


Abstract
Objectives: To assess outcomes and complications of patients with cerebral venous thrombosis (CVT).
Methods: This multicenter retrospective study was conducted at 2 health care centers in Saudi Arabia and Oman. Adult patients diagnosed with CVT in radiological imaging between 2006 and 2020 were included. Data were collected from medical records and analyzed using the software IBM® SPSS version 22. Neurological disability occurring after CVT was graded according to the modified Rankin scale (mRS).
Results: The study included 103 patients, of which the majority (68%) were female. The mean age was 39.12±12.96 years. Two-thirds of patients received low-molecular-weight heparin (LMWH) in acute treatment, while 76% of discharged patients used warfarin. The majority of patients had no or mild neurological disability during follow-up, and 6 patients had an mRS score ≥3, implying significant neurological disability. There were 55 patients (52.3%) who had complications from CVT, including seizures in 17 (16.5%) patients and one mortality. Follow-up imaging of 55 patients showed complete thrombus resolution in 20 patients (36%).
Conclusion: Anticoagulation is the mainstay treatment for CVT patients. Approximately half of patients experience complications. Prospective studies are needed to assess the long-term neurological outcomes in such patients.
Cerebral venous thrombosis (CVT) refers to the development of a blood clot in the venous system of the brain.1 It is a rare cause of cerebral infarction that comprises an estimated 0.5 to 1% of all cases of stroke.2,3 According to a recent meta-analysis, the incidence of CVT is approximately 12 cases per 100,000 people per annum.4 It is seen more frequently in young adults and is 3 times more prevalent in females than males.5
The CVT is diagnosed using radiological imaging, and the most commonly employed diagnostic modality is computed tomography (CT), including CT venography. However, magnetic resonance imaging (MRI) methods, including magnetic resonance venography (MRV), are more sensitive techniques.6 The cornerstone of treatment for patients with CVT is anticoagulation therapy. Algahtani et al reported that prompt initiation of anticoagulation resulted in either total or partial recovery in 87% of their patients with CVT.7 In that study, patients who showed a partial response to anticoagulation with some residual neurological dysfunction had presented late in the course of the disease.7 Several anticoagulant drugs are available, but a recent meta-analysis found that low-molecular-weight heparin (LMWH) is a safe and effective option at the time of the initial diagnosis of CVT.8
Complications of CVT can range from minor bleeding episodes to significant neurological deficits resulting in permanent disability or even death.9 A recent study from Oman evaluated the clinical characteristics and outcomes of patients with CVT. The authors found a higher probability of developing neurological impairment following an episode of CVT, which occurred in 30% of patients at the time of hospital discharge.10 The International Study on Cerebral Vein and Dural Sinus Thrombosis (ICVST) reported that thromboembolic complications can occur after an episode of CVT even if the patient is on anticoagulation. The consequences included recurrent CVT, pulmonary embolism, limb, and pelvic thrombosis.11 Thus, this condition is associated with significant morbidity.
The main objectives of this study were to assess the outcomes and complications of patients with CVT. We assessed the outcomes in terms of neurological disability and the radiological resolution of thrombus according to follow-up observations. We also describe the type of anticoagulation therapy being used by these patients. We anticipate that our findings may guide physicians in the treatment, neurological rehabilitation, and counselling of patients with this uncommon form of cerebrovascular disease.
Methods
This multicenter retrospective study involved 2 hospitals in Saudi Arabia and Oman. We identified adult patients diagnosed with CVT between 2006 and 2020 through the electronic medical records system and reviewed their electronic files. We extracted data regarding patient demographics, radiological features, and outcomes from the files using a structured data collection form. The study included adult patients (≥18 years old) who were diagnosed with CVT based on CT or MRI. We excluded patients if they did not attend the hospital for at least one follow-up visit after hospital discharge.
We used the Modified Rankin Scale (mRS) to assess the degree of disability following an episode of CVT. The Rankin scale was originally formulated in 1957 as a 6-point scale ranging from 0 to 5. Later on, it was updated to include a score of 6 to indicate mortality. We considered a score greater than or equal to 3 as indicating that the patient’s level of independence when performing their daily activities has been significant impacted.12
We assessed the mRS score at the first hospital visit following recovery from CVT. The outcomes assessed included the degree of neurological disability and complications following the occurrence of CVT, such as seizures, bleeding episodes, and mortality. We collected follow-up data from the index of CVT diagnosis until the last encounter date, end of study period, or death. This study commenced after receiving approval from the ethics review committees of participating hospitals in accordance with the principles of Declaration of Helsinki. Due to the retrospective nature of the work, consent forms were not required.
We analyzed the data using the Statistical Package for Social Sciences (IBM® SPSS version 22). We calculated the means and standard deviations for quantitative variables (age). We reported the frequencies and percentages for qualitative variables such as gender, diagnostic modality, follow-up imaging, and complications. For the outcome analysis, we divided patients into 2 groups based on their level of disability: patients with mRS scores of 0 to 2 and patients with mRS scores greater than or equal to 3. We used a chi-squared test to determine the association between radiological findings and patient outcomes. We performed a Cox regression analysis to identify factors predicting poor outcomes in patients with CVT. We considered a p-value of less than 0.05 as statistically significant for all analyses.
Results
We identified 103 patients with CVT during the study period. The mean age of the patients was 39.12±12.96 years, and the majority were female (70 patients, 68%); 33 patients (32%) were male. LMWH was the initial anticoagulant administered to 74 (71.8%) patients, whereas 23 (22.3%) patients received unfractionated heparin (UFH), and data were not available for 6 patients. At the time of discharge from the hospital, the majority of patients switched to warfarin therapy (79 patients, 76.7%). There were 18 (17.5%) patients who continued on LMWH and 6 (5.9%) patients who received direct oral anticoagulants (DOACs), which included rivaroxaban, apixaban, and dabigatran. None of the patients were treated with thrombolytic therapy or thrombectomy. The median treatment time was 11 months.
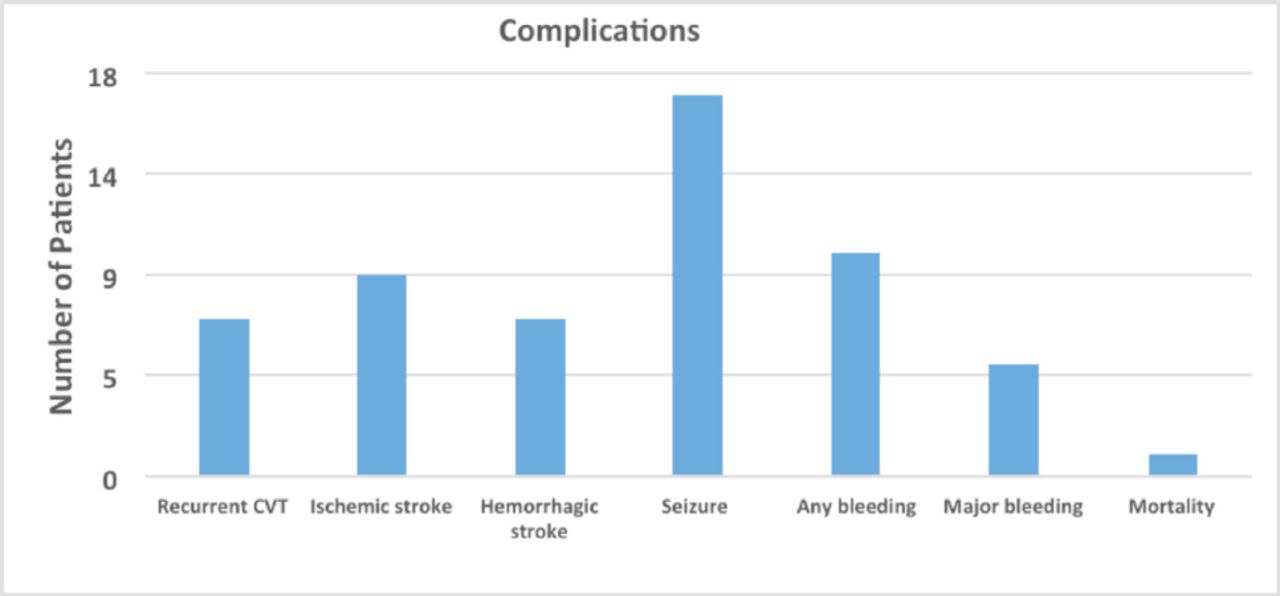
We assessed the mRS for 98 patients during follow-up. There were 92 patients (93.8%) who had mRS scores less than 3, and 6 patients (6.1%) had scores greater than or equal to 3. Table 1 summarizes the clinical and radiological features of patients categorized based on their mRS scores. Overall, 55 patients (53.4%) had complications from CVT during the study period, and Figure 1 shows their frequencies. We performed a Cox regression analysis to assess the clinical and radiological predictors of complications in patients with CVT but identified no statistically significant factors (Table 2).

- Frequency of complications occurring in patients with cerebral venous thrombosis (CVT).
- Comparison of clinical and radiological factors among patients with mRS scores <3 and ≥3.
- Cox regression analysis of factors associated with adverse outcomes (HR: hazard ratio).
We identified 103 patients with CVT during the study period. The mean age of the patients was 39.12±12.96 years, and the majority were female (70 patients, 68%); 33 patients (32%) were male. The LMWH was the initial anticoagulant administered to 74 (71.8%) patients, whereas 23 (22.3%) patients received unfractionated heparin (UFH), and data were not available for 6 patients. At the time of discharge from the hospital, the majority of patients switched to warfarin therapy (79 patients, 76.7%). There were 18 (17.5%) patients who continued on LMWH and 6 (5.9%) patients who received direct oral anticoagulants (DOACs), which included rivaroxaban, apixaban, and dabigatran. None of the patients were treated with thrombolytic therapy or thrombectomy. The median treatment time was 11 months.
We assessed the mRS for 98 patients during follow-up. There were 92 patients (93.8%) who had mRS scores less than 3, and 6 patients (6.1%) had scores greater than or equal to 3. Table 1 summarizes the clinical and radiological features of patients categorized based on their mRS scores. Overall, 55 patients (53.4%) had complications from CVT during the study period, and Figure 1 shows their frequencies. We performed a Cox regression analysis to assess the clinical and radiological predictors of complications in patients with CVT but identified no statistically significant factors (Table 2).
Discussion
This study assessed the outcomes and complications of CVT in adult patients from 2 health care centers in Saudi Arabia and Oman. The study population showed a predominance of female patients. Similarly, a study from Saudi Arabia included 51 patients with CVT, and almost 70% of the patients were female.13 It is possible that this tendency could be due to gender-specific risk factors for CVT among female patients, such as pregnancy and the use of hormonal therapy.14,15
Over 50% of the patients had complications following an episode of CVT, including seizure, bleeding, and recurrent CVT. Residual neurological disability was also seen in a minority of patients (6.1%), but the risk of mortality was low (0.9%). All patients continued taking anticoagulation medication at the time of hospital discharge, and the majority switched from LMWH to warfarin (76.7%). A few continued with LMWH (17.5%), and a minority received DOACs (5.9%). A descriptive study on CVT in an Asian population reported that while 96% of their patients received heparin during the acute episode of CVT, only 68% of the patients continued with anticoagulation at the time of hospital discharge.16 Possible reasons for not continuing anticoagulation included medical conditions, such as pregnancy and recent surgery, as well as practical constraints, such as the unavailability of anticoagulation-monitoring facilities.16
A retrospective analysis of 45 patients with malignancy-associated CVT found that 25% of patients who had not received anticoagulation had recurrent CVT.17 Among those who had received anticoagulation, patients treated with warfarin had a significantly higher rate of bleeding complications than those who were on LMWH.17 In the present study, 93.8% of patients had an mRS score less than 3 during follow-up, indicating good neurological function. This is similar to the findings of Dentali et al, who conducted a large cohort study of 706 patients with CVT in Europe. In that study, 93% of patients had complete or partial recovery of neurological function with mRS scores of <3 at the end of a median follow-up period of 40 months.18
A single mortality occurred during the study period. Similarly, another study from Oman reported a 90% survival rate among patients with CVT.19 Most of the literature, has attributed the low risk of mortality to the availability of accurate diagnostic methods, improved therapeutic modalities, and especially the prompt initiation of anticoagulant drugs.20,21 While the mortality risk was low, around 50% of the patients had complications like seizures and major bleeding episodes. A recent systematic review and meta-analysis assessed risk factors to predict the occurrence of late epileptic seizures in patients with CVT. Involvement of the superior sagittal sinus was one of the risk factors identified.22 Most of our patients had involvement of multiple venous sinuses.
The onset of seizures and hemorrhagic transformation of the infarct caused by CVT are also associated with an increased risk of mortality.23 The VENOST study involved a multicenter assessment of 1144 patients with CVT and also found poor outcomes in patients with CVT following the development of a hemorrhagic infarct.24 However, in our study, we could not identify predictors for poor neurological outcomes (mRs≥3), which could be related to the small number of patients with poor neurological outcomes.
This study provides a comprehensive description of the outcomes and complications of patients with CVT in Saudi Arabia and Oman. However, the retrospective nature is a limitation as some of the patients were lost to follow-up. A prospective multicenter study could verify our findings by assessing neurological disability at multiple time intervals following an episode of CVT. A prospective study design would help to establish the long-term outcomes of CVT and to identify predictors of complications in such patients.
Conclusion
The CVT is a disease that predominantly affects young females. While the risk of mortality is low, other adverse outcomes occurred in over 50% of patients. Prospective studies are needed to ascertain the long-term neurological outcomes of such patients.
Acknowledgement
We would like to thank American manuscript editors (www.americanmanuscripteditors.com) for English language editing.
- Received June 15, 2023.
- Accepted October 17, 2023.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.




{kind=link}