


Abstract
Objectives: To measure and assess the physical activity (PA) of patients with multiple sclerosis (MS) and its association with the quality of life (QoL).
Methods: This cross-sectional study included patients with MS in Kingdom of Saudi Arabia from August, 2022 to November, 2022. Data were collected via social media platforms using a questionnaire that included 3 sections: sociodemographic data, International PA Questionnaire (IPAQ), and the Health Status Questionnaire Short Form-36 (SF-36).
Results: In total, 145 eligible patients with MS were included. The patients’ ages ranged from 18 to 60 years, with a mean age of 33.2±13.9 years. Females were predominantly affected, and most of the patients were either not working or retired. Relapsing-remitting MS constituted the majority (66.2%) of patients. Additionally, most patients (75.9%) were free from co-morbidities. Approximately 41.7% of patients with high PA levels had good QoL scores.
Conclusion: Higher PA levels was significantly associated with better QoL in patients with MS. High PA can improve the QoL by taking into consideration several factors that could influence readiness for exercise and its effect on MS symptoms.
Multiple sclerosis is a chronic, inflammatory, demyelinating disease affecting the central nervous system and the most common non-traumatic neurological cause of disability in young people. The MS first presents commonly between the ages of 20 to 40 years,1 and its outcome differs depending on the site of CNS lesion and the phenotype.2 The clinical presentation of MS can be heterogeneous involving paresis, sensory deficits, visual impairment, weakness, ataxia, and speech disorders, and may be associated with mental and cognitive disorders.3 Knowing the MS phenotype can be helpful in establishing prognosis and implementing an appropriate treatment strategy, only a limited number of which are successful.1,4 Although the etiology of the disease remains unclear, it is believed to be a consequence of interactions between genetic and environmental factors.5-7 In the Kingdom of Saudi Arabia (KSA), the prevalence of MS is estimated to be around 62 patients per 100,000 Saudi nationals, with more females being affected than males (ratio 2:1).8
During the course of this lifelong chronic debilitating condition, which frequently affects young adults during their most productive and active years, there is a significant association between the disease and decreased levels of physical activity.9 Physical activity is a complex behavior affected by different components. Demographic characteristics, including age, gender, marital status, and duration of the disease impact health-promoting behaviors such as physical activity.10 For several patients with MS, fatigue is a major debilitating symptom; thus, patients feel the need to conserve energy due to heat sensitivity. Inactivity may increase the prevalence of co-morbidities or obesity, which has a detrimental impact on the course of MS and can potentially cause functional deterioration and muscle weakening.11,12 Physical activity can reportedly enhance the quality of life (QoL) and cognitive function in patients with MS.13-17 Health benefits of physical activity for patients with MS include decreased risk of coronary heart disease, hypertension, and diabetes mellitus, decreased incidence of depression and anxiety, improved mood, and increased functionality for daily tasks over the course of a lifetime.18 The QoL is defined as an individuals’ view of their situation in life in relation to their objectives, expectations, standards, worries, and culture and value systems as influenced by their physical well-being, social connections, and interactions with key elements of their environment.19 Consequently, patients with MS typically experience lower QoL than the general population as they interact with key elements of their environment. This phenomenon was first described in 2011 and has since been confirmed in several publications.20-22 Their decreased ability to operate in daily life interferes with family relationships, employment opportunities, and social dynamics, which may contribute to the lower QoL.23,24 Numerous disease-related factors, such as impairment level or MS phenotype, and personal factors, such as social support, can influence the well-being of patients with MS. We aimed to assess the physical activity of patients with MS and its association with QoL.
Methods
This cross-sectional study included males and females living in Saudi Arabia who were diagnosed with MS. Exclusion criteria were as follows: 1) individuals with motor disability requiring wheelchair assistance, 2) patients aged <18 years, and 3) those not previously diagnosed with MS. According to the National MS Registry (NMSR), the number of patients with MS in Saudi Arabia is 2313. The majority of the patients (80%) have no or minimal disability, and nearly 1850 of them fit the inclusion criteria. Based on this report, the sample was calculated using OpenEpi (version 3;) (Mini & Nobili, 2017) to be 100 participants, with a confidence level of 95% and a margin of error of 5%. Consent was obtained from all participants. Data were collected using an online questionnaire through social media platforms from August 11, 2022, to November 9, 2022. The Statistical Package for the Social Sciences (SPSS) was used to analyze the data. This study was approved by the institutional review board (IRB) Ethics Committee of King Fahad Medical City in Riyadh, Saudi Arabia, with the approval number of FWA00018774.
The questionnaire involved 3 sections. The first section included age, gender, marital status, place of residence, occupation, weight, height, MS type, special diet, and comorbidities. The second section assessed physical activity using a validated Arabic version of the International Physical Activity Questionnaire (IPAQ); it consisted of 7 questions that measure the intensity of walking and other activities that patients may have performed for the last 7 days.25 According to the scoring system provided by the IPAQ, the activity was categorized as low, moderate, or high activity levels. High activity levels refer to the practice of at least an hour of moderate-intensity activity per day. Moderate activity refers to the practice of half an hour or more of moderate-intensity physical activity on most days. Low activity refers to levels that do not satisfy the criteria of either moderate or high activity levels. The duration of walking, moderate-intensity, and vigorous-intensity activities by minutes and frequency per day were recorded. The recorded minutes and days were multiplied by each other and lastly by the intensity measured in metabolic equivalent of task (MET units); 3.3 MET for walking, 4 MET for moderate activity, and 8 MET for vigorous activity.25 The third section assessed the QoL using a validated Arabic version of The Health Status Questionnaire Short Form-36 (SF-36), which is the most commonly used tools.26 It consists of 8 scales: physical functioning, role limitations–physical, bodily pain, general health, vitality, social functioning, role limitations–emotional, and mental health, with 10, 4, 2, 5, 4, 2, 3, and 5 items, respectively. The combination of the 8 scales will result in 2 core scores, physical and mental, with high scores denoting high QoL.
Data analysis
The data were collected, reviewed and analyzed using Statistical Package for Social Sciences (SPSS; version 21; IBM Company). All statistical methods used were two-tailed, with an alpha level of 0.05, p-value≤0.05 was considered statistically significant. SF-36 was scored using 0-100 for each domain. Overall score <50% was considered poor, 50–75% was considered intermediate, and ≥75% was considered good. Physical activity over the previous 7 days was categorized into low (<600 MET-min/week), moderate (600–1499 MET-min/week), and high (above 1500 MET-min/week) levels. Patient’s bio-demographic data, physical activity, and QoL are presented as frequency distribution and percentage and were descriptively analyzed and plotted. If the frequency distribution was small, the patient’s overall quality physical activity was cross-tabulated by their personal data and other factors using Pearson chi-square test to test for significance and exact probability. Additionally, the relationship between patient’s QoL and their physical activity level was assessed.
Results
A total of 145 eligible patients with MS were included in this study. The patients’ ages ranged from 18 to 60 years, with a mean age of 33.2±13.9 years. Among the 145 patients, 92 (63.4%) were female, 67 (46.2%) were single. Furthermore, 63 (43.4%) were not working/retired and only 13 (9%) carried out fieldwork. Relapsing-emitting MS was observed in 96 (66.2%) patients, primary progressive MS in 29 (20%) patients, and secondary progressive MS in 20 (13.8%) patients. A total of 26 (17.9%) patients followed the dietary system. Among the 145 patients, 14 (9.7%) were obese, and 110 (75.9%) had no co-morbidities (Table 1).
- Bio-demographic data of patients with multiple sclerosis (MS) (n=145).
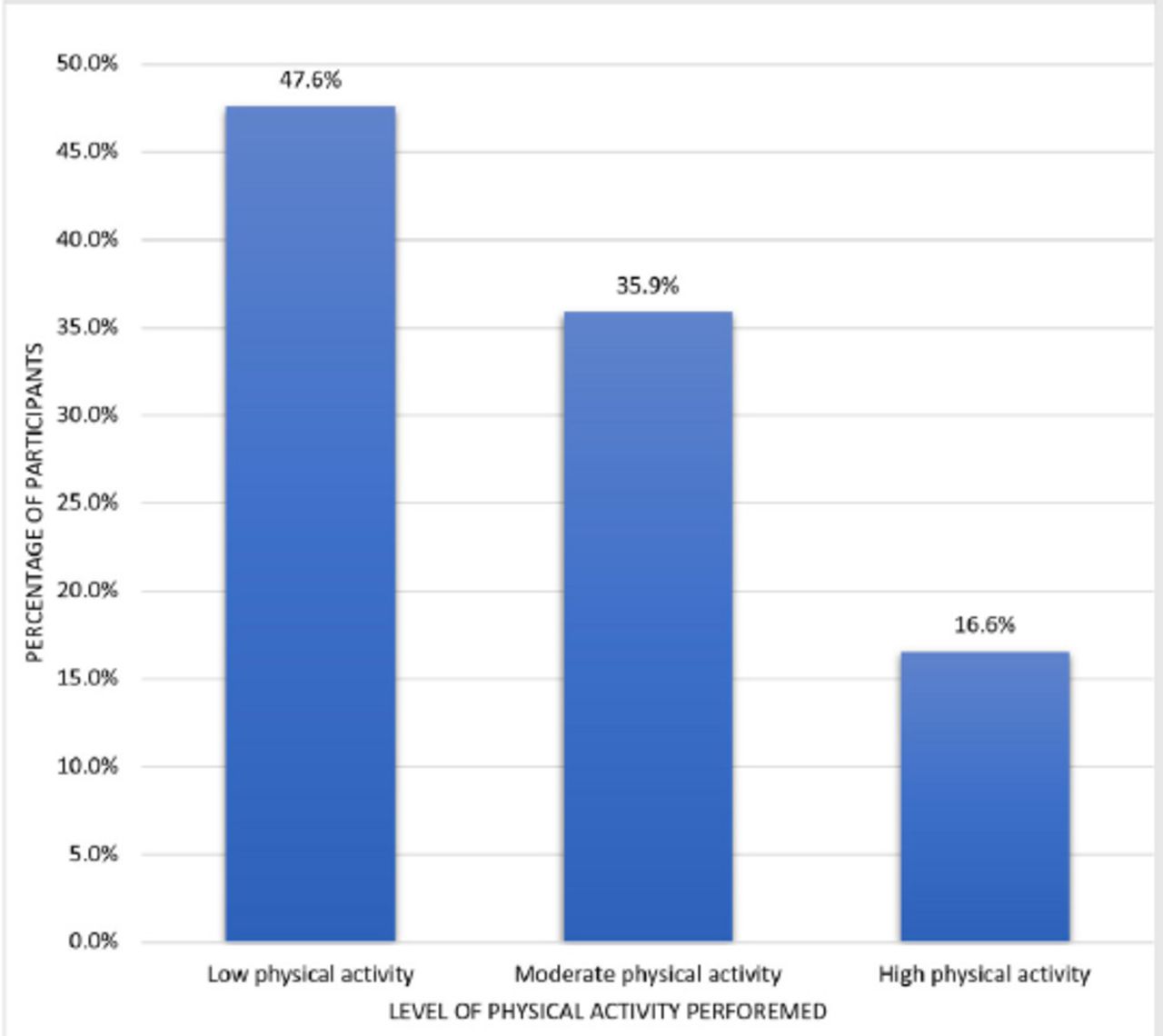
The average number of days of high (vigorous) activity per week was one, ranging from none to 7 days. The average number of days of moderate activity per week was 2, ranging from none to 7 days. The average number of walking days per week was 4, with an average of 15 minutes per day (Table 2). In total, 69 (47.6%) patients performed low levels of physical activity, 52 (35.9%) performed moderate levels, and only 24 (16.6%) performed high levels of physical activity (Figure 1).
- International Physical Activity Questionnaire among MS patients.
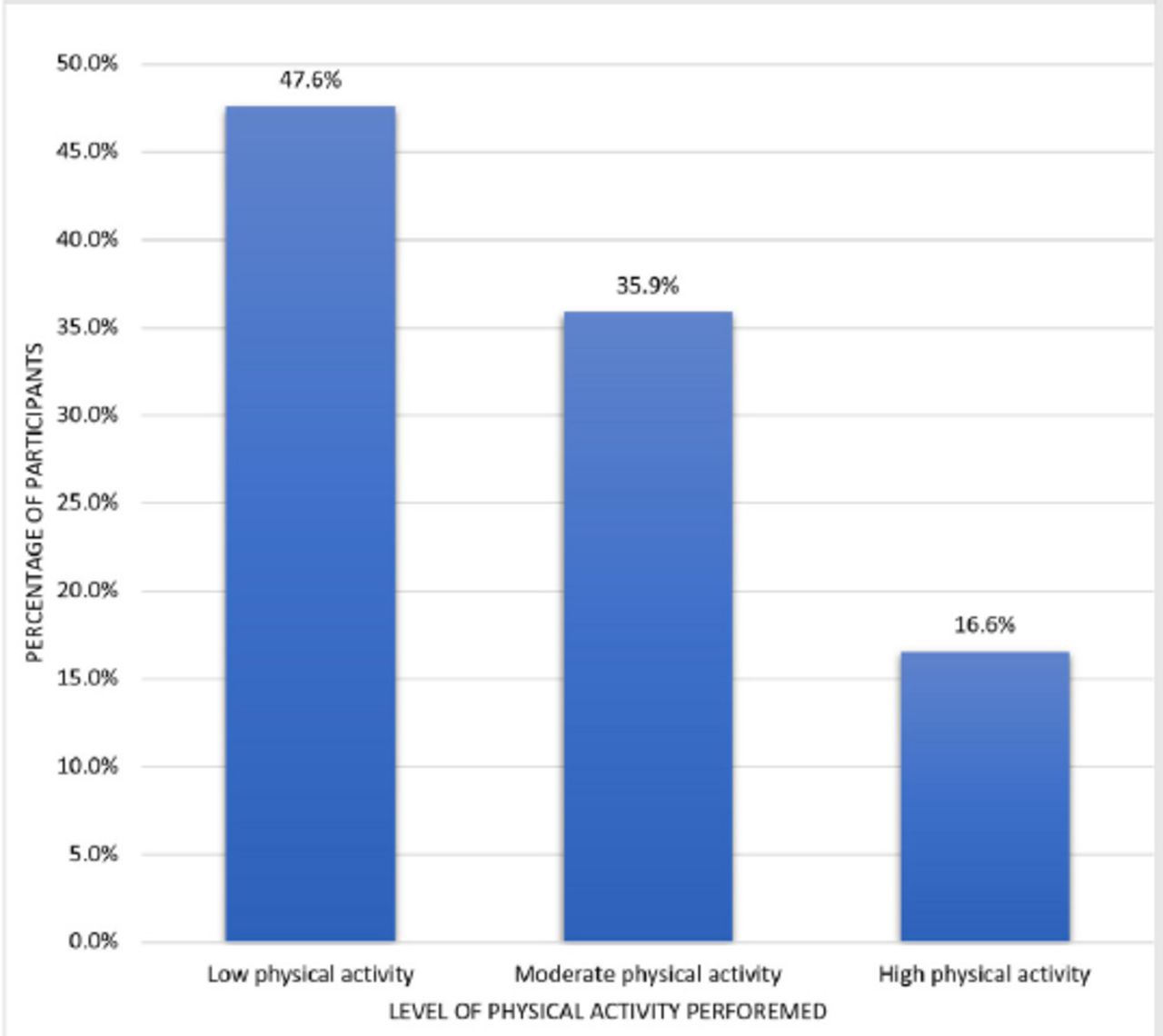
- Level of physical activity among patients with multiple sclerosis in Saudi Arabia
The highest QoL score was observed in physical functioning (73.9±21.9), followed by pain (70.1±25.8), social functioning (68.4±26.0), and emotional well-being (61.8±22.1). The lowest score was for energy/fatigue (55.8±20.6) (Table 3). Of the 145 patients, 45 (31%) had poor QoL, and another 45 (31%) had good QoL.
- SF-36 quality of life score among patients with multiple sclerosis.
After assessing the association between physical activity in patients with MS and their QoL, 41.7% of patients with high PA levels had good QoL compared to 42.3% and 18.8% of those with moderate and low PA levels, respectively (p=.047) (Table 4).
- Association between MS patients’ physical activity and quality of life.
Approximately 30% of patients with secondary progressive MS had high PA, while only 12.5% of those with relapsing-remitting MS had high PA levels. The difference was statistically significant (p=.049). In addition, 26.9% of patients who followed a specific diet, and 14.3% of those who did not, had high PA levels (p=.001). No other factors were significantly associated with the patients’ PA levels (Table 5).
- Factors associated with physical activity level among MS patients.
Discussion
Exercise and physical activity are recommended for patients with MS; however, it is recommended to consider individual variations in disability. Frequently encountered symptoms of MS, including fatigue, weakness, and poor coordination, may make exercise challenging.27,28 Disease-modifying drugs are often associated with considerable side effects.29 Consequently, effective non-pharmacological management with few side effects is under focus; one of the most promising modalities is exercise.30 This is consistent with the recent guidelines, in which exercise prescription is now considered “medicine” for 26 chronic conditions.31
We aimed to assess the physical activity, QoL, and their relationship among patients with MS in Saudi Arabia. The current study showed that nearly half of the study patients had low physical activity, while one-third had moderate levels and less than one-fifth had high levels. The average number of days of vigorous activity per week was 1, while for moderate activity and walking it was two and four days, respectively, for an average of 15 minutes per day. Similar findings were reported by Kalron et al.,32 where 45% patients of MS were classified as physically active, with an increased fear of falling and extra walking difficulties among those who were inactive. In addition, Petajan et al.,33 reported that fatigue is detected in 85% of patients with MS who present with motor and sensory symptoms, reduced mobility, and reduced QoL. Physical activity and recreation are reduced in patients with MS; approximately 78% of patients with MS do not perform any type of physical activity.34 The number of physically inactive patients with MS is not consistent with the assumption that their health and performance will improve if they participate in physical activities.35 Moreover, another study found that among 1064 patients with MS who reported fears of falling, 82.6% reported decreased physical activity.36 In Saudi Arabia, Almarhoon et al37 reported that 39% of patients with MS were highly active physically.
The current study showed that nearly one-third of the study patients had poor QoL, while another one-third had good QoL. The highest QoL score was observed for physical functioning (73.9±21.9), followed by pain (70.1±25.8), social functioning (68.4±26.0), and emotional well-being (61.8±22.1). The lowest score was observed for energy/ fatigue (55.8±20.6). Almarhoon et al.37 reported that the mean physical health score was the highest (78.6), the mean energy score was the lowest (49.4); the mean overall QoL score was 69.5. These finding are similar to those of the current study. A study conducted by the North American Research Committee on Multiple Sclerosis (NARCOMS) assessed five groups of patients with MS; approximately 26% of the participants in the first group had consistently low and stable QoL, compared to 29% and 13% in the second and third groups, respectively. The fourth group (17%) had an early decline, which was followed by an increase to moderate-to-normal QoL. The fifth group (14%) had a normal QoL for 20 years, which subsequently declined.38
Our study showed that higher physical activity was significantly associated with better QoL. These findings are similar to those of Marck et al;39,40 their study showed that increased physical activity leads to significant improvement in the QoL and disability.
The current study had some limitations. First of all, psychological status of the participants was not assessed as it could have a negative impact on the physical activity and QoL of patients with multiple sclerosis. Another limitation was that the extent of motor disability in which participants were excluded was not measured in the current study. We recommend future studies to consider a larger and more diverse sample to assess the extent of disability and provide suitable physical programs.
In conclusion, this study showed that high physical activity was associated with better QoL in patients with MS. However, it was also shown that nearly half MS patients perform low physical activity. Therefore, health practitioners should evaluate the physical activity of their patients in every follow up visit. There is still more to be carried out to find the best exercise strategy for patients with MS, taking in consideration several factors that could influence the readiness for exercise and effect on MS symptoms.
Acknowledgment
We would like to thank Editage (www.editage.com) for English language editing.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received March 20, 2023.
- Accepted August 8, 2023.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
References
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.