sympathetic block. The needle tip is confirmed to be anterolateral to the vertebral body by injection of contrast medium in the fluoroscopic view. In the lateral and anteroposterior view, the filling defect is observed.
Diagnostic assessment
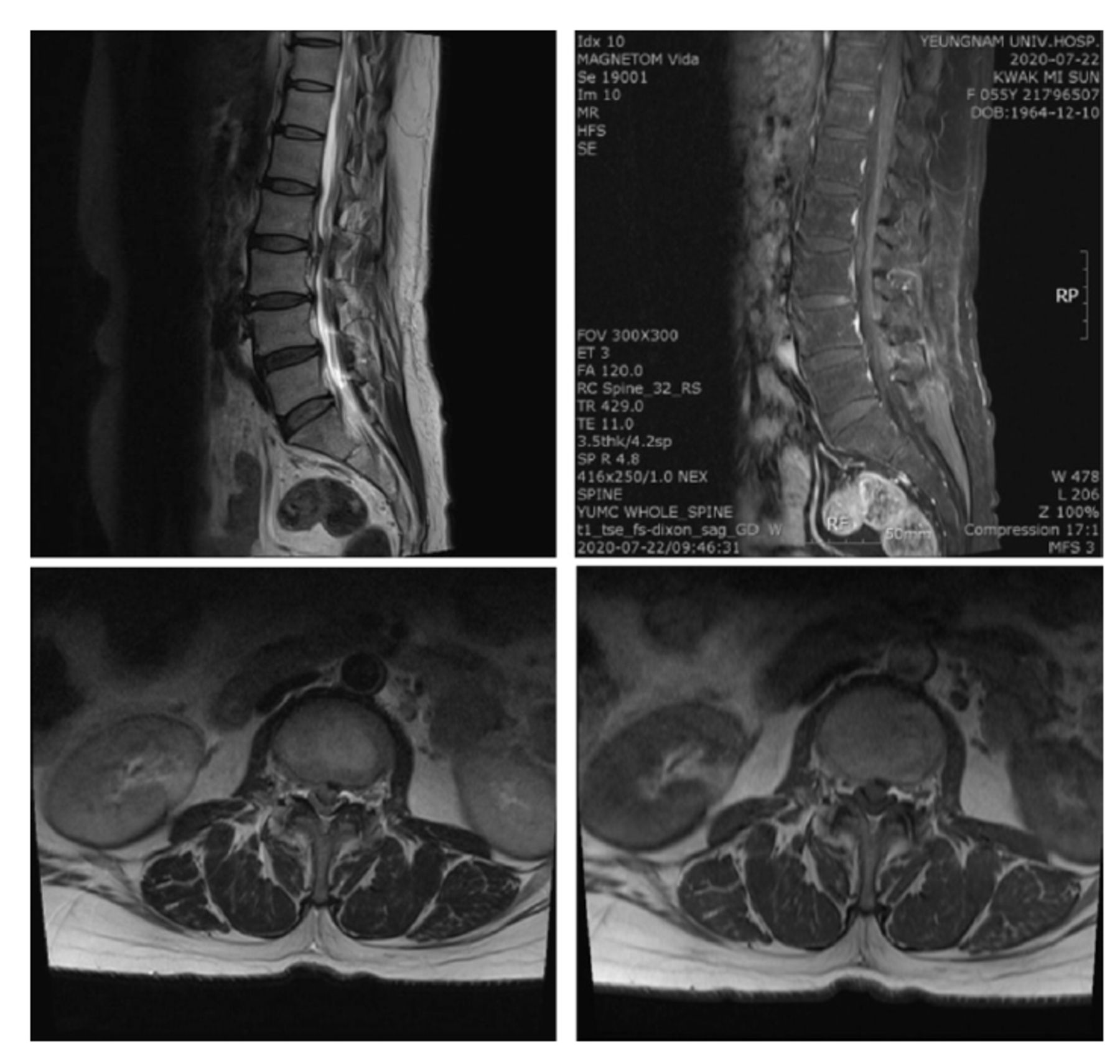
We performed an epidural block at the lumbar spine to relieve the symptoms. However, despite repeated epidural nerve blocks, she experienced continuous low back discomfort, anal numbness, and fecal incontinence. Therefore, we performed lumbar spine magnetic resonance imaging and found moderate disc extrusion to the central zone, with inferior sequestration at L2/3 and moderate central canal stenosis at L2/3 (Figure 2).

- The lumbar MRI of the patient. The findings are moderate disc extrusion to the central zone, with inferior sequestration at L2/3 and moderate central canal stenosis at L2/3 on sagittal T2 and fat suppressed T1-weighted Image with transverse T1 and T2-weighted image.
Therapeutic intervention
The patient has undergone posterior lumbar interbody fusion at L2/3, with L2 partial laminectomy and discectomy (Figure 3).

- The postoperative radiography of lumbar spine. The postoperative state shows posterior lumbar interbody fusion at L2/3, with L2 partial laminectomy and discectomy.
Follow-up and outcomes
The biopsy result of dissected disc materials revealed the degenerative change. The lower back pain and cauda equina symptoms significantly improved. The clinical findings, diagnostic assessment, and interventions are shown in timeline table (Table 1).
- Timeline table.
Discussion
Physicians usually use LSN to manage severe lower extremity pain caused by CRPS. The mechanisms of action of LSN are to attenuate vasomotor activity and block afferent pain signals by disrupting the sympathetic ganglia. The lumbar sympathetic chains are located at the anterolateral site of the vertebral bodies with individual variability. The most common location of lumbar sympathetic chains is at the L2/3 intervertebral level.3 In addition, ganglions are in anatomically complex sites where many blood vessels are present adjacent to them. The inferior vena cava and aorta ran medially over both sides of the vertebral body, respectively. The LSN targets the expected location of the sympathetic chains, which are anatomically located in the fat tissue between the vertebral body, psoas muscle, and aorta or vena cava. Therefore, LSN should be performed under the guidance of imaging, using various equipment such as fluoroscopy, ultrasound, and computed tomography (CT). Fluoroscopy-guided LSN is a popular technique, and ultrasound is a useful device. CT-guided LSN was performed to determine the exact needle position.4
During the procedure, several complications may occur due to needle injury or administration of chemical agents. Complications include bleeding, nerve injury to the genitofemoral nerve and spinal nerve root, infection, and intravascular injection. In addition, necrosis, and stricture of the ureters and pelviureteric junction disruption have been reported as complications of chemical sympatholysis.5,6 Especially, accidental puncture of lumbar segmental vessels and major vessel, such as aorta and vena cava, is always possible due to the complicated anatomy of the needle targeted site. In addition, unintentional intravascular injection into the lumbar vessels may result in toxic or ischemic injury to the spinal cord.
Patient perspective
In our case, intervertebral disc herniation between lumbar vertebrae 2 and 3 developed after LSN, leading to cauda equina syndrome. We considered several possibilities to determine the causal relationship between the LSN and disc herniation. In our procedure, we found that the needle tip was located at the middle third of vertebral body and the filling defect in the lateral view of fluoroscopy. We thought that the filling defect might be due to the localization of fat tissue in the anteroposterior view. However, we assumed that the filling defect might indicate the starting point of a lumbar blood vessel coming out of the great vessel because the lumbar arteries usually pass through the middle third of vertebral body at second and third lumbar level. Therefore, we assumed that the cause of the complications was related to blood vessel damage. If the chemical agent causes vasoconstriction and results in a reduction in the blood supply to vertebral body, it may disturb disc cell metabolism and accelerate disc degenerative changes. We hypothesized that lumbar vessels injured by LSN induce acute intervertebral disc degeneration, followed by herniation of the nucleus pulposus.
Pathophysiology
The intervertebral discs are large and avascular structures, and the cells depend on the diffusion of blood vessels at disc margins for supplying nutrients with oxygen and removing metabolites. The cells are very vulnerable to low oxygen concentrations, poor nutrition, and acidic pH, which results in the matrix synthesis rates falling steeply.2 The impaired matrix synthesis and breakdown of the matrix component may lead to disc degeneration. Therefore, the most important etiologies of intervertebral disc degeneration are the impairments of oxygen and nutritional provision to the cells.7 For example, disc degeneration develops due to atherosclerosis because the oxygen and nutritional provision to the disc cells can be impaired by diminished blood flow to the vertebral column.8,9 It is also reported that disc ischemia is related to abdominal aorta atherosclerosis, stenosing the orifices of vessels feeding the vertebral bodies.10 In this case, it is assumed that the lumbar arteries of L3 were damaged by needle injury or pure alcohol, and as a result, blood supply to the L2/L3 intervertebral disc cell became insufficient due to possible stenotic changes in the injured vessels. Thereafter, degenerative changes of the affected disc structures occur, which are considered to have eventually led to disc herniation in our patient.
In conclusion, the needle pathways during the LSN are better avoided at the midpoint of the vertebral body. The most proper sites for needle tip placement being used for chemical lumbar sympatholysis are the one third of anterolateral aspect in the second or third vertebral body.3 In addition, regardless of an intravascular injection, chemical neurolytic agents have the potential to damage surrounding anatomical structures, including lumbar vessels by direct toxicity or induced ischemic change.
Acknowledgement
We would like to thank Editage for English language editing.
Footnotes
Disclosure. This work was funded by the 2019 Yeungnam University Research Grant, Daegu, Republic of Korea
- Received May 16, 2022.
- Accepted October 12, 2022.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.




{kind=link}
{kind=link}
{kind=link}