


Abstract
Objective: To study the safety and efficacy of an innovative device using distraction-based magnetically controlled growing rods (MCGR) for the treatment of pediatric scoliosis.
Methods: This is an evidence-based systematic review of literature for the surgical management of patients with pediatric scoliosis using MCGR technique. Six clinical studies regarding the use of MCGR were included in this review, with a total of 68 patients, and mean age of 8.38 years. The dual-rod (DR) technique of rod construct with MCGR was used in 33.85% and the single-rod (SR) in 66.15% of the patients.
Results: The mean preoperative main coronal curve for the DR was 65.9°, and for the SR was 69.6° (p>0.05). At the latest follow-up, it was 36.8° for DR and 43.0° for SR (p<0.05). The mean preoperative T1-S1 spinal length was 298.7 mm for the DR and 303.5 mm for the SR group (p<0.05). According to the latest follow-up, using the DR construct, the spinal length increased to 347 mm with 13.92% of total lengthening; and using the SR construct, the average lengthening was 339 mm, with 10.48% of total lengthening (p<0.05). Postoperative complications were similar, 25% in DR and 31.57% in the SR group (p>0.05).
Conclusion: Level IV of medical evidence supports the use of MCGR as a safe and effective alternative for the treatment of severe pediatric scoliosis. Recommendation Grade C supports the role of MCGR with DR construct as an option to achieve a better correction of the scoliotic curve and to maximize the postoperative T1-S1 spinal length.
Chronologically, pediatric idiopathic scoliosis can be categorized on the basis of age of the patient at first identification of the deformity: infantile (0-2 years and 11 months), juvenile (3-9 years and 11 months), and adolescent (10-17 years, and 11 months),1,2 or as early (0-5 years-old) and late-onset scoliosis (>5 years-old), which does not only includes idiopathic scoliosis, but also those children with neuromuscular, congenital, or syndromic scoliosis.3,4 Pathological classifications relate to the main system or tissue affected by the underlying pathology, such as congenital scoliosis, which affect the skeletal elements of the spine, neuromuscular scoliosis, related to general neurological and/or muscular disorders, and idiopathic scoliosis, where there is no clear underlying problem which might cause the curvature.5,6 Progressive spinal deformity in early life presents significant health risks for the child and a challenge to the treating surgeon.7-9 Non-operative treatment includes casting and orthotic treatment, and can be indicated for early-onset scoliosis with curves from 25-35° until 40-50°, usually requiring it until skeletal and spinal maturity. This treatment, however, can deform the immature thorax and cause subsequent pulmonary complication, pressure sores, among others, and maybe ineffective to control the curve progression.10,11 When the deformity is progressive and severe (>40-50°), surgical treatment is often indicated. Spinal fusion, if undertaken before growth is complete, results in shortening of the trunk, arrested pulmonary development, severe respiratory compromise, and poor cosmetic appearance.12-14 The gold standard for surgical treatment of scoliosis in young non-skeletally mature children has been the traditional growing rod (TGR) procedure. This technique requires repeated lengthening every 6 months, with the patient anesthetized in the operating theatre undergoing an invasive procedure with the accompanying risks. This approach can control the progression of the curve and gradually straighten the spine, allowing the child’s spine to grow until definitive correction can be made when the patient nears skeletal maturity after the age of 11-13 years of age. However, this technique requires the invasiveness of repeated distractions, with associated anesthetic and surgical risks.9,10,15-17 The TGR is also associated with many socioeconomic drawbacks, like costs of the repeated operations, miss of school time by the children, and time off work by the parents.18-20
A new device using distraction-based magnetically controlled growing rods (MCGR) was developed to treat selected cases of severe pediatric scoliosis, to avoid such repeated surgeries and associated deleterious consequences for the patient and their families. Preliminary results indicated MCGR was safe and provided adequate distraction similar to TGR technique, and can be used as dual-rod (DR) or single-rod (SR) technique of rod construct.13,15,17,21-24 As this is a relatively new technique, figures were added to illustrate a case in which the magnetic rods were implanted (Figures 1-4). Our aim was to present an evidence-based systematic review of the literature for the surgical management of patients with pediatric scoliosis using this relatively new MCGR technique.

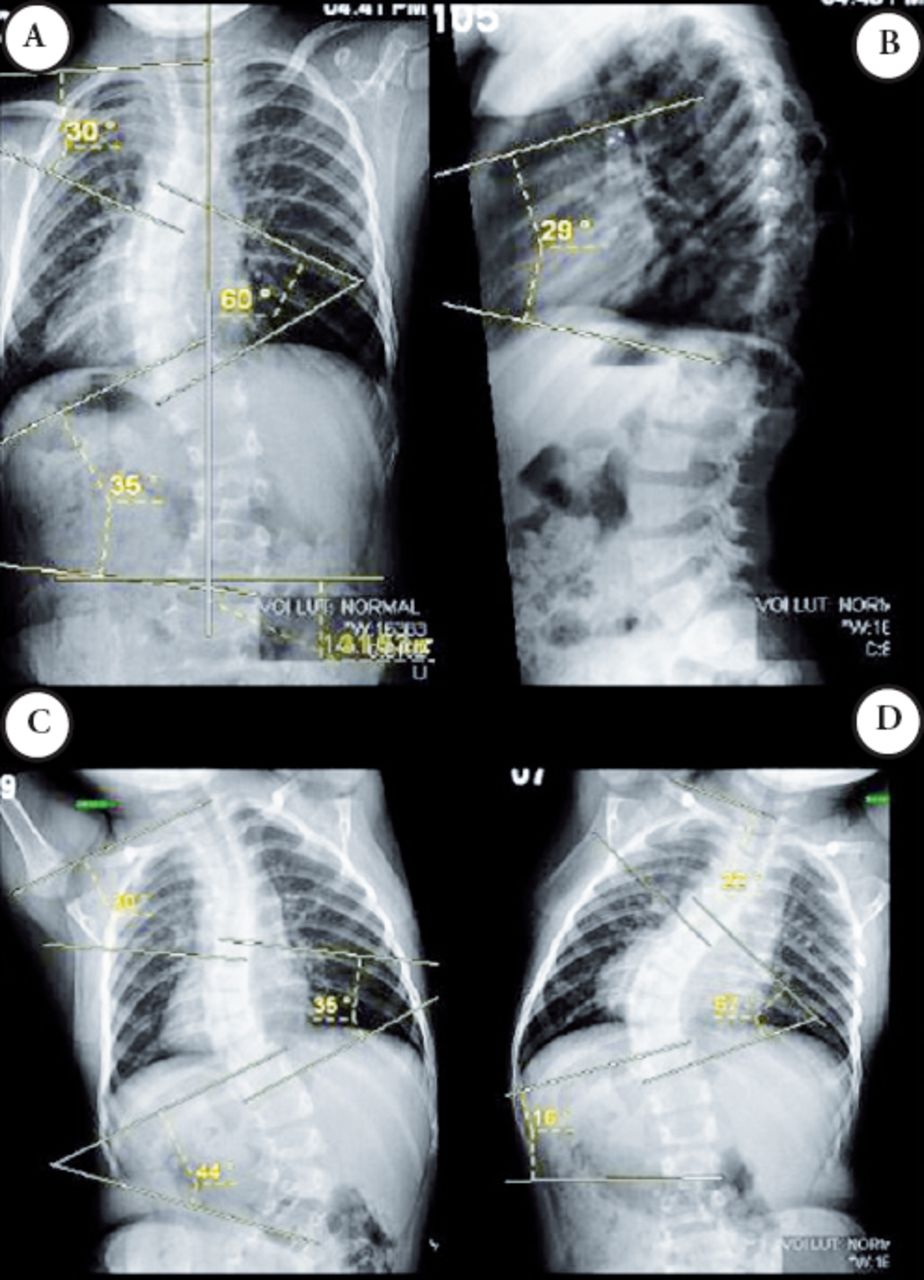
Scoliogram of a 3-years and 3 months-old girl with severe idiopathic early-onset scoliosis, progressive and non-responsive to conservative treatment: A) Preoperative standing PA scoliogram; B) standing lateral scoliogram; C) Preoperative left side bending film (PA); and D) right side bending film (PA). PA - posteroanterior

Surgical view of a posterior thoracolumbar spine approach for the implantation of the pedicle screws and magnetic rods (1 incision at high thoracic and another at lumbar region) in the same patient, which x-ray was presented before with severe scoliosis.

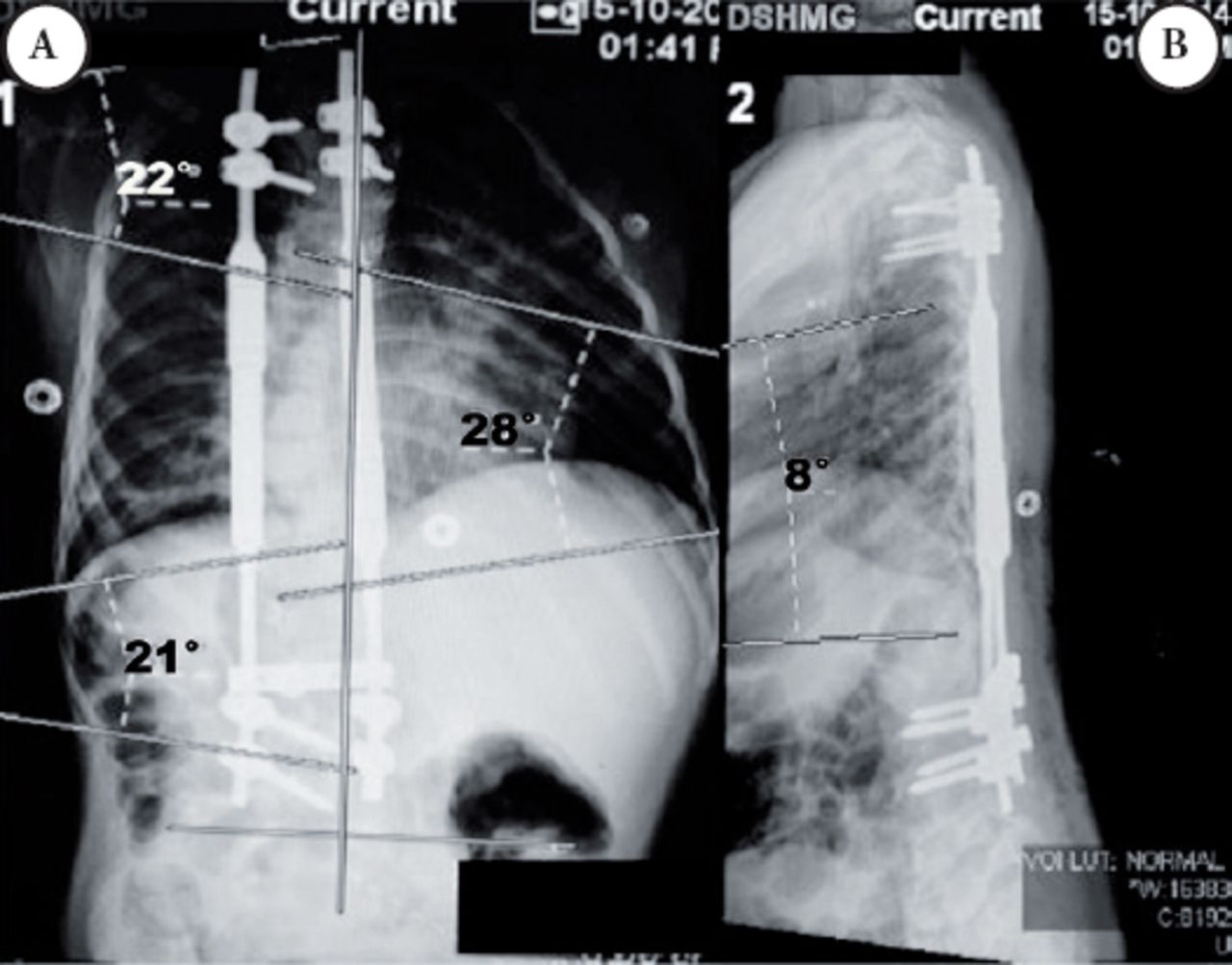
Scoliogram of the same 3 year-old girl at first postoperative day: A) standing posteroanterior spinal x-ray; and B) standing lateral.

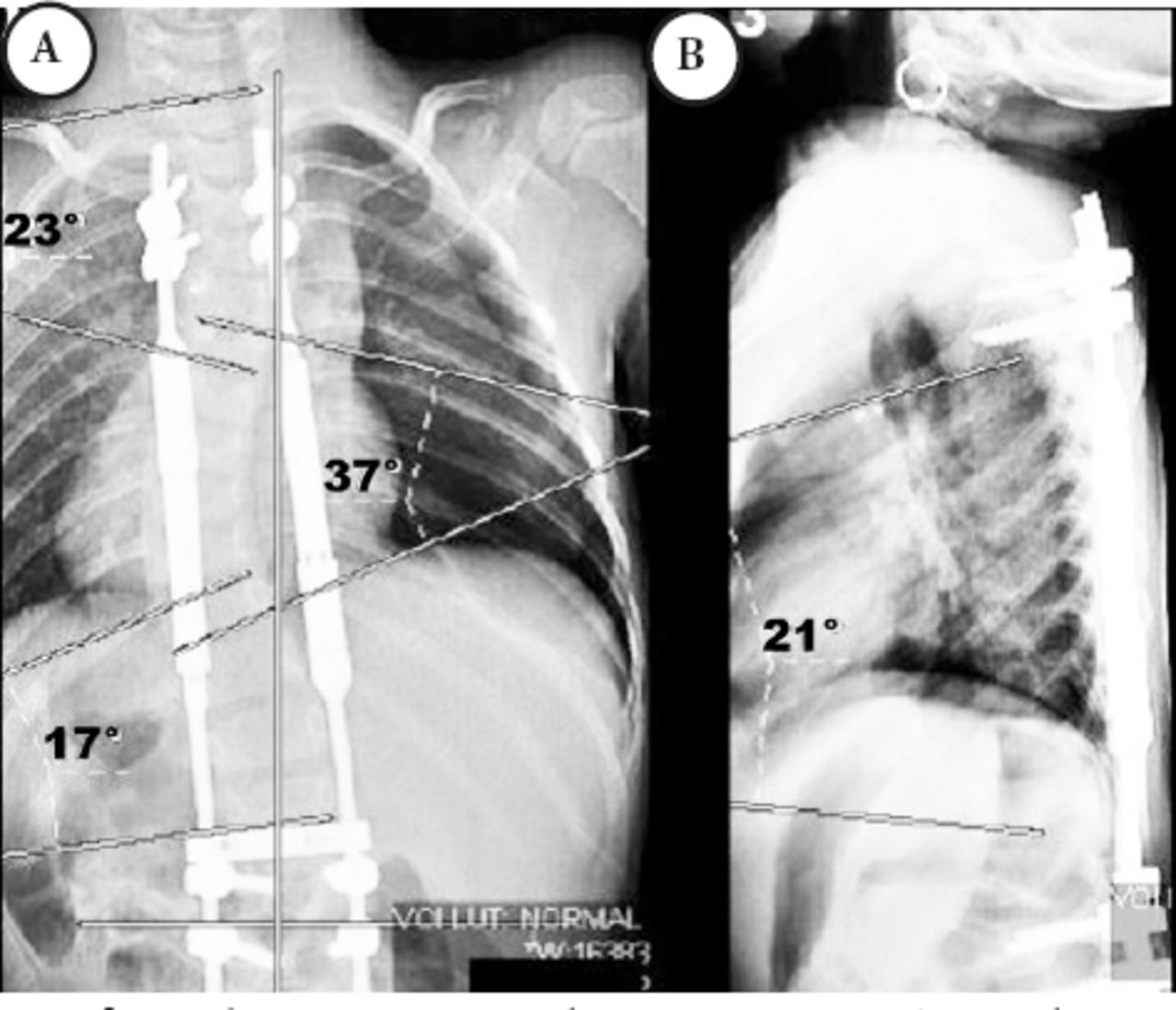
Scoliogram at 2 months postoperative: A) Spinal x-ray after the first distraction standing posteroanterior; and B) standing lateral.
Methods
An evidence-based systematic review of literature for the surgical management of patients with pediatric scoliosis with MCGR technique was performed, using the PubMed (indexed for MEDLINE), limited to articles regarding pediatric scoliosis in English-language, sampling only human-children (from birth to 18 years), from all the previous publication until the present (February 2015).25 The following main search terms were used: “pediatric scoliosis” (1,067 papers); “early-onset scoliosis” (150); “scoliosis AND magnetic rods” (9); “magnetic growing rod” (6); “adolescent scoliosis AND magnetic rods” (4); “magnetically controlled growing rods” (4); “early-onset scoliosis AND magnetic growing rod” (5).
Reviewed case series, case reports or cohort studies describing patients with pediatric scoliosis submitted to surgical management with MCGR were pulled and reviewed. Papers not concerned with the clinical or therapeutic aspects using this system were excluded. Relevant socio-demographic data, preoperative and postoperative films, surgical technique, complications of the treatment, and patient outcomes were collected, analyzed, and discussed. Descriptive statistics were compiled when appropriate.
Statistical analysis
Preoperative, immediate postoperative, and last follow-up outcomes (Cobb angle, spinal length, mean distraction length, among others) were averaged and standard deviations calculated over the 6 studies, weighting appropriately with the respective sample sizes in order to arrive at overall figures. This was also the case for the complication rates. Statistical comparisons of the outcomes were evaluated separately for DR and SR appliances. Differences between the 2 were evaluated with a “t-test”. Statistical comparison of the complication rates between DR, and SR were carried out with Fisher’s Exact Test.
Results
A total of 7 articles met the initial inclusion criteria and were fully reviewed.13,15,17,21-24 After reviewing those papers, one article was excluded, as it describes a different and not yet approved model of magnetic growing rod (GR), the custom made “Phenix rod” (Phenix Medical, Paris, France).21 The other 6 remaining papers described the use of the same equipment, the MCGR called: MAGEC system™ (Ellipse Technology, Irvine, CA, US), and for this reason, it was decided to include only those cases to make a more homogeneous comparison.13,15,17,22-24 Six published papers using the MCGR (MAGEC™ Ellipse Technology, Irvine, CA, USA) were included,13,15,17,22-24 total of 68 patients, and mean of 11.33 patients/study (1-34). The mean age of the patients was 8.63 years (3-14 yr.-old), 30 (44.11%) were male and 36 (52.94%) were females, with a male/female ratio of 0.83. According to the pathological classification of the scoliosis presented,5,6 there were 26/68 (38.23%) idiopathic, 36/68 (52.94%) neuromuscular, and 6/68 (8.82%) of congenital subtype (Tables 1 and 2). This review13,15,17,22-24 demonstrated that the dual-rod (DR) technique of rod construct was used in 43/65 (66.15%), and the single-rod (SR) in 22/65 (33.84%) of the patients, among those cases where the construct was specified. The mean interval between the distractions was of 55.33 days (1-135), mean of 3 mm (1.5-4.5) of distraction per episode. The mean preoperative main coronal curve (scoliogram) for the patients submitted to DR construct was 65° and for the SR was 69.6° (p=0.1209). The immediate postoperative curve was 44.9° (37.64% of correction) for the DR group and 47.8° (31.33% of correction) for the SR group (p=0.0348). The latest follow-up postoperative curve was 36.8° (44.16% of final correction) for DR and 43° (38.22% of final correction) for the SR (p=0.0007). The mean preoperative T1-S1 spinal length was 298.7 mm for the DR group, and 303.5 mm for the SR group (p=0.0052). According to the latest follow-up, using the DR construct, the spinal length increased to 347 mm, with 13.92% of total lengthening; and using the SR construct, the average lengthening was 339 mm, with 10.48% of total lengthening (p=0.0042) (Table 2).
Descriptive summary of all included studies regarding MCGR for severe pediatric scoliosis.
Quantitative summary of the papers related to magnetically controlled growing rod for severe pediatric scoliosis.
Postoperative complications occurred in 30.88% (21/68) of the patients, being 25% in DR and 31.57% in the SR group (p=0.7516) according to this review.13,15,17,22-24 Among those, prominent implant occurred in 8.33% of the patients who had DR construct, and none at the SR group (p=0.5437); wound infection in 2.77% of DR and 10.52% of SR (p=0.2716); loss of distraction in 8.33% of DR and 10.52% of SR (p=1.0000); rod breakage in 2.77% and 10.52% of SR (p=0.2716); implant pull-out in 2.77% and none at the SR group (p=1.0000) (Table 2).
Discussion
The natural history of progressive early-onset scoliosis (EOS) is usually unfavorable, due to rapid progress causing cosmetic disfigurement, significant cardio-pulmonary insufficiency, and poor prognosis.15,26,27 Significant progression of these curves may be associated with life-threatening health risks.7-9 Pulmonary development is not complete at birth and thoracic deformity caused by scoliosis may adversely affect lung maturation up to the age of 8.28 The deleterious effect of scoliosis on the developing lung is to inhibit the growth of both alveoli and pulmonary arterioles. This incomplete maturation of the lung and pulmonary vasculature is the primary cause of the ventilation defect seen in patients with EOS.12 The growth of the spine and thoracic cage in children varies significantly from birth to the onset of adulthood. The T1-S1 segment grows approximately 100 mm during the first 5 years of life (1.66 mm/month), approximately 50 mm between ages 5 and 10 (0.83 mm/month), and approximately 100 mm between age 10 and skeletal maturity (1.5 mm/month). Therefore, it is very important for a surgeon to consider the state of skeletal maturity and the amount of growth remaining in the spinal segment to be fused.29,30
The proper management of EOS remains challenging since therapeutic approach aims at reducing and controlling the spinal curvature while maintaining growth of the spinal column and thorax. The TGR technique with repeated open distractions was considered the main treatment for progressive and severe EOS until the definitive spinal fusion could be performed around 11-13 years of age.9,10,15-17 Non-fusion instrumented surgery reduces the curvature and maintains the correction by repetitive distraction surgeries, allowing for spinal and indirect pulmonary growth. Although still considered an effective technique for the management of EOS, TGR can lead to many surgical and anesthetic complications, potentially affecting the quality of life of those children.24,27,31
One of the major disadvantages of the TGR is the requirement for repeated surgical procedures to lengthen the rods as the child grows. Considering an average of rod lengthening at every 6 months, a child can be submitted to approximately 15 surgeries during their GR treatment. In addition to the surgical and anesthetic morbidity, the patient and the family must take significant time off school and work, besides possible psychological disturbance.17,19,32
Bess et al19 studied 140 patients with EOS, submitted to 897 TGR procedures. The mean age at the initial surgery was 6 years, and mean duration of follow-up was 5 years. At least one complication happened in 58% of the patients, being 27% of SR group because of implant complications, compared with 10% of the DR group. Among those patients with subcutaneous rod, 26% had wound complications compared with 10% with submuscular rod. The patients with subcutaneous DR had more wound complications, more prominent implants, and more unplanned surgical procedures than did those with submuscular DR construct. The risk of complications occurring during the treatment period decreased by 13% for each year of increased patient age at the initiation of treatment, and increased by 24% for each additional surgical procedure performed.
The concept of a remote magnet to drive force for a GR system and promote correction of scoliosis was suggested by Takaso et al33 in 1998. Other authors reported that a magnetically expandable GR system can be used for distraction between ribs, vertebra, and pelvis.34,35 Cheung et al13 reported the first clinical study using MCGR (MAGEC®, Ellipse Technology, Irvine, CA, USA) in 2012. They described the 2 years follow-up of 2 patients with severe scoliosis, and shorter follow-up of other 3, where the preliminary clinical results showed evidence of its health-care benefits, supporting its role as an alternative to the TGR. The MCGR was able to correct spinal curvature and encourage normal spinal growth with a non-invasive outpatient distraction method. Akbarnia et al24 reported that the mean correction of scoliosis was 43% after initial MCGR and improved to 48% at final follow-up, comparable with the reported TGR studies,36-38 and similar to our review with MCGR, which showed 45% of mean curve correction. They concluded that the use of MCGR seems to be effective in correcting and maintaining scoliosis curve correction.24
Charroin et al20 published their study regarding the costs of the management of EOS in France, comparing the TGR with MCGR technique. The estimated direct costs of TGR in 4 years were €49,067 (USD 61,380) and €42,752 (USD 53,477) for MCGR strategies. In the cases of the TGR, costs were mainly represented by hospital stay expenses (83.9%) whereas in the other, the cost of MCGR contributed to 59.5% of the total amount. This study showed that MCGR is a recent and promising innovation in the management of severe EOS. Therefore, MCGR can minimize the costs of repeated surgical-anesthetic procedures and hospital admissions. Rolton et al39 also evaluated the costs of all aspects of each treatment group and compared the differences between those 2 rods in treating EOS over a projected 5 year period. There was a cost saving of over £8,000 (USD 12,190) per patient in favor of the MCGR. In Saudi Arabia and Gulf Region, the average price of MCGR with SR construct (MAGEC™; Ellipse Technologies, Irvine, CA, USA) was approximately SAR 45,000 (USD 11,995) and with DR construct was approximately SAR 72,000 (USD 19,192), while the cost of the TGR with SR construct (Pediatric Legacy Spinal Deformity System®, Medtronic Sofamor Danek, Memphis, TN, USA) was approximately SAR 15,000 (USD 3,997) and with DR construct plus connector was approximately SAR 30,000 (USD 7,995), not including the additional costs (hospital and admission fees, medical personal, among others). If the efficacy and safety of MCGR is proven in long term studies, the cost-effectiveness of this new technique may justify its use for cases of severe pediatric scoliosis.20,38,39
An evidence-based review conducted by the Medical Technologies Advisory Committee at the National Institute for Health and Care Excellence (NICE), in England, provided guidance regarding the use of the MAGEC system for pediatric scoliosis.40 The provisional recommendations supported the use of the MCGR for children aged between 2 and 11 years, with progressive scoliosis unresponsive to conservative treatment, to avoid repeated surgical procedures for rod lengthening. The study also estimated that using the MAGEC system is cost-saving compared with TGR from about 3 years after the initial procedure. The estimated cost-saving per patient after 6 years is approximately £12,077 (USD 18,946).40,41 The literature on TGR has shown that DR are more advantageous than SR in terms of lower rate of rod fracture, better rate of deformity correction, and higher rate of spinal growth.36,37 In this systematic review using MCGR,13,15,17,22-24 the mean correction of the main scoliosis and spinal growth at the latest follow-up was significant and also more advantageous using the DR construct (Table 2).
Using the TGR technique, the usual interval between distractions is between 6 to 9 months; however, distraction in MCGR can be carried out more frequently depending on the patient’s age, growth potential, curve flexibility, and diagnosis.24,42 In this systematic review of cases using MCGR,13,15,17,22-24 the mean interval between distractions was 55.33 days, and mean of 3 mm of distraction per episode (Table 2).
Akbarnia et al16 reported that the average T1-S1 length increase was 12.1 mm per year for patients with EOS who underwent DR surgery and were followed up for at least 24 months. Olgun et al43 found that the growth of the vertebral body heights within the instrumented levels (7.0±2.9 mm) was significantly more than those outside the instrumentation levels (5.2±3.4 mm) and concluded that GR had stimulated the growth of the vertebral height. Cheung et al13 using the MCGR, showed that the actual and predicted rod distractions were closely comparable. In this more recent study of Akbarnia et al,24 the average monthly T1-S1 growth was comparable, 3.09 mm using DR and 1.27 mm using SR construct, yet slightly higher than the TGR technique, and they supposed that this difference could be because of more frequent remote controlled distractions, especially during the more rapid phase of growth. In our study,13,15,17,22-24 the mean postoperative T1-S1 spinal length increased more with the DR in comparison with the SR technique, being 13.92% with the DR (48.3 mm; 2.8 mm/mo.) and 10.48% with the SR (38.8 mm; 2.29 mm/mo.) (p=0.0042) (Table 1 & 2).
Postoperative complications occurred in 21/68 (30.88%) of the patients, being 25% in DR, and 31.57% in the SR group, but the difference between both in groups was not statistically significant (p=0.7516). Among those, prominent implant occurred in 8.33% of patients who had DR construct, and none at the SR group (p=0.5437); wound infection in 2.77% of DR and 10.52% of SR (p=0.2716); loss of distraction in 8.33% of DR and 10.52% of SR (p=1.0000); rod breakage in 2.77% and 10.52% of SR (p=0.2716); implant pull-out in 2.77% and none at the SR group (p=1.0000) (Table 2).
There were some limitations to this work. As a retrospective study of a relatively new medical topic, there was potential selection bias, limited comparable results, small number of published studies and cases, and there was lack of a standardized way to describe the main results for most of the papers. Overall, the systematic review of the literature suggests that MCGR is a safe and effective alternative to the TGR system in the treatment of progressive EOS, with the avoidance of repeated surgical lengthening.13,15,17,22-24
Classification of evidence
Level IV of Medical Evidence (case series) for Therapeutic Study44 was provided with this systematic review supporting the role of MCGR in the treatment of patients with severe pediatric scoliosis, as a safe and effective technique.13,15,17,22-24 Level IV of Medical Evidence44 was provided with this systematic review supporting the role of MCGR with DR construct in the management of severe pediatric scoliosis, in order to achieve a better correction of the scoliotic curve and to maximize the postoperative T1-S1 spinal length.13,15,17,22-24
Recommendation Grade C (based on single Level II study or multiple Level IV or V studies)44 can be formulated to support the use of MCGR in patients with severe pediatric scoliosis, as an option to reduce and control the spinal curvature while maintaining growth of the spine, as an alternative to the TGR system without inducing major morbidity.13,15,17,22-24
Recommendation Grade C44 supports the use of MCGR as an option in patients with severe pediatric scoliosis, to achieve better correction of the scoliotic curve and to increase postoperative T1-S1 spinal lengthening using DR construct.13,15,17,22-24
In conclusion, this was an evidence-based systematic review of the literature regarding pediatric scoliosis treated with MCGR, limited to the previously established criteria. According to this study, the MCGR could be a safe and effective alternative technique to the traditional growing rods system for patients with severe pediatric scoliosis. The use of MCGR is as an option to reduce and control the spinal curvature while maintaining growth of the spine, without inducing major morbidity, with better correction of the scoliosis, and increased postoperative T1-S1 spinal lengthening using double-rod construct technique.13,15,17,22-24
Footnotes
Disclosure
The authors disclose no affiliation or financial involvement with organizations or entities with a direct financial interest in the subject matter or materials discussed in the manuscript. No funding was received for this work from any organization.
- Received April 15, 2015.
- Accepted October 7, 2015.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.