


Abstract
Objectives: To assesse the characteristics and validity of the Functional Gait Assessment (FGA). Concussion is a frequent brain injury that affect cognition, balance, and mobility. Prediction of the course of recovery after concussion could be achieved using a multidimensional examination. The FGA has been used to assess balance of individuals with concussion.
Methods: A prospective cross-sectional study was commenced between 2015-2020 in Pittsburgh, PA, USA, including 27 high schoolers with current complaints of concussion and 86 healthy controls. Participants in both groups provided demographics and completed FGA, Gait Disorientation Test (GDT), and Gait Speed (GS) tests.
Results: The FGA test correlated significantly with the GS and GDT. The FGA score in adolescents with concussion was significantly lower than healthy controls (U=1574.5, p=0.004). An FGA score less than 27 indicated a positive concussion injury with a sensitivity of 0.33 and a specificity of 0.92. The FGA showed a diagnostic odds ratio of 5.64. The positive and the negative likelihood ratios were of 3.03 and 0.54, respectively. For adolescents with concussion, the FGA showed no floor effect; however, a small ceiling effect (11.1%) was observed.
Conclusion: The FGA was valid and feasible to assess concussion injuries. It should be noted that a full score on the FGA should not be interpreted as full recovery from a concussion injury.
Concussion (or mild traumatic brain injury) is a frequent brain injury.1 Concussion results in a variety of cognitive and physical symptoms such as headaches, vertigo, balance issues, and visual issues.2,3 The medical community has become more aware of concussions in recent years, and the majority of attention has been on adult injuries.4 According to several studies, however, adolescents are more prone than adults to sustain concussions.5,6 Prior research has shown that cognition, balance, and mobility all suffer after sustaining concussion injuries and do so at varying rates.7,8
Three distinct sensory systems—somatosensory, visual, and vestibular—are integrated to maintain balance, which is a complex task. Normal balancing can be preserved even when one sensory system is disabled. The impact on balance may be more pronounced when more than one sensory system is altered.
A concussion is a multidimensional condition that includes functional, cognitive, emotional, and behavioral impairments. As part of a comprehensive assessment of a concussion, health care practitioners may be better able to predict the path of recovery after a concussion by including a performance test.9,10 In this study, we have focused on the functional aspect of a concussion.
Multiple gait assessment tools are used in neurological cases including the Gait Speed (GS), the Gait Disorientation Test (GDT), and the Functional Gait Assessment (FGA).11 The FGA is a common functional assessment of ambulatory balance that has been used in adults and children with a wide spectrum of disorders and conditions that may hinder balance.12,13 With the increase in awareness of concussion injuries, the FGA has been used more often as a tool to assess balance after concussion as well as to track recovery.14,15
This study aims to determine the reliability of the FGA and to determine the construct validity of the FGA compared to Gait Speed (GS) and Gait Disorientation Test (GDT) in adolescents with concussion. Specifically, our aims were to investigate 1) the FGA concurrent validity with GS and GDT, 2) the FGA known-groups validity, 3) the cutoff score that best discriminates concussed children from healthy controls, and 4) the floor and ceiling effects of FGA in adolescents suffering a concussion.
Methods
This was a cross-sectional study of adolescents suffering from concussion injury and healthy controls. Students with concussion and healthy controls participated in the research. All participants and their parents gave informed consent. The research was authorized by the University of Pittsburgh (IRB approval number: PRO11100023, 2015) and followed the Helsinki Declaration.
The research included 27 adolescents with concussion/mild traumatic brain injury and 86 14- to 17-year-old controls. Inclusion criteria consisted of adolescents with head injuries who sought medical treatment for their concussion. Participants were recruited from a tertiary balance center at the Medical Center of the University of Pittsburgh after completing an extensive neurological evaluation. Healthy participants were recruited from Pittsburgh, PA. The study was commenced between 2015-2020 in Pittsburgh, PA, USA
In a single session, participants provided demographic information and completed FGA, GDT, and GS tests. The FGA is a 10-item performance assessment incorporating stair climbing and walking activities performed under various settings. These activities comprise normal walking, walking while changing the speed, walking with side to side and up-down head rotations, walking with a rapid turn, walking over obstacles, heel to toe walking, walking while shutting eyes, walking backward, and walking up and down stairs. The FGA has a potential range of scores that starts from 0 up to 30, with each activity being scored between 0 and 3 based on certain criteria. Poorer performance is indicated by a lower FGA score.11
In the GS test, the participants were instructed to walk at their own speed in a corridor measuring 10 meters in length. To account for acceleration and deceleration, the timing for the middle 6 meters was recorded. The GS was calculated by dividing the 6-meter fixed distance by the number of seconds required to accomplish the activity.
The GDT is a recently developed gait balancing test that compares the times required to complete a 6-meter walking activity while keeping one’s eyes open and while keeping them closed. The GDT has been shown to be highly discriminatory between those with vestibular impairments and healthy individuals, with a threshold score of 4.5 seconds added to the walking time with the eyes closed providing a clear distinction. A recent study demonstrated that the GDT was capable of differentiating between children who had sustained a concussion injury and those who had not, with an ideal cutoff of a 1.5-second increase during walking with closed eyes.10,16
Statistical methods
The Statistical Package for Social Sciences, IBM SPSS version 24 (SPSS Inc., Chicago, IL, USA) was used to perform all statistical analyses. The Shapiro-Wilk test of the distribution’s normality was used to evaluate the outcomes and choose the best statistical techniques. The relevant statistical techniques were used to provide descriptive data, such as means, medians, and frequencies, with their standard deviations, interquartile ranges (IQRs), and percentages.
The FGA’s convergent validity (comparisons between measures) was assessed using Spearman correlation coefficients to determine the association of the FGA with the GDT and GS.
A Mann-Whitney U test assessed the discriminant validity of the FGA (comparisons of FGA scores between adolescents with and without concussion). The FGA’s discriminative capacity was evaluated using receiver operator characteristic (ROC) analysis. The best discriminant threshold for the FGA was calculated using Youden’s technique.17 The sensitivity and specificity of the FGA test were then calculated using a contingency table produced with the threshold. We calculated the diagnostic odds ratio (DOR), the positive likelihood (LR+) and the negative likelihood ratios (LR-).
The floor and ceiling effects of FGA scores were assessed by reporting the percentage of participants scoring the highest possible (ceiling effect) or the lowest possible (floor effect) score.
Results
The participants comprised 27 adolescents (70% female) between 14 and 17 years of age (mean age 15.5±1.1 years) who were seeking medical services for their concussion injury, and 86 healthy high school children (50% female) between 14 and 17 years of age (mean age 15.5±0.9 years) were recruited. Groups showed no statistically significant differences in gender, age, weight, height, or body mass index (p>0.05). However, participants with a concussion walked slower and had higher (worse) scores on GDT than healthy controls (p<0.05) (Table 1).
- Characteristics of the participants and group comparisons.
Convergent validity
For adolescents with concussion, the FGA correlated significantly with the GS, with a Spearman’s coefficient of correlation of 0.719 (p<0.001). Furthermore, the FGA correlated significantly with the GDT with a Spearman’s coefficient of correlation of -0.472 (p=0.017). Higher scores on the FGA correlated with faster walking speed in adolescents with concussion. Furthermore, higher scores on the FGA correlated with less time difference on the GDT in adolescents with concussion.
Discriminant validity
The Mann-Whitney U test indicated that the FGA total score in adolescents with concussion was significantly lower (median=28, IQR=3, Range:18–30) than that of healthy controls (median=29, IQR=2, Range:24–30) (U=1574.5, p= 0.004). Table 2 shows group comparisons for the total FGA score and the individual tasks of the FGA.
- Group comparisons on FGA and individual FGA items.
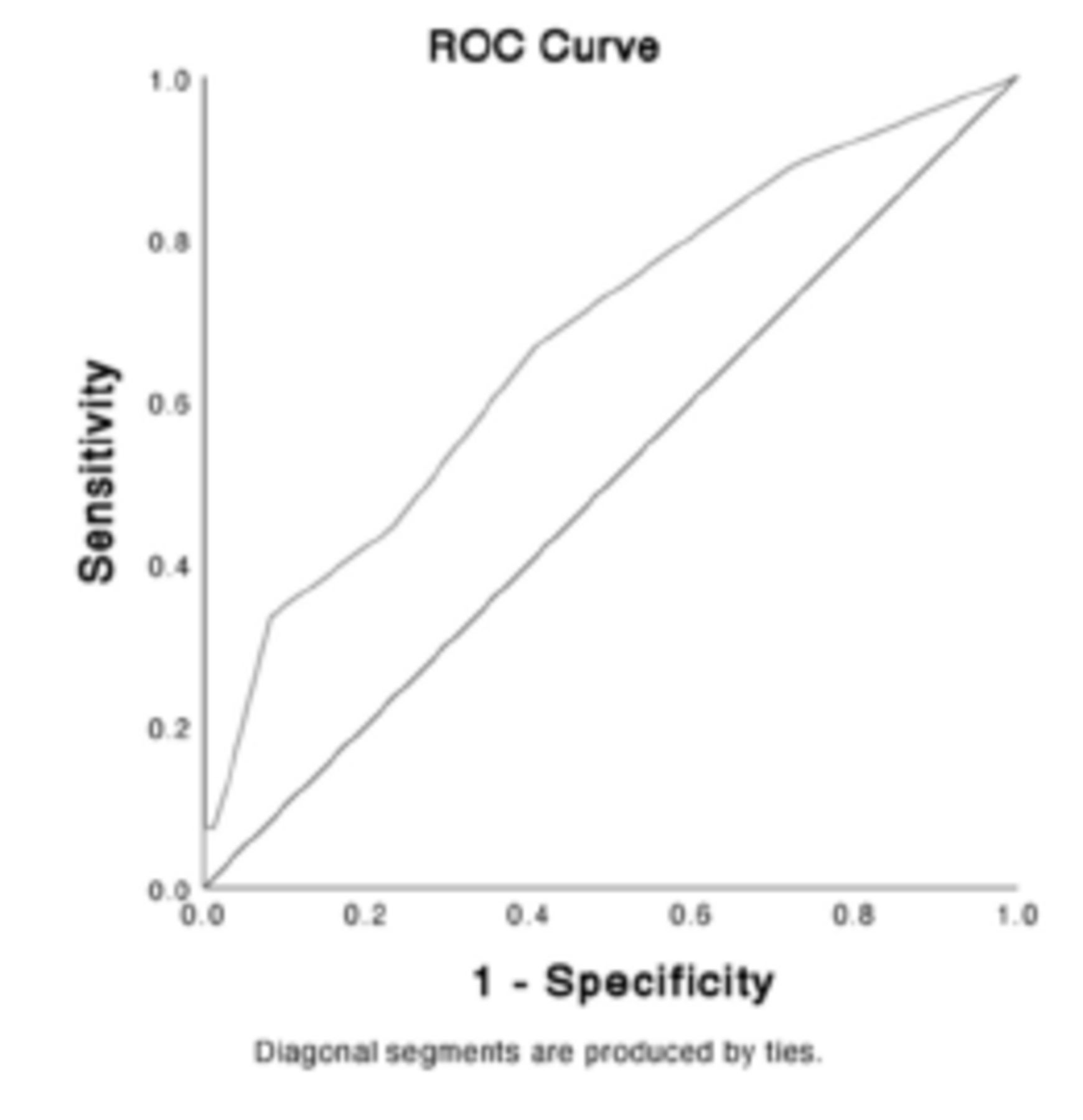
The FGA significantly differentiated the groups, and its discriminant validity was further evaluated using ROC analyses, with AUC=0.678 (0.559–0.779) (Figure 1). Using Youden’s Index, the ideal cutoff score for the FGA to differentiate between the 2 groups was established to be 26 points. With a sensitivity of 0.33 and specificity of 0.92, a score of 26/30 or less indicated a positive concussion injury. The DOR of the FGA was calculated using the contingency table (Table 3) to be 5.64, with an LR– of 0.54, and LR+ of 3.03.
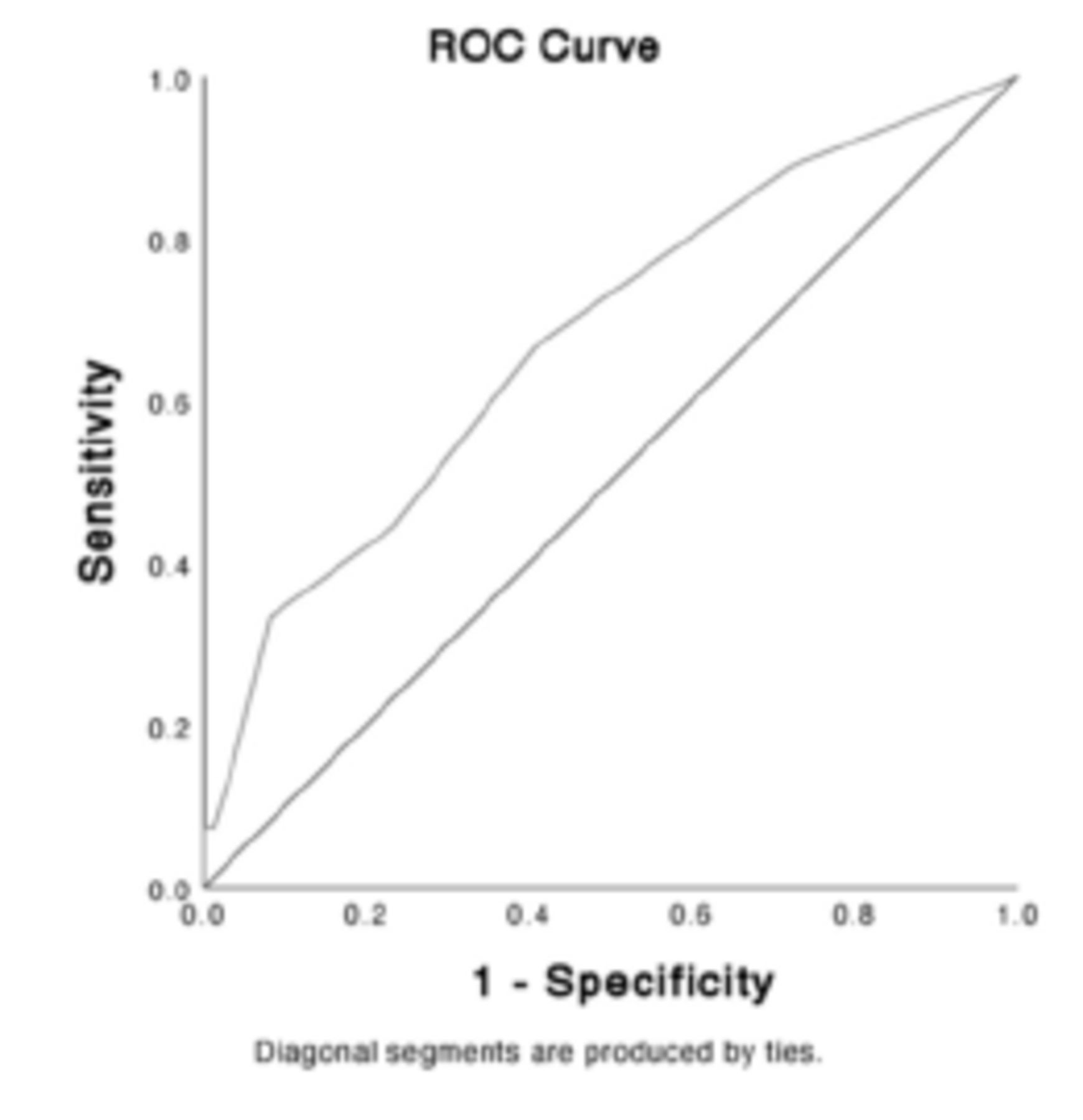
- Receiver operating characteristic (ROC) curve for the FGA score, comparing adolescents with concussion and controls (AUC = 0.678; 95% CI (0.559–0.797); SE = 0.061; p=.005).
- Contingency table.
Floor/ceiling effects
The FGA score showed no floor effect (0%) and a ceiling effect of 11.1%. For the individual items of the FGA, FGA 8 had a floor effect of 7.4%, while all of the other individual FGA items showed no floor effect. Nonetheless, each item on the FGA displayed ceiling effects (Table 4).
- Frequency for floor/ceiling effects of FGA items and FGA total.
Discussion
The FGA is a frequently used functional test that assesses an individual’s ambulatory balance by assessing the quality of 10 standardized ambulatory activities. The primary aim of this study was to compare the validity of the FGA with that of the GS and GDT in adolescents with concussion. Our specific goals were to investigate the FGA’s concurrent validity, known-groups validity, best cutoff score to distinguish concussed adolescents from healthy controls, and floor and ceiling effects.
There were three main findings. First, adolescents with concussion scored less (worse) in the FGA than controls did. Specifically, adolescents with concussion scored less (worse) than controls in 4 of the FGA items: FGA 1, FGA 2, FGA 3, and FGA 9. Second, in participants with concussion, the FGA correlated significantly with GS, showing that better performance on the FGA indicated faster (better performance) walking speed. Third, in participants with concussion, the FGA correlated significantly with the GDT showing that better performance on FGA indicated less change (better performance) in GS between walking with open eyes and closed eyes.
The construct validity of the FGA demonstrated a strong relationship (ρ=0.719) with the GS. This result is similar to a prior study in patients with stroke, which found a strong correlation (ρ=0.879) between the FGA and the GS.18 The FGA demonstrated a moderate negative relationship (ρ=-0.472) to the GDT which was consistent but weaker than that found in adults with and without vestibular hypofunction.16
The FGA differentiated controls from individuals with concussions. The FGA’s capacity to discriminate between controls and individuals with vestibular hypofunction,19 as well as those with Parkinson’s disease20 reported in a previous study, is now enhanced by its capacity to identify those who have suffered a concussion.
In this research, an FGA score of 26 or below distinguished adolescents with concussion from healthy controls. This is above the 22-point cutoff for detecting risk of fall in community-dwelling elderlies21 and the 15-point and 18-point cutoffs for identifying fall risk in Parkinson’s disease patients.20
The FGA revealed no floor effect and only a minor ceiling effect. This finding is consistent with the ceiling effects of the FGA reported in Parkinson’s disease patients, stroke patients, and community-dwelling older adults.22,23 Despite the fact that only 3 of the 27 participants received the maximum score, more than half (15 of the 27 participants) received a score of 27/30 or higher, indicating that the FGA was an easy test for this population. When we looked at the individual items of the FGA, the ceiling effect was more pronounced, with items reaching a maximum score in 59% to 96% of participants.
Study limitations
The study sample was drawn from a highly specialized concussion center and likely included patients not commonly seen in other clinical settings. The study covered a wide range of times since concussion injury; focusing on subcategories of participants, such as those with an acute or chronic injury, will provide more insight into the validity of the FGA in patients with concussion.
Conclusion
To summarize, the FGA is a valid and feasible test for assessing a concussion injury. It should be noted, however, that a full score on the FGA should not be interpreted as a complete recovery from a concussion.
Acknowledgment
The author would like to thank the Deanship of Scientific Research at Majmaah University for supporting this work under Project Number (R-2023-482). We would like also to thank SCRIBENDI (www.scribendi.com) for English language editing.
Footnotes
Disclosure. This study was supported by the Deanship of Scientific Research at Majmaah University Project Number (R-2023-482)
- Received December 12, 2022.
- Accepted June 13, 2023.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.