


Abstract
Objective: To evaluate the correlation between the distance of craniectomy from the midline and hydrocephalus after DC.
Methods: The following electronic databases were searched from their inception to June 2015: Cochrane Library, MEDLINE, Science Direct, EMBASE, Scopus, Google Scholar, the Chinese Biomedical Database (CBM), and the Chinese National Knowledge Infrastructure (CNKI). All randomized clinical trials, prospective cohort, retrospective observational cohort, and case-control studies investigating the relationship between distance of craniectomy from the midline and hydrocephalus after DC were enrolled. The Cochrane Collaboration’s software RevMan 5.3 was used for meta-analysis.
Results: Six retrospective cohort studies involving 462 participants were included. Pooled analysis of 4 studies suggested that craniectomy close to the midline (<25 mm) was associated with a significantly increased risk of postoperative hydrocephalus (odds ratio [OR] = 3.61, 95% confidence interval [CI]: 1.3 - 9.97, p=0.01). However, meta-analysis of 4 studies did not find statistical differences when comparing the distance of craniectomy from the midline in the hydrocephalus group and that in the non-hydrocephalus group (OR = −0.14, 95% CI: −0.44 - 0.15, p=0.34).
Conclusions: Available evidence was insufficient to support the theory that craniectomy close to the midline increases the risk of developing hydrocephalus after DC. Well-conducted randomized clinical trials are required to verify this issue.
Decompressive craniectomies have been carried out more frequently in the past decades because of their known benefits in treating situations such as traumatic brain injury (TBI) with medically refractive intracranial pressure (ICP), subdural hematoma, and cerebral swelling due to vasospasm after subarachnoid hemorrhage.1 This treatment involves removing part of the skull to allow the brain to swell outward without being squeezed, thereby preventing brain tissue shifts and life-threatening cerebral herniation.2 The beneficial effect of DC in reducing ICP has been well-documented in several studies. However, several delayed complications of DC have been reported, including sinking flap syndrome, extra-axial fluid collection, hydrocephalus, and the development of subdural hematomas.3,4 Hydrocephalus is a common complication after DC. Variable results have been reported from 0–88.2%.5,6 Some authors found that DC is a risk factor for hydrocephalus,7,8 whereas others did not find relationship between them.9,10 There is still no conclusive evidence on the relationship between the superior limit of DC and hydrocephalus.
There have been numerous studies investigating the risk factors for hydrocephalus after DC.11-16 Some studies reported that patients with DC whose superior limit was <25 mm from the midline had a significantly increased risk of developing postoperative hydrocephalus,2,11,13,14 whereas other studies found that the distance of craniectomy from the midline was not significantly associated with hydrocephalus.12,15,16 Thus, the relationship between the superior limit of DC and hydrocephalus is still controversial. To precisely determine this issue, we conducted a systematic review to critically evaluate all relevant, currently available trials.
Methods
Search strategies
We searched the Cochrane Library, MEDLINE, Science Direct, EMBASE, Scopus, Google Scholar, the Chinese Biomedical Database (CBM), and the Chinese National Knowledge Infrastructure (CNKI) from their inception to June 2015 for relevant studies using appropriate combinations of medical subject headings terms and key words, including decompressive craniectomy, craniectomy, surgery, hydrocephalus, ventriculomegaly, and complication. Corresponding Chinese terms were also searched. References were addressed in original articles, and reviews were further searched for relevant studies. We included studies published in English and Chinese. We excluded studies as follows: 1) studies that did not evaluate the correlation between the distance of craniectomy from the midline and hydrocephalus after DC, 2) studies that could not provide enough raw data for statistical analysis, 3) studies whose data were integrated by another studies, and 4) studies published in other languages.
Study selection
Two authors assessed the titles, abstracts, and full texts of the initially identified studies to determine eligibility independently. All randomized clinical trials and prospective cohort, retrospective observational cohort, and case-control studies that evaluated the correlation between distance of craniectomy to the midline and hydrocephalus after DC were included in our analysis. Hydrocephalus had to be diagnosed according to a standardized criterion.
Data extraction
According to pre-established eligibility criteria, 2 reviewers independently reviewed all citations and selected eligible studies using a standardized data abstraction form. Disagreements were resolved by consensus. Data were extracted for 1) study characteristics (author and year of publication, country, study design, and sample size), 2) patient demographics, 3) treatment details (distance of craniectomy to the midline), and 4) study outcomes (incidence of hydrocephalus). We contacted authors for clarification on study samples or for missing data.
Methodological quality of included studies
We used the criteria for reporting observational studies proposed in the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement to complete a methodological evaluation of the included observational studies.17
Statistical analysis
Statistical analyses were performed using Review Manager Software (Review Manager (RevMan) [Computer program] version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014.). All tests were 2-sided, and the significance level was set at 0.05. Statistical analyses for continuous variables or dichotomous variables were conducted. Mean differences (MDs) were used for the analysis of continuous variables, and odds ratios (OR) were used for dichotomous variables. When possible, we extracted the adjusted ORs from the observational studies and then computed a pooled OR. If not, we used RevMan 5.3 to abstract the odds ratios. For studies without sufficient information, we contacted the primary authors in order to acquire and verify data when necessary. The chi-square test and the Higgins I2 test were used to assess heterogeneity. We pooled the data across studies using fixed-effects models if statistical heterogeneity did not exist. If appropriate, a meta-analysis would be conducted using random effects models when the I2 value exceeded 50%. We constructed funnel plots to assess publication bias.
Quality of evidence
Studies were graded and assigned a quality rating with respect to the key question according to the Centre for Evidence-Based Medicine criteria. Studies were graded from level 1 (strongest evidence) to level 5 (weakest evidence).18
Results
Study selection and methodological quality
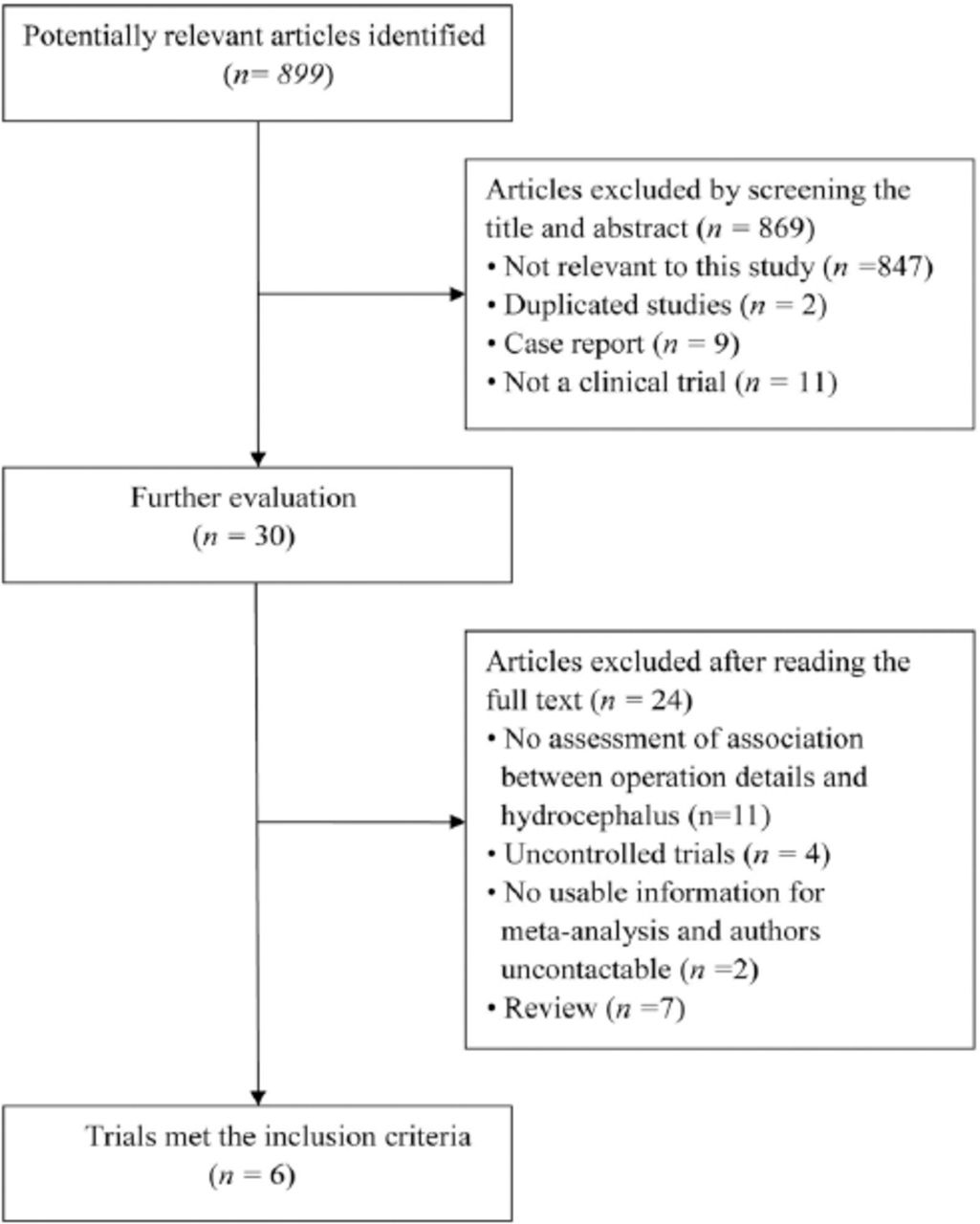
The literature search revealed 899 potentially relevant articles, of which 6 studies2,12-16 involving 462 participants were included in our analysis (Figure 1). One eligible study11 was excluded because its data was integrated by another included study.13 All included studies were published, peer-reviewed papers. No randomized controlled trial was found. All 6 included studies were observational cohort studies, and their general information is listed in Table 1. All studies defined hydrocephalus after DC as radiographic evidence of progressive ventricular dilation, with an Evans’ index >0.3, narrowed CSF spaces at the convexity on CT scans, and associated with a worsening neurologic status (not due to infections or other medical causes). Four studies were conducted in Asia,2,14-16 one in Europe,13 and one in Australia.12 All patients were adults, and the primary diseases included TBI, hypertensive intracerebral hemorrhage, and cerebral infarction. Four studies2,13,14,16 evaluated the correlation between DC with a superior limit <25 mm from the midline and the incidence of distance of hydrocephalus, while 2 studies12,15 compared the distance of craniectomy to the midline in a hydrocephalus group and a no-hydrocephalus group.

Flowchart of trial selection for a meta-analysis on the impact of operation detail on hydrocephalus after decompressive craniotomy.
Characteristics and outcomes of the studies included in the meta-analysis on the impact of operation details on hydrocephalus after decompressive craniotomy.
In the 6 observational cohort studies, 5 studies adequately described their study population (including missing data and patients lost during follow-up), 4 studies performed adequate control for confounding using multivariate logistic regression analysis, and 3 presented their funding sources. Table 2 provides a more complete evaluation of methodological quality.
Methodological quality of included studies (STROBE criteria) in a meta-analysis on the impact of operation details on hydrocephalus after decompressive craniotomy.
Outcome measures
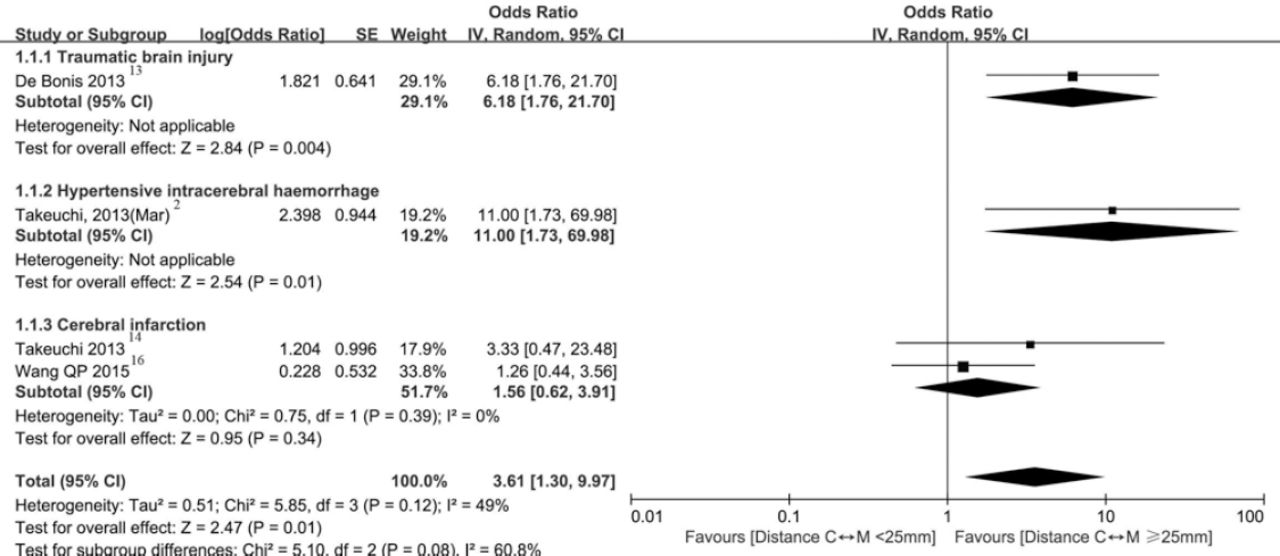
Four studies2,13,14,16 compared the incidence of postoperative hydrocephalus in the superior limit <25 mm from the midline group and the superior limit ≥25 mm group. Moderate heterogeneity between the trials was observed (χ2=5.85, p=0.12, I2=49%, Figure 2), and we conducted the meta-analysis using the random effects models. The meta-analysis showed that craniectomy close to the midline (<25 mm) was associated with a significantly increased risk of postoperative hydrocephalus (OR=3.61, 95% CI: 1.30 - 9.97, p=0.01, Figure 2).

Forest plot of correlation between distance of craniectomy to the midline and hydrocephalus after decompressive craniectomy. The pooled estimates were obtained using a fixed-effects model. IV - inverse variance, C<->M - craniectomy to midline, SE - standard error, CI - confidence interval, df - degrees of freedom. Mar - the article published in March
Two studies12,15 compared the distance of craniectomy to the midline in a hydrocephalus group and a no-hydrocephalus group. Other studies did not give detailed information on the accurate distance of craniectomy to the midline of every patient. We tried to contact authors for original data, but only one author12 sent us portions of data. Thus, we could not perform a meta-analysis of all included studies. We extracted available data and conducted a meta-analysis accordingly. The results showed that there were no statistical differences when comparing the distance of craniectomy to the midline in a hydrocephalus group and a no-hydrocephalus group (OR = −0.14, 95% CI: −0.44-0.15, p=0.34, Figure 3).

Forest plot for comparison of the craniectomy distance to the midline in the hydrocephalus group and the no-hydrocephalus group. The pooled estimates were obtained using a fixed-effects model. IV - inverse variance, SD - standard deviation. CI - confidence interval, df - degrees of freedom. Mar - the article published in March

Discussion
Decompressive craniectomy is frequently reported as a salvage procedure for malignant intracranial hypertension, but it commonly leaves patients with obvious sequelae. Hydrocephalus is a common and tough complication after DC, which may cause clinical deterioration and require reoperation of cerebrospinal fluid drainage.3,4
Several researchers have investigated the mechanisms of hydrocephalus after DC in order to control it better. Jiao et al7 reported that advanced age, subarachnoid hemorrhage (SAH), and hygroma (subdural, or interhemispheric) are correlated with the development of hydrocephalus. Tian et al9 found that traumatic SAH is a risk factor for the development of hydrocephalus in head injury patients. Honeybul et al12 indicated that injury severity is a significant independent risk factor for hydrocephalus after DC. Some authors have noted that DC itself was a risk factor for hydrocephalus. Choi et al8 found that the size of DC is an influencing factor for hydrocephalus after TBI, and they believed that DC itself was a risk factor for hydrocephalus. In contrast, some authors hold that DC is not an impact factor for hydrocephalus. Waziri et al19 found no relationship between DC and hydrocephalus through retrospectively analysing a cohort of consecutive patients. Significant attention has been given to the mechanisms of hydrocephalus after DC; however, no final conclusion has yet been reached on this matter, and the mechanisms of hydrocephalus after DC are still controversial.
Some authors found that the distance of craniectomy to the midline was a factor associated with hydrocephalus after decompressive craniectomy. They considered that when the skull was removed too close to the midline, the external force compressing the temporal and parietal bridging veins was reduced, and that this might cause an increase in venous blood flow and extracellular fluid absorption and a decrease in brain parenchyma volume, causing a consequent increase in ventricular volume, which resulted in post-operation hydrocephalus.11,20 This was an inspiring finding because it was a controllable factor. The neurosurgeons can easily minimize the risk of postoperative hydrocephalus caused by DC. However, the results of consequent studies are inconsistent.12,15 Recently published research16 on cerebral infarction also did not find a correlation between the distance of craniectomy from the midline and hydrocephalus. Thus, there was still no conclusive evidence on the impact of the distance from the midline on hydrocephalus. In order to precisely determine this clinically relevant question pertaining to everyday neurosurgical practice, we conducted this systematic review and meta-analysis.
This meta-analysis showed that existing research could not provide enough evidence for a relationship between the distance of craniectomy from the midline and hydrocephalus. Thus, this study aimed at presenting the yielded results, providing references for future studies, and suggesting future large, well-conducted, randomized clinical trials to clarify this issue.
Our review has several limitations. First, the included studies are limited, and no high quality randomized control trail was found. In addition, 2 of the articles were published by one author, which might affect the meta-analysis results. Second, we included only historical cohort studies, and this type of observational study is prone to selection, performance, attrition, and detection bias. Third, the primary diseases of the included studies differed, which might introduce confounding factors. These issues weakened the strength of the analysis, although some studies were adjusted for bias. Finally, 3 studies had small populations, which may result in an over- or under-estimation of the effect.
In conclusion, the relationship between the distance of craniectomy from the midline and hydrocephalus after DC is still inconclusive. Available evidence is insufficient and well-conducted randomized clinical trials are required to verify this situation.
Footnotes
Disclosure
This work was supported by the Chinese Natural Science Foundation (NO. 81000027). No potential conflicts of interest relevant to this article were reported and the study was not supported by any drug company.
- Received August 25, 2015.
- Accepted October 28, 2015.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.