


Abstract
Objectives: To examine the fetal axillary nerve to reveal and compare its morphometric features within the second and third trimester.
Methods: This study was conducted at the Anatomy Department, School of Medicine, Mersin University, Mersin, Turkey. Thirty-five fetal shoulders were studied to provide anatomic data and to describe its position with regard to certain landmarks around the shoulder.
Results: The shortest distance between the axillary nerve and the glenoid labrum was found 2.27 mm and 2.89 mm in the second and third trimester fetuses, respectively. The shortest distances between the anterior and posterior acromial tips and the axillary nerve were also measured and were used with arm length measurements to define the anterior and posterior indexes.
Conclusion: The indexes show that the distance between the axillary nerve and the anterior/posterior acromial tips are approximately one-fourth of the arm length in both the second and third trimester fetuses. The data presented in this study will be of use to surgeons, particularly to pediatric and orthopedic surgeons who will undertake surgical procedures in the axilla and arm in the newborn or early childhood.
There is detailed knowledge regarding the morphological features of the axillary nerve in adults, however, it in the fetal period we encountered no information. Brachial plexus injuries have been reported with a rate of 0.38-2.6 per thousand live births. Shenaq et al1 mentioned that the diagnosis, observation, and therapy are the initial approaches to these injuries, and should be initiated immediately. They also stated that early surgical intervention is essential to maximizing the long-term improvements in selected patients by helping to prevent residual growth deformities and underdevelopment of the affected limbs. The surgical treatment options include the reconstruction and neurotization.2 For the axillary nerve injuries, for example in case of C5-C6 avulsion, in which the upper roots have been avulsed from the spinal cord, and the clinical picture is that of a classic Erb palsy, they preferred to use neurotization technique. In this type of avulsion, the upper roots are not available as donors, and the C7-T1 roots are uninvolved. So, the suprascapular nerve is neurotized by the ipsilateral spinal accessory nerve, and the axillary nerve is neurotized by redundant branches to the triceps to ideally restore shoulder and elbow function. The thoracodorsal or the subscapular branches can also be neurotized to the axillary nerve to provide better shoulder function. Thus, anatomical details of the axillary nerve in fetal period become essential for such operations. We carried out this study to evaluate these parameters regarding the axillary nerve anatomy, which may be helpful to surgeons in certain conditions, such as end-to-side neurorrhaphy in brachial plexus reconstruction, neurotization, proximal humeral fracture repair, and shoulder dislocation treatment in the early childhood.
Methods
This study was performed on 35 spontaneously aborted fetuses (21 female, 14 male), aged between 20 and 37 weeks of gestation. The material came from the collection of the Anatomy Department of the School of Medicine. Fetuses without any pathology or anomaly in their extremities were included in the study. This study was approved by the Ethics Board of the School of Medicine, Mersin University. The following parameters were examined in this study: location, course, and branches of the axillary nerve; diameter of the axillary nerve where it exits from the quadrangular space; course of the axillary nerve deep to the deltoid muscle, and to determine the innervation patterns of the axillary nerve branches to the deltoid muscle, and distance of the axillary nerve from certain landmarks. Gestational ages of the fetuses were determined using biparietal diameter, head circumference, and foot length. Fetuses were divided into 2 groups according to their gestational ages: Group 1 - 19 second trimester fetuses; and Group 2 - 16 third trimester fetuses. Dissections were performed with a dissecting microscope (OPMI pico 200, Carl Zeiss, rue Louis Armand, Paris, France), and all parameters were measured with Mahr digital caliper (MarCal 16 ER, Swiss Instruments Limited, Mississauga, ON, Canada) by the same researcher. Measurements were recorded and were given in millimeters (mm) in Table 1. Before any dissection, arm length, which was accepted as the distance between the most lateral point of acromion and the lateral epicondyle was measured. Then, dissections were performed to reveal the brachial plexus and the thickness of the axillary nerve was measured at the point where it diverged from the posterior cord before giving its branches. At this stage, in order to detect the course of the axillary nerve beneath, the deltoid muscle was dissected from its anterior and posterior avascular raphe by anterior and posterior deltoid splitting approaches. Thus, the clavicular and acromial heads of the deltoid were identified. The axillary nerve passing anteriorly was found beneath the muscle and the distances between the anterior and posterior tips of the acromion to the axillary nerve were measured at the anterior and posterior raphes. Then, the clavicular and acromial parts of the deltoid muscle were removed from their insertions. This provided a clear vision of the glenoid capsule. Parameters related to the coracoid tip and glenoid capsule were measured. Finally, shoulder joint capsule was cut, the humeral head was separated from the glenoid capsule, and the glenoid labrum was identified. The shortest distance between the axillary nerve and the glenoid labrum was measured. The course of the axillary nerve from its origin from the posterior cord till the deltoid muscle was divided into three segments as proximal, anterior and distal to the subscapularis muscle, regarding its position to the muscle. The organization of the nerve’s fasciculi and the segments where the branches arose, were recorded.
Descriptive statistics for the measurements defining the distances between the axillary nerve and several reference points as well as its thicknesses at various points. All measurements were given in millimeters.
Statistical analysis was performed by Statistical Package for Social Sciences version 12 (SPSS Inc., Chicago, IL, USA). Normal distribution for all parameters was found with the Kolmogorov Smirnov test. Paired t test was applied for the detection of significance between the sides. For both trimesters, possible difference between the right and left side arm lengths was tested with univariate analysis of variance (ANOVA). Difference between the groups for each parameter was evaluated by Student’s-t test. Pearson’s correlation test was used for the evaluation of the relationships between certain parameters. P<0.05 was accepted as statistically significant for all analysis.
Results
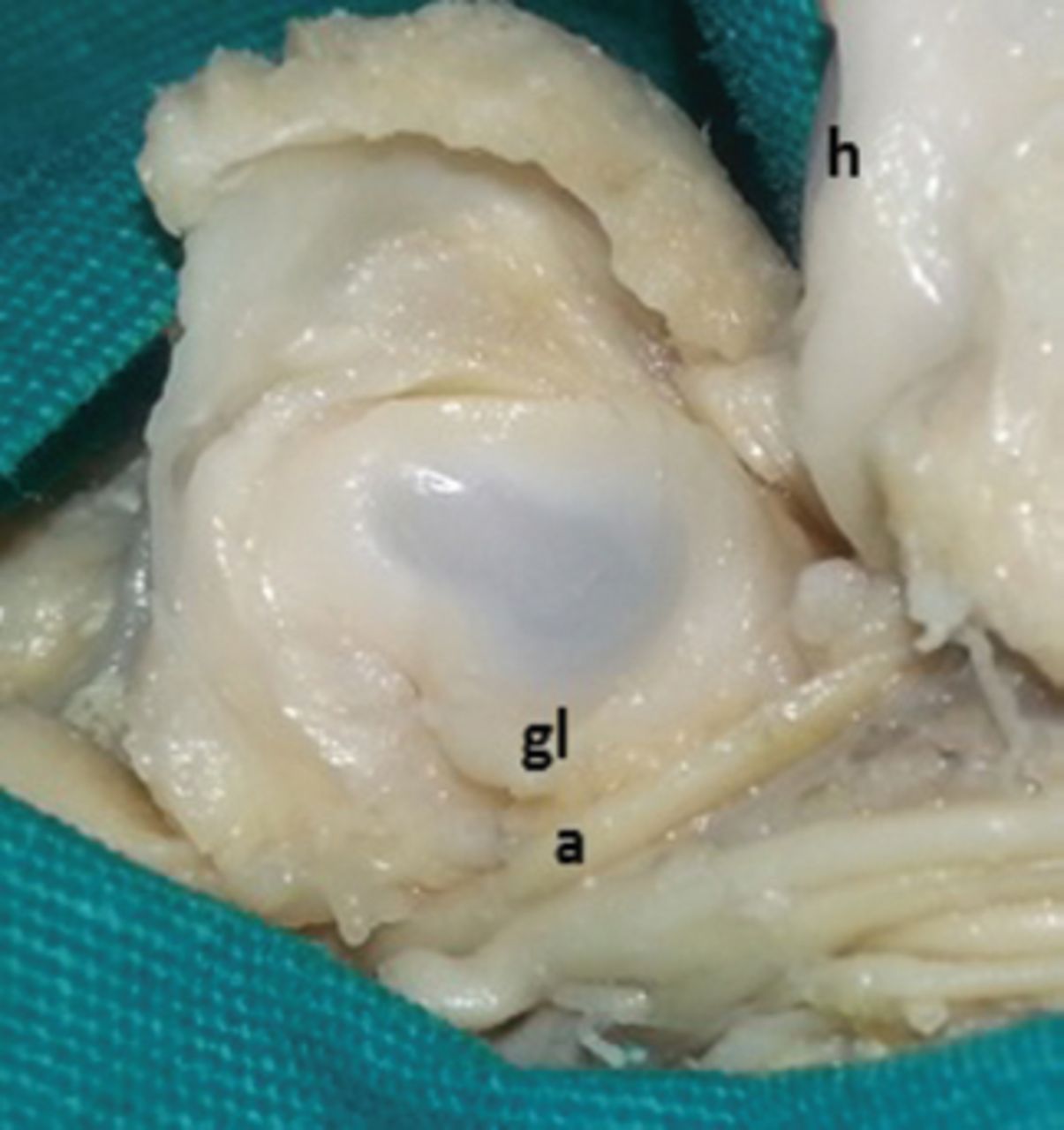
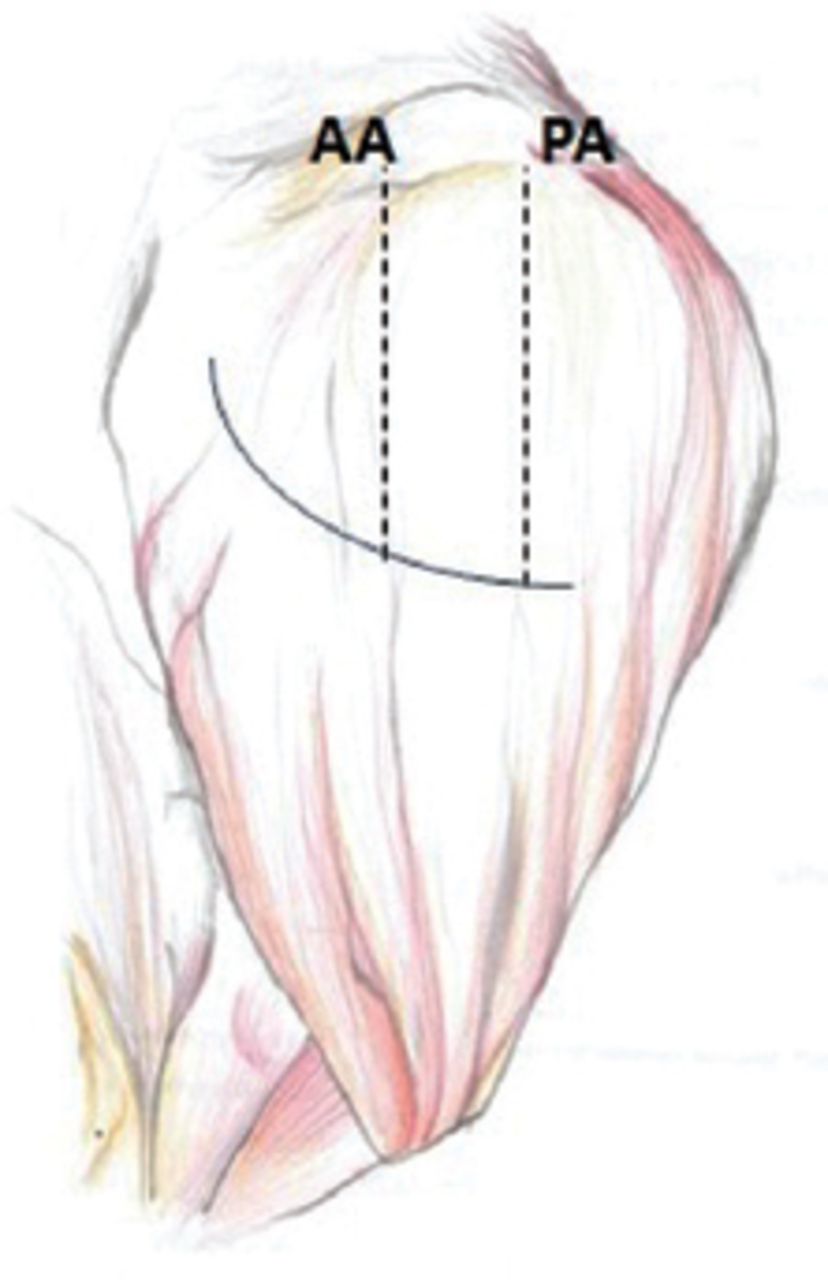
Arm lengths was found 43.47 ± 6.70 mm for the right side and 43.79 ± 7.43 mm for the left side in second trimester fetuses, while they were 61.56 ± 10.11 mm for the right and 61.10 ± 9.71 mm for the left side in third trimester fetuses. For both trimesters, no significant difference was found between the right and left side arm lengths with ANOVA (p=0.974). This measurement was used to define the anterior and posterior indexes. In all fetuses, axillary nerve was diverging from the posterior cord of the brachial plexus. The distance between the coracoid tip and the diverging point of the axillary nerve from the posterior cord was 8.85 mm in the second, and 15.77 mm in third trimester fetuses. There was a statistically significant difference between the 2 groups (p=0.0001). The closest point between the axillary nerve and the glenoid labrum was slightly medial to the most inferior point of the glenoid labrum, and from this point, the nerve was receding from the glenoid labrum (Figure 1). The shortest distance between the nerve and the glenoid labrum was 2.30 mm in the second, and 2.89 mm in third trimester fetuses. The difference between them was found to be statistically significant (p=0.001) (Table 1). The shortest distance between the anterolateral tip of acromion and the axillary nerve, which was provided by deltoid-splitting approach through the anterior avascular raphe, was found to be 10.52 mm in the second, and 13.68 mm in third trimester fetuses (Figure 2) (Table 1). On the other hand, the shortest distance between the posterolateral tip of acromion and the axillary nerve, which was provided by deltoid-splitting approach through the posterior avascular raphe, was found to be 11.59 mm in the second, and 15.40 mm in third trimester fetuses (Figure 2) (Table 1). The above-mentioned distances and the arm length were found to be correlated in both groups, thus we defined 2 indexes: anterior and posterior axillary nerve indexes. The anterior axillary nerve index was defined as the ratio of the distance between the axillary nerve and the anterior acromial tip to the arm length. The anterior axillary index was 0.24 in second trimester and 0.23 in third trimester fetuses. No significant difference was found between the 2 groups (p=0.092) using the Student’s t-test. Similarly, the posterior axillary nerve index was defined as the ratio of the distance between the axillary nerve and the posterior acromial tip to the arm length. The posterior axillary index was 0.27 in second trimester, and 0.25 in third trimester fetuses. Again, there was no significant difference between the 2 groups (p=0.250).

Passage of the axillary nerve (a) close to the glenoid labrum (gl). The closest point between the axillary nerve and the glenoid labrum was slightly medial to the most inferior point of the glenoid labrum. h - humeral head

The shortest distance between the anterolateral (AA) and posterolateral (PA) tips of acromion and the axillary nerve which was provided by deltoid-splitting approach through the anterior and posterior avascular raphes of the deltoid muscle.
When the course of the axillary nerve was examined, it was found in all fetuses that the nerve was a single trunk in the first segment. In the second segment, the axillary nerve was observed as divided into 2; first as medial and lateral then anterior and posterior trunks. Nerve branches were the continuations of these trunks. No branches were observed arising from the first segment. The first branch of the posterior trunk in all fetuses was the nerve to the teres minor muscle and then the upper lateral cutaneous nerve of the arm. The posterior trunk was then continuing as the branch to posterior deltoid. The anterior trunk contained all fibers that innervate to the anterior and middle deltoid. In only 2 shoulders (2.9%), apart from the ones from the posterior trunk, extra branches were arising from the anterior trunk to the posterior deltoid. The thickness of the axillary nerve at the point where it diverged from the posterior cord was found to be 1.05 mm in the second, and 1.32 mm in the third trimester fetuses (Table 1).
Discussion
Reviewing the literature on fetal axillary nerve, we encountered no data regarding morphometric features of fetal axillary nerve. In this study, we performed anatomical dissections to gather detailed data on the course, branches, and morphometric parameters of the fetal axillary nerve. Apaydın et al3 investigated the relationship of the axillary nerve to the shoulder capsule and the subscapularis muscle in adult cadavers, and defined anatomical landmarks and regions that can be practically used in anterior surgical approaches to the shoulder region. Lo et al4 mentioned that the axillary nerve is at greatest risk during dissection when performing surgery about the coracoid. In this study, we provided the measurements for the closest distance between the anteromedial aspect of the coracoid tip and the axillary nerve at the point where it diverges from the posterior cord. We think this measurement may be helpful to surgeons during surgical interventions.
The distance between the axillary nerve and the glenoid labrum may also be critical in certain surgical procedures on the shoulder. The results of our study may provide a safe access when performing surgical procedures on the shoulder. Duparc et al5 examined the axillary nerve course in adults by dividing it into 5 segments. We preferred to examine the course of the nerve by dividing it into 3 segments as proximal, anterior, and distal to the subscapularis muscle, regarding its position to the muscle. A safe zone for the axillary nerve deep to the deltoid muscle has been studied by researchers.6,7 Also, Nassar et al8 described an axillary nerve index in adults, which can be used to predict the location of the axillary nerve. Similarly, we described 2 indexes; the anterior index (distance between the nerve and the anterior acromial tip/arm length), and the posterior index (distance between the nerve and the posterior acromial tip/arm length). These indexes clearly show that the distance between the axillary nerve and the anterior/posterior acromial tips are approximately one-fourth of the arm length in both the second and third trimester fetuses. This safe zone would be of use in regional operations in newborns, or during early childhood.
Wozniak9 found the axillary nerve diameter in fetuses as 0.77 mm (on the left), and 0.78 mm (on the right). However, the exact coordinates of the axillary nerve where the measurements were taken and the average diameters of the nerve in different trimesters were not mentioned. We measured the diameter of the axillary nerve at the point where it diverges from the posterior cord. We found larger diameters than those of Wozniak9 both in the second and third trimester fetuses. Although we had 16 third trimester fetuses in the department archive, only 7 of them were more than 30 weeks old. This can be considered as the limitation of the study.
In conclusion, this study provides information regarding the normal course, branching pattern, and dimensions of the axillary nerve in the fetal period, as well as the distances between the axillary nerve and certain reference points. This data will be of use to surgeons, particularly to pediatric and orthopedic surgeons who undertake surgical procedures in the axilla and arm region of the newborn, or during early childhood, such as, end-to-side neurorrhaphy in brachial plexus reconstruction, neurotization, proximal humeral fracture repair, and shoulder dislocation treatment.
Footnotes
Disclosure
This study was supported by the Scientific Research Projects Commission (BAP-SBE TTB (TU) 2012-3 YL) of Mersin University, Mersin, Turkey.
- Received January 5, 2015.
- Accepted May 18, 2015.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.