


Abstract
Objective: To translate the Falls Efficacy Scale International (FES-I) into Arabic according to the World Health Organization’s criteria and to evaluate the concurrent validity of the FES-I in persons living with balance and vestibular disorders.
Methods: This cross-sectional descriptive study included 43 persons with balance and vestibular disorders presenting to an outpatient dizziness center at King Abdulaziz University Hospital, Riyadh, Kingdom of Saudi Arabia between June 2012 and May 2013. All participants completed the Arabic version of the FES-I and the Dizziness Handicap Inventory (DHI) during their assessment with the clinical audiologist. In addition, subjects completed the Dynamic Gait Index 4-item (DGI-4) gait test. An additional 55 control participants also completed the Arabic FES-I, the DGI-4, and the Arabic DHI.
Results: Forty-three participants with vestibular disorders (36 females, 7 males) with a mean age of 32 years (standard deviation (SD) 10 years, range 18-56 years) and 55 control participants (27 females, 28 males) with a mean age of 33, (SD-12), and age range of 18-78 participated. The correlation between the Arabic FES-I and the Arabic DHI was 0.75 in patients and 0.77 in control participants. The correlation between the Arabic FES-I and the DGI-4 was r=-0.30 (p=0.003).
Conclusion: The Arabic FES-I has established concurrent validity and may be helpful for measuring an individual’s concern of falling in people with vestibular and balance disorders.
Reliable and valid measures to assess persons with balance and vestibular disorders are important to determine change and to objectify the person’s perceived disability. Several balance and vestibular outcome measures have been translated into Arabic for use with adults with balance and vestibular disorders including the Dizziness Handicap Inventory (DHI),1 the Vestibular Activity and Participation measure (VAP),2 and the Dynamic Gait Index (DGI).3 The Bruininks-Oseretsky tool, which is a balance measure used in children, has also been validated in Arabic.4 In a recent report from the National Health and Nutrition Examination Survey in the United States,5 people with reports of dizziness were 12 times more likely to have fallen within the last 12 months. Reports of falling are much higher in persons with bilateral vestibular disorders compared to unilateral hypofunction.6 In post-menopausal women in Saudi Arabia, risk factors for falls were studied but subjects were not questioned regarding vertigo or dizziness.7 The authors noted that a history of falls, age ≥65, walking speed, grip strength, and osteoarthritis of the knee were related to higher numbers of fall incidents in the women studied (n=707).7 Limitations in activities and participation in the community plus negative changes in quality of life have been associated with vestibular disorders.8-11 Difficulty with walking in stores, car travel, walking, and activity avoidance are common in persons with vestibular disorders.12-16 Determining falls efficacy, impairments due to dizziness, and also the ability to ambulate safely in persons with vestibular disorders is important in all cultures. The Falls Efficacy Scale-International (FES-I) was developed for use in various cultures to quantify fear of falling.17 Since 2005, the FES-I has been translated and validated in 6 languages other than English.18-24 Recently, the Dutch short version of the FES-I was used to quantify fear of falling in persons with bilateral vestibular hypofunction.25 The original FES-I was chosen for the study as both the short and longer tests have excellent reliability and validity, but the FES-I is better established. The FES-I shortened version consists of items from the FES-I original.26 In a group of people with balance and vestibular disorders (age range 18-79), the FES-I was shown to be reliable (r=0.94).27 The FES-I is a 16-item tool that asks the patient how concerned they are about falling while performing the 16 different tasks.17,28 Persons rank how they feel regarding performing the tasks with the following: not concerned at all, somewhat concerned, fairly concerned, and very concerned. The FES-I takes little time to complete and contains items that are important to patients such as their ability to clean, shop, reach for objects, and go out to social engagements. The FES- I and the Activities-specific Balance Confidence (ABC) scale scores are related in persons with balance and vestibular disorders.27 The FES-I has not been translated into Arabic. The goal of this study was to determine if the newly translated Arabic version of the FES-I is valid for use in persons with balance and vestibular disorders.
Methods
Subjects
Participants were recruited prospectively during their visit to an audiologist who specializes in the diagnosis and management of persons with balance and vestibular dysfunction. Forty-three participants (36 females, 7 males) with a mean age of 32 years (standard deviation [SD] 10 years, range 18-56 years) provided informed consent that had been approved by the University of Pittsburgh Biomedical Review Board, King Saud University, and King Khalid University Hospital.
Patients were recruited from the ENT Department, King Abdulaziz University Hospital, Riyadh, Saudi Arabia between June 2012 and May 2013. The percentage of patients with various diagnoses included; benign paroxysmal positional vertigo (BPPV) (26%), Meniere’s disease (21%), unspecified dizziness (19%), migraine-related vestibulopathy (12%), vestibular neuronitis (7%), labyrinthitis (7%), anxiety related dizziness (5%), perilymphatic fistula (2%), and head injury (2%).
The inclusion criteria for this study were a complaint of dizziness or balance dysfunction that required an appointment with the audiologist. Participants were excluded if they were unable to ambulate, unable to read and understand Arabic, and if they were less than 18 and or over 85 years of age. Fifty-five control participants (27 females, 28 males) were also recruited in order to compare findings. The control participants had a mean age of 33 years, SD 12 years, and age range of 18-78 years. All controls were free from any vestibular/balance complaints. Any subject with a vestibular or balance issue was excluded from the study. Recruitment was conducted via fliers posted in King Abdulaziz University Hospital as well as by contacting different departments at the hospital inviting staff to come forward to participate. Those who fit the selection criteria were enrolled in the study on a first come first serve basis.
Procedures
Patients were asked to complete the Arabic FES-I and Arabic DHI versions during their first clinical visit. It took approximately 10 minutes to complete the forms. Then, one examiner administered the 4-item DGI, which is a test of ambulation.29
Outcome measures
Both the FES-I and the DHI were forward and backwards translated from English to Arabic and back into English according to the World Health Organizations criteria. Gait was assessed utilizing the DGI-4 item test.29
Falls Efficacy Scale–International
The FES-I is a 16-item questionnaire of fall-related self-efficacy based on the Falls Efficacy Scale (10 items),30 with 6 more difficult new items.31 One rates the FES-I items related to how concerned they are about falling via the following scale: not at all (1), somewhat (2), fairly (3), and very concerned (4) with scores that range between 16 to 64. Higher scores indicate greater concern of falling. In older adults, the test-retest reliability of the FES-I ranged from 0.79 to 0.96.31-33 The validity of the FES-I has been shown in various subject groups and with different outcome measures.31,32,34,35 The FES-I was significantly associated with the ABC scale in persons with vestibular disorders (r=-0.68),35 and has been shown to be responsive.36 The FES-I has recently been utilized with subjects who are younger.
Dizziness Handicap Inventory
The DHI is a 25-item questionnaire that quantifies the impact of dizziness on daily life by evaluating the self-perceived handicap in patients with vestibular disorders.37 Scores on the DHI range from 0-100 with higher scores suggesting greater handicapping effects of dizziness. Higher (worse) scores have also been related to greater reports of falls in people with vestibular dysfunction.37 The DHI loads on 3 different domains: the functional, emotional, and physical aspects of dizziness. The DHI responses are either “yes/sometimes/no” with corresponding scores of “4, 2, or 0” points. Internal consistency for the total DHI score (α=0.89) was high and satisfactory. internal consistency has been reported for its 3 subscales (α=0.72-0.85).37 Test-retest reliability of the DHI is high (r=0.97),37 and it has been recently translated into Arabic for use.1 The Arabic DHI was able to discriminate between control participants and persons with dizziness.1
The Dynamic Gait Index-4
The DGI-4 was developed based on the original Dynamic Gait Index.29 Factor analysis revealed that 4 items were as helpful as 8 items, thus shortening the test. The DGI-4 was developed for persons with balance and vestibular disorders.29 Persons are asked to: 1) ambulate over a 4.1m walkway, 2) to ambulate at their self-selected speed, fast and slow speeds, plus to walk while 3) turning their head and 4) looking up/down. Each of the 4 tasks is scored on a 0 to 3 ordinal scale, with a possible range of scores from 0-12. Higher scores indicate more stable ambulation.
Data analysis
Subject characteristics and responses/performance on outcome measures were described as means/SD for continuous and frequency (%) for categorical variables. The internal consistency of the Arabic FES-I was evaluated using coefficient theta, based on a principal component factor analysis. Coefficient theta ranges from 0-1, with 1 indicating perfect internal consistency and is derived from the individual factor weightings for multi-construct outcome scales. Internal consistency for individual factors on the Arabic FES-I was judged to be satisfactory if theta >0.70. Construct validity of the Arabic FES-I was tested using correlational analysis with the Arabic DHI and the Arabic DGI-4. Spearman non-parametric correlational coefficients were used to describe the inter-scale associations. Correlations were judged to be significant at p<0.05 and magnitude of significant coefficients was evaluated as follows: small (0.1-0.29), medium (0.3-0.5) and large (greater than 0.5).38 All data analysis was performed using IBM Statistical Package for Social Science statistics for Macintosh, version 22 (IBM Corp, Armonk, NY, USA)
Results
Subject characteristics
Table 1 includes the mean age (± SD) of the participants, gender, Arabic DHI score, Arabic FES-I, and the Arabic DGI-4. The patient group consisted of a significantly greater proportion of females (84%) than the control group (49%, p<0.001). There were no differences noted in age, Arabic DGI-4, Arabic DHI, or Arabic FES-I scores between the patient group and the control participants.
Descriptive values for age, gender, and outcome measure scores for healthy controls and patients with balance and vestibular disorders (mean ± standard deviation except where indicated).
Internal consistency
The individual item scores on the Arabic FES-I demonstrated a correlation with total FES-I score ranging from 0.50 (item 8: walking around the neighborhood) to 0.84 (item 14: walking on uneven surface). Principal component analysis demonstrated a 3-factor solution predicting 51%, 12%, and 7% of total variance (total variance explained = 69%). Based on the latent root for the 3 factor loadings, coefficient theta was found to be 0.93 for the dominant factor in the Arabic FES-I. All items demonstrated loadings on factor 1, ranging from 0.56 (item 10: going to answer the telephone) to 0.84 (item 14: walking on uneven surfaces).
Factors 2 and 3 were found to present with insufficient internal consistency at 0.51 and 0.11. Based on the results from the predominant factor, the Arabic FES-I was judged to display excellent internal consistency, consistent with findings from other studies, which found a unitary factor structure.31
Construct validity
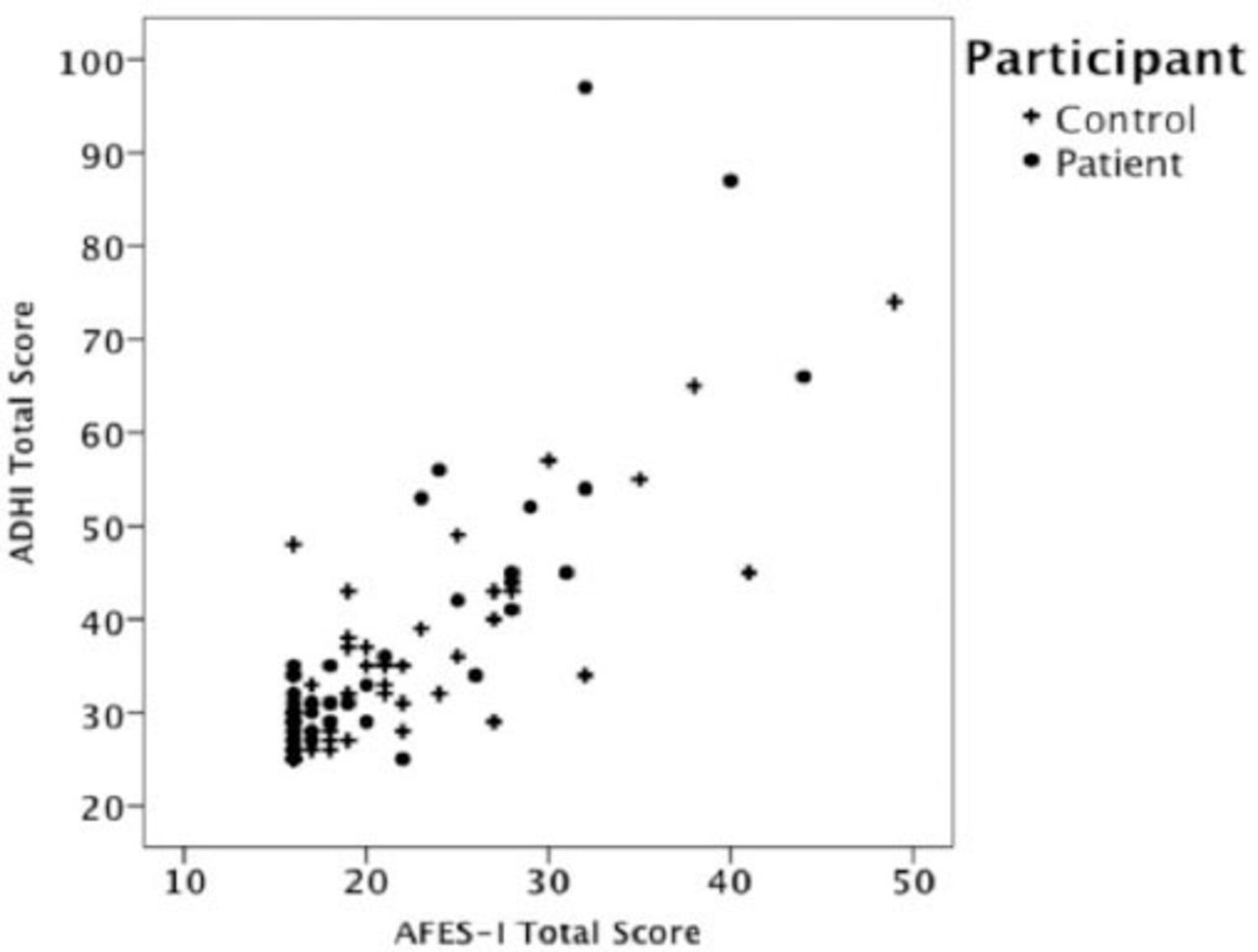
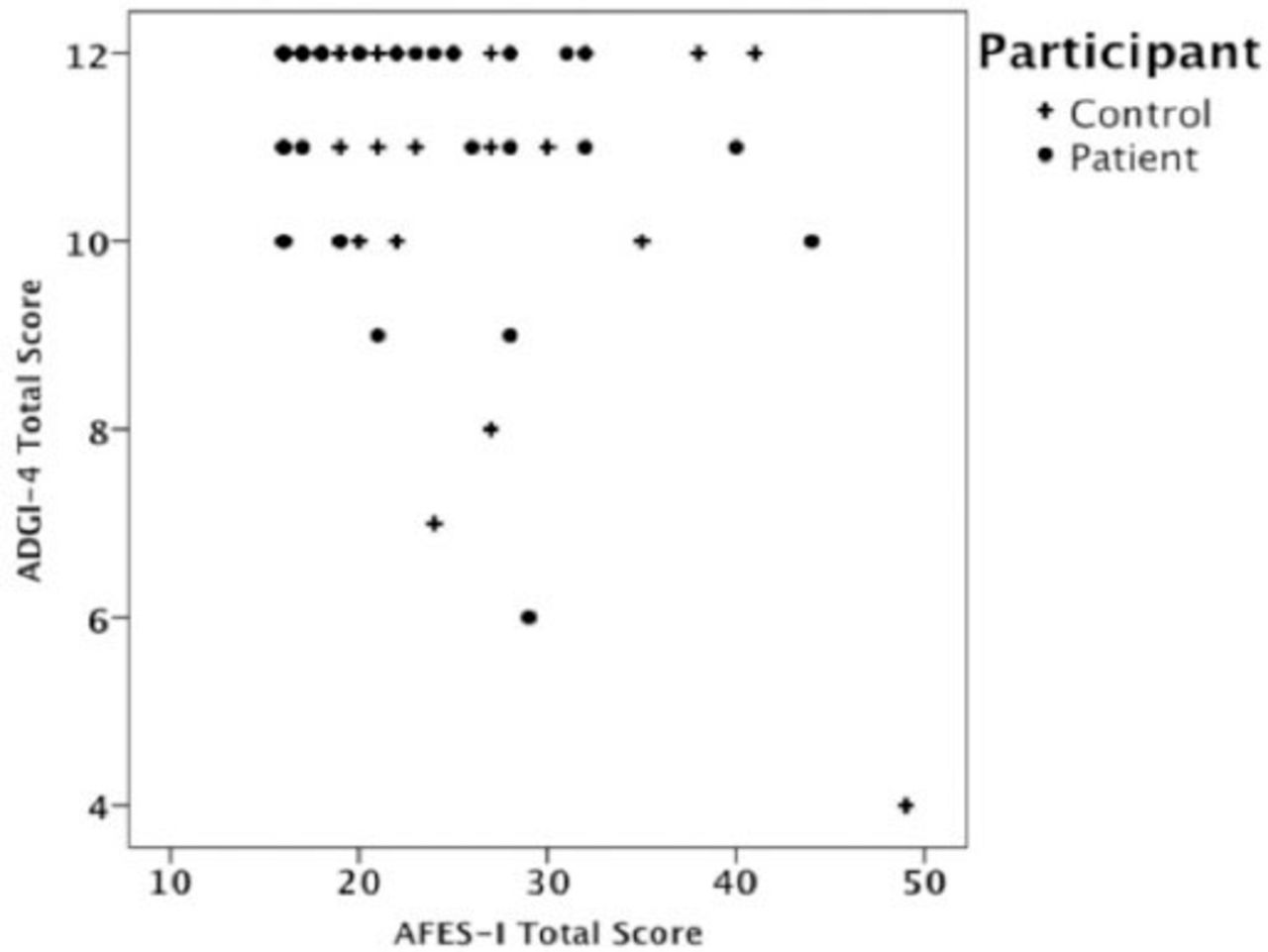
The Arabic FES-I was found to be significantly correlated with the Arabic DHI with a large magnitude correlation coefficient (r=0.76, p<0.011) (Figure 1). Translated FES-I scores were significantly correlated with DGI-4 scores with a medium magnitude correlation coefficient (r=0.30, p=0.003) (Figure 2). There was a gender effect in the Arabic DHI and the Arabic FES-I in control subjects. Females had a significantly higher mean Arabic DHI (p=0.026) than males. Females had a significantly higher mean Arabic FES-I score than males (p=0.040). There was a significant association between age and Arabic FES-I scores in patients, r=0.37 (p=0.016).
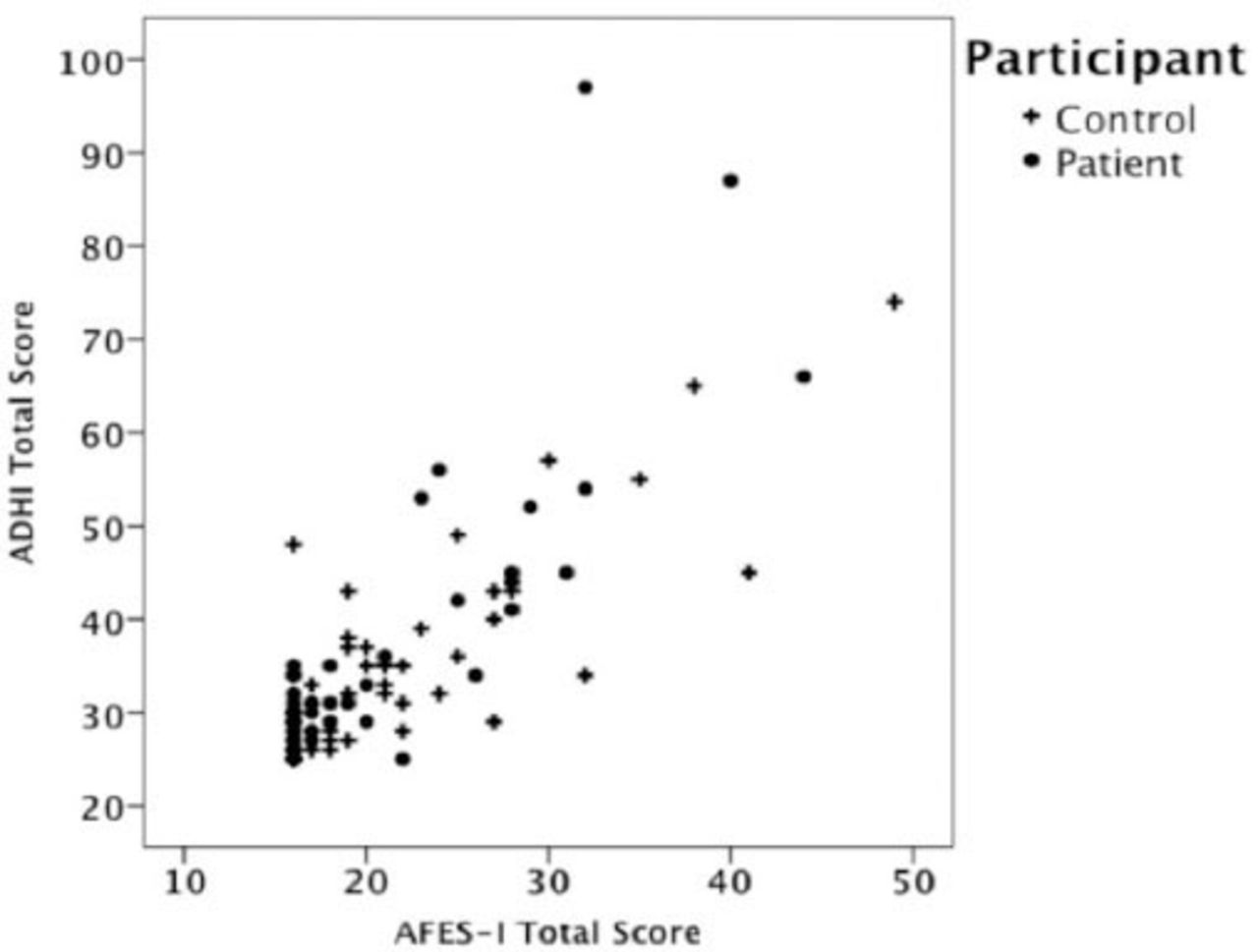
Scatterplot of the Arabic Dizziness Handicap Inventory (ADHI) versus the Arabic Falls Efficacy Scale International (AFES-I) scores by subject type among healthy controls and patients with balance and vestibular disorders.
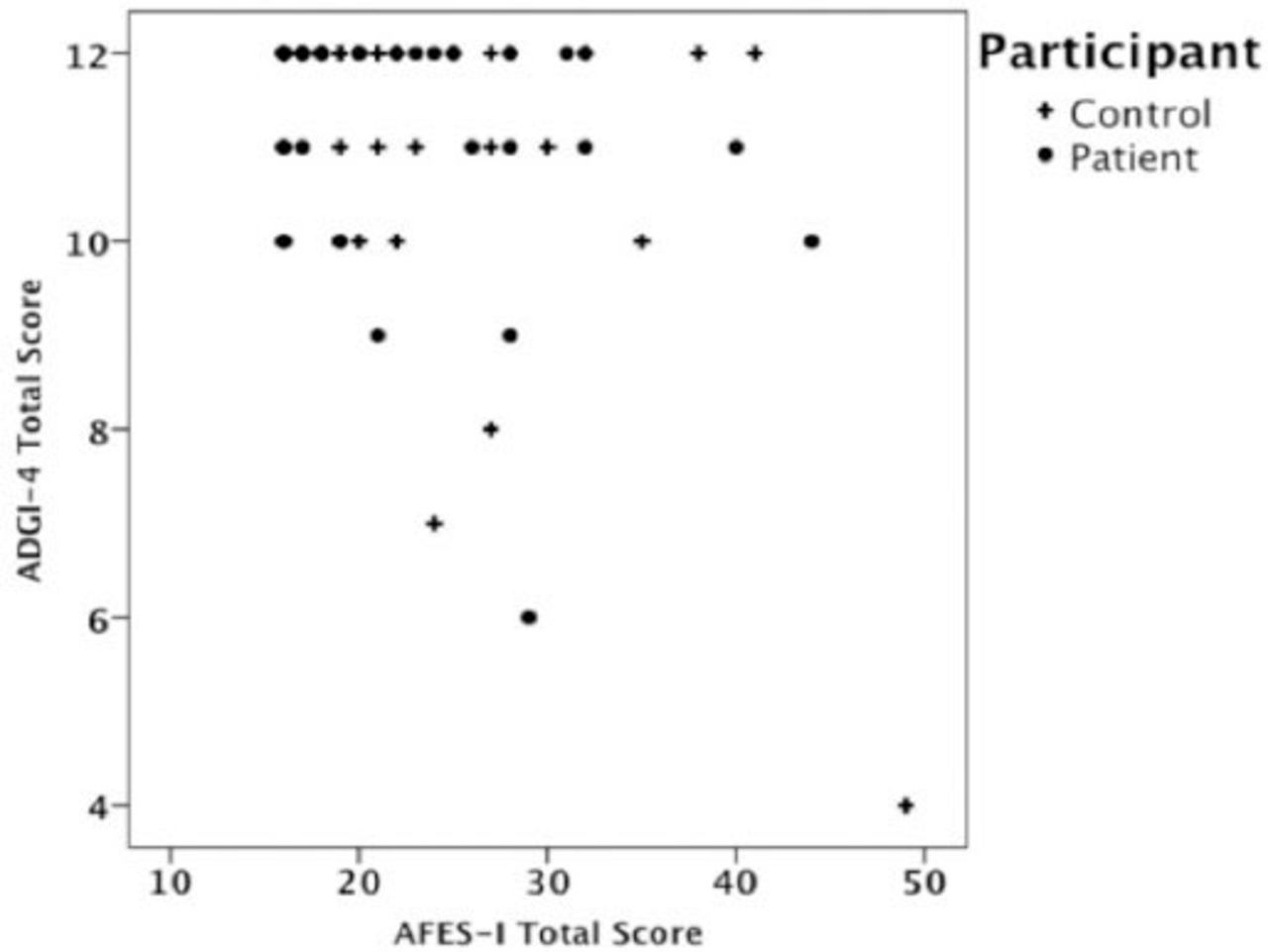
Scatterplot of the Dynamic Gait Index-4 (DGI-4) versus the Arabic Falls Efficacy Scale-International (AFES-I) by subject type among healthy controls and patients with balance and vestibular disorders.
Discussion
The Arabic FES-I demonstrates excellent internal consistency with a single factor solution and sufficient construct validity in a sample of combined patents with vestibular disorders showing minimal impairment and self-reported handicap and control participants. The Arabic FES-I as translated could be used with persons with dizziness to determine their fear of falling. The Arabic FES-I is available now to persons whose primary language is Arabic as the first tool that has been translated for use for persons at risk for falls. There is a scarcity of other validated self-report
Arabic falls measures in the literature
It was not surprising that the Arabic FES-I and the 4-item DGI had a low correlation value. Measures of gait and self-report questionnaires tend not to be strongly related in the literature.39-41
Many studies of persons with vestibular disorders include an older cohort than our study.42-48 It was much more difficult to recruit older adults in Riyadh, Saudi Arabia than anticipated. In a recent report (mean age 38; n=470), men, older adults, and those who were well educated were dissatisfied with the informed consent process in Saudi Arabia,49,50 suggesting that older participants may not have “trusted” the consent process in our study and therefore did not agree to participate. Fayez et al51 previously reported that 60% of the members of the medical team in 4 Saudi Arabian hospitals (n=370) did not feel that informed consent was performed ethically in Saudi Arabia. It may be that the older adults who were approached did not fully understand the value of the study or were fearful of participation. The literacy rate of women in Saudi Arabia in 2010 was 81%, and in men 90% over the age of 15.52 For older adults, the rates are much likely lower than those stated above. One of the exclusion criteria was that participants had to be able to read Arabic, and older adults were more likely to be illiterate in Arabic than younger adults.
The mean age of our sample was 32 years, which is much younger than typically reported in the literature for persons with balance and vestibular disorders.53 Typically, in most large sample papers, the mean age of participants with vestibular disorders is closer to 60 years of age.53 The female:male ratio is what is typically described in the literature (~3:2).36,54 The scores on the DGI-4 had a strong ceiling effect as 70% of all participants (63% patients, and 75% controls) demonstrated a perfect 12/12 score. This could possibly have occurred because the patients with balance and vestibular dysfunction were so young compared to previous studies. If we had been able to recruit more patients that were older, the correlation between the Arabic FES-I and the Arabic DHI might have been better since low variability within a sample can cause a lower correlation coefficient. The ceiling effect of this young group on the measures recorded might have also have affected the correlations. Most persons recruited had the diagnosis of BPPV. Whitney et al55 reported a mean DHI score of 42 (n=84) and in persons with various vestibular diagnoses the DHI scores were 46 (n=289) with a mean age of 61. In the present study, the mean Arabic DHI score was 37 with an average age of 52. Friscia et al36 reported mean DHI scores of 45 in persons with both peripheral, central, or combined peripheral and central disorders with a mean age of 56. The patients with BPPV participants had mean Arabic DHI scores of 42.5 ± 25.7, so the Arabic DHI scores are similar to the other studies.36,53 Participants with BPPV were older on average by 6 years than the other patients in our study. Twenty-seven percent of Friscia et al’s sample had BPPV, which is similar to our sample.36 Age may have been a factor that affected the lower (better) overall Arabic DHI scores in our sample.
A possible limitation of our study is that the authors did not collect falls data, similar to Ulus et al56 in their validation of the Turkish FES-I. Ulus et al56 tested 2 measures of balance (the Timed Up & Go and the Berg Balance Scale) plus the Barthel Index (which is a measure of activities of daily living) to determine construct validity in their study. In the present validity study, one test of balance (the DGI-4), and a measure of dizziness were utilized.
In conclusion, the Arabic FES-I has established concurrent validity and can be used to assist with clinical decision making related to an individual’s concern of falling in people with vestibular and balance disorders.
Footnotes
Disclosure
This work was full financially funded by King Saud University through the Vice Deanship of Research Chairs, Rehabilitation Research Chair. No potential conflicts of interest relevant to this article were reported and the study was not supported by any drug company.
- Received November 18, 2014.
- Accepted April 27, 2015.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.