


Abstract
Objective: To determine the pattern, management, and outcome of headaches among patients treated at Outpatient Neurology Clinic.
Methods: A retrospective study was conducted at the Out-Patient Neurology Clinic of the Butare University Teaching Hospital, University of Rwanda, Butare, Rwanda between February and May 2015. We extracted the demographic data, headache characteristics, and associated conditions, prior pain-relieving medication use, waiting time before consultation, the results of paraclinical investigations, final diagnosis according to the International Classification of Headache Disorders, management, and 3-month clinical outcome from the medical records of all patients who consulted for headache over 36-month period. Epi Data and Statistical package for Social sciences software version 21.0 (SPSS Inc, Chicago, IL, USA) software were used for data processing.
Results: Headache disorders represent a quarter of all neurological consultations. Patients were predominantly female (67%) and young (78% <45 years old). One-third (34%) presented with chronic tension-type headache. Neuroimaging demonstrated an abnormality in a significant minority (14%). Amitriptyline was the most commonly used drug (60%) in management. Forty percent of those patients followed for 3 months did not experience any clinical improvement.
Conclusion: Headache is among the most common medical complaints in the Outpatient Neurology Clinic, with a wide array of underlying diagnoses, and a significant yield on neuroimaging. A significant proportion of those suffering from headache disorders have poor short-term outcomes. Novel approaches, such as headache support groups and alternative pharmacological agents, should be investigated for these patients.
Headache is one of the most common reasons for neurological presentation in sub-Saharan Africa being responsible for 31.9% of visits to Outpatient Neurology Clinics.1,2 According to the World Health Organization, 1.7-4% of the adult population of the world have headaches on 15 or more days every month3 suggesting that up to 170 million adults worldwide have headaches fitting chronic tension-type criteria, according to the International Classification of Headache Disorders.4 Headache disorders impose a major burden on their sufferers, with intensity ranging from impaired quality of life and financial cost to severe associated illnesses, such as depression, which is 3 times more common in people with migraine or severe headaches than in healthy individuals.3,5-7 While headache disorders are a major public health concern in sub-Saharan Africa,8 there is scarce literature on neurological diseases in this region.2 Very little study of the epidemiology of headache in tropical countries has been conducted,9 and there are also un known published data on headache disorders in Rwanda. The aim of this baseline study was therefore, to determine the pattern, management, and outcome of headaches among patients treated at the Outpatient Neurology Clinic of the Butare University Teaching Hospital, Butare, Rwanda associated with the University of Rwanda, to reduce this knowledge deficit and provide data on where the available neurological resources should best be directed.
Methods
Between February and May 2015, medical records of all patients who consulted for headache from June 2011 to May 2014 (a 36-month period) were retrospectively collected by a senior consultant neuropsychiatrist involved in patient’s care at the Outpatient Neurology Clinic of the Butare University Teaching Hospital (BUTH), University of Rwanda, Butare, Rwanda. Patients who consulted for any complaint other than headache were excluded from the study. The following data were extracted from these patients’medical records: demographic information, pain-relieving medication use prior to visit the clinic, waiting time before consultation, headache classification and associated conditions according to the international classification of headache disorders.4 The paraclinical investigations results, final diagnosis, management, and 3-month clinical outcome (in terms of severity, frequency, and duration of headache) were also recorded where available. After extraction and interpretation according to the international classification of headache disorders,4 data were recorded using a predetermined questionnaire (one questionnaire per patient). In the second time, each questionnaire was encoded in a database using EpiData software. After checking of data, they were analyzed using Statistical package for social science software verision 21.0 (SPSS Inc, Chicago, IL, USA). Association between variables was tested using the Pearson chi-square test, with a p-value of <0.05 being considered statistically significant. This study was approved by the BUTH Ethics Committee (RC/UTH/B/18/2015).
Results
Over the period of 36 months, 3966 consultations were reported at the Neurology Clinic of the BUTH / UR among which 1023 (25.8%) for headache. These 1023 visits for headache concerned a total of 287 patients.
Baseline characteristics of headache sufferers
The majority of patients were female (Table 1). Female gender was also similarly represented in the primary headache (109/166, 65.7%) and in the one thought to be attributed to other medical conditions (83/121, 68.6%) groups. Two hundred and twenty-four patients (78%) were younger than 45 years with a peak of 55.4% between 15 and 34 years. Students and farmers were the most common professions listed (Table 1). Only 8 (2.8%) patients had neurological deficit at presentation.
Baseline characteristics of headache sufferers. N=287
Headache classification
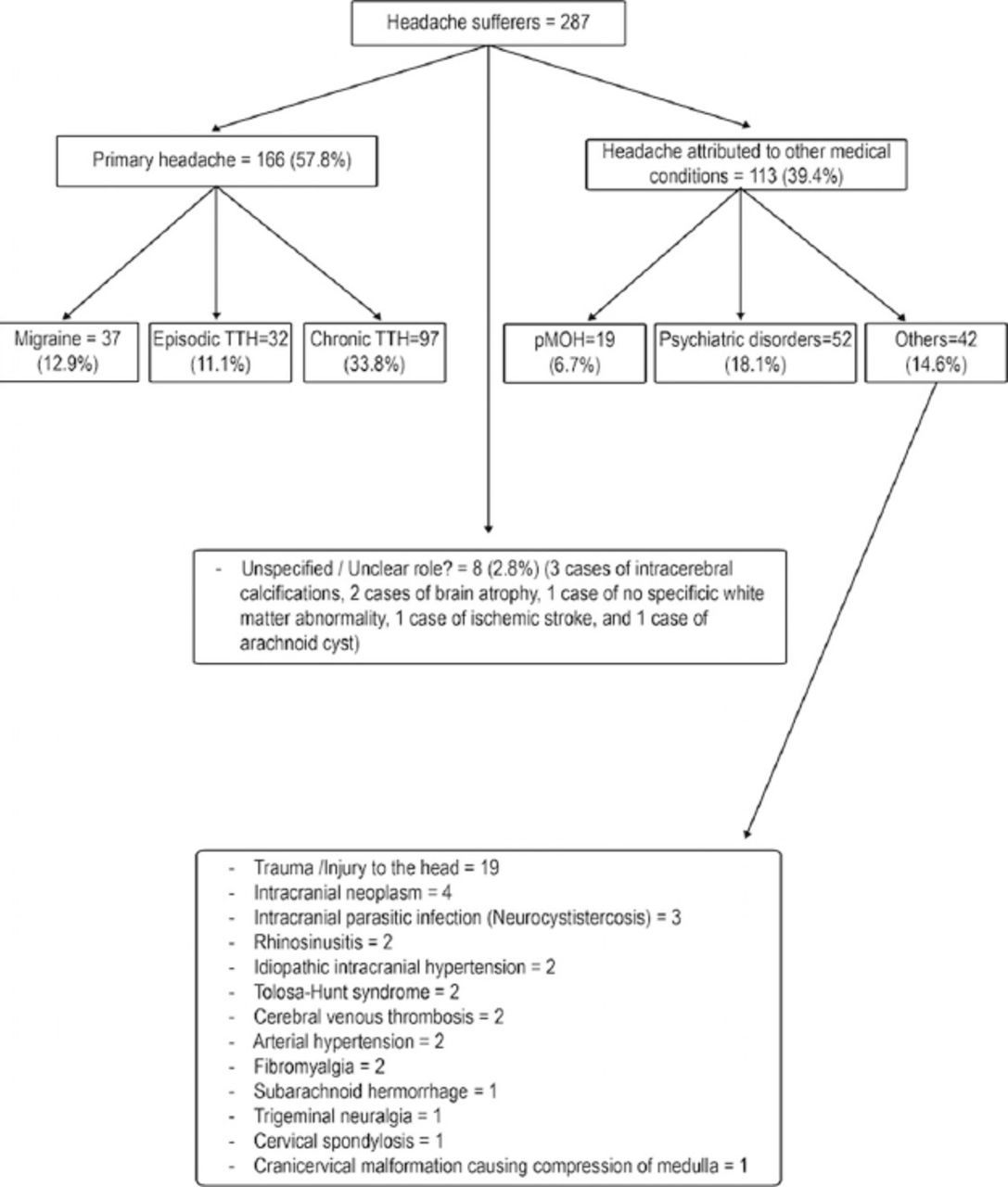
Chronic tension-type headache was 3 times more frequent than episodic one (Figure 1). Of the 37 (12.9%) patients with migraine, 25 (67.6%) were female. Nineteen (59.4%) of 32 patients with episodic TTH were female. It is the same for chronic TTH in which the female remains predominant: 65/97 (67%). Based on the international classification of headache disorders criteria,4 19 (6.6%) patients were thought to have head and/neck trauma-related headache (occurred for the first time within 7 days following the incriminated trauma) although brain imaging showed post traumatic injury in only one case (Figure 1). In 52 (18.1%) cases, headache was attributed to psychiatric disorders (persistent depressive disorders, post-stress traumatic disorders, and somatization: diagnosis based on personal evaluation, history-taking and, physical examinations). Of these, 29 (55.8%) were identified as “direct” 1994 Rwandan genocide victims. A statistical link was found between a diagnosis of “headache attributed to psychiatric disorders” and being a genocide victim (p=0.001). In 19 (6.7%) cases, headache was thought to be induced by the headache medication abuse (occurring at least 15 days per month associated with regular overuse of any headache medication on 15 days/month for at least 3 months prior to consultation). The term of probable medication overuse headache (pMOH) was preferred since it’s known that the diagnosing of MOH requires an individualized assessment of the patient’s medication and headache history.10 Among them, 12 (63.2%) were being treated (self-administration) with a combination of several drugs prior to consultation at neurology clinic while the remaining were on non-steroidal anti-inflammatory drugs (NSAID). Seven cases were attributed to non-vascular intracranial disorders, 4 cases of neoplasm, 2 cases of idiopathic intracranial hypertension and one case of craniocervical malformation, while 3 were attributed to intracranial infections (Figure 1). In 8 patients, it was not easy to conclude on the role that intracerebral calcifications (3 cases), cerebral atrophy (2 cases), ischemic stroke, arachnoid cyst, and non-specific abnormalities of white matter would have played in the onset and maintenance of headaches (Figure 1).
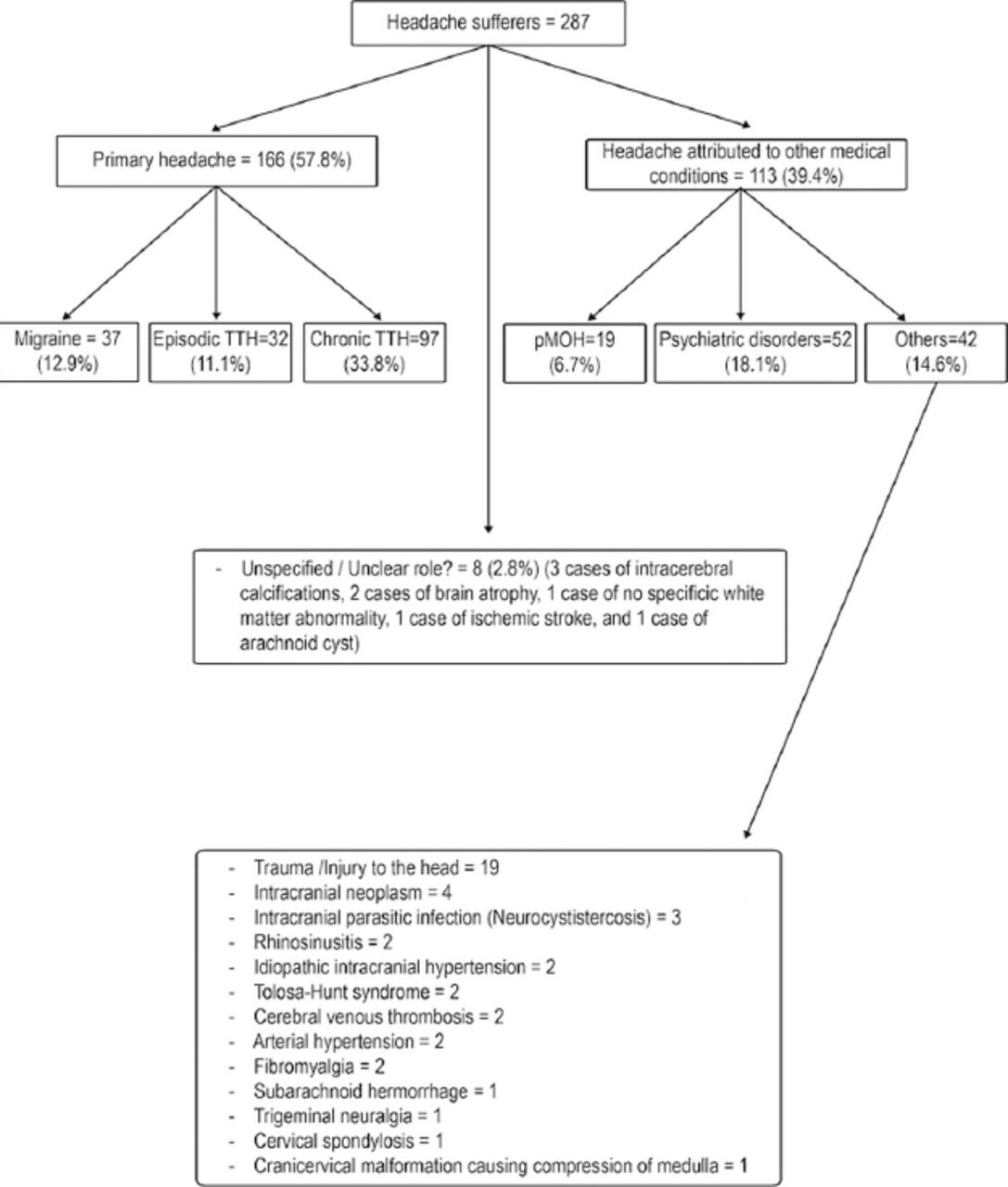
Headache classification.
Associated clinical circumstances
Most of the patients were not able to recall the exacerbating / alleviating factors, and symptoms associated with their headache. Concentration / being at school seemed to be the most common exacerbating factor. Rest / sleep were the most important alleviating factors. Psychological symptoms (irritability, lack of concentration, memory disturbances, and lack of sleep) were the most common associated factors.
Paraclinical investigations results
This study included many patients who underwent paraclinical investigations. Fundoscopy and eletroencephalography, when performed, were normal most of the time (Table 2). Mostly based on the presence of warning signs (sudden onset of headache, increased frequency, or severity of headache, papilledema, vomiting, previous head trauma, suspicion of an underlying medical condition, any other focal neurologic symptom or sign and patient being 50 years old or more), a brain CT scan was performed in 117 (40.8%) cases. It was abnormal in 16 (13.7%) cases and helped to diagnose 4 space occupying lesions (one arachnoid cyst, one subarachnoid hemorrhage, one pituitary adenoma, and one midbrain neoplasm), 3 cases of neurocysticercosis, 2 cases of generalized brain atrophy, 2 cases of unexplained calcified lesions, 2 cases of sinusitis, one case of cervical osteodegenerative process, one case of ischemic stroke, and one case of severe post-traumatic lesions. Brain MRI was performed in 14 (4.9%) cases. It was abnormal in 7 (50%) and helped to diagnose 2 cases of cerebral venous thrombosis, one case of pituitary macroadenoma, one case of right temporal lobe neoplasm, one case of a non-specific white matter abnormality, one case of intracerebral calcifications, and one case of a craniocervical malformation causing compression of medulla. Overall, 23 (8%) patients were found to have a possible pathological cause of their headache by CT scan or MRI. In all but 2 patients, standard laboratory tests (full blood count and erythrocyte sedimentation rate) were performed and were normal.
Paraclinical investigations results. N=287
Management and outcome
Among 230 patients requiring maintenance pharmacological treatment, amitriptyline (Agog Pharma, India) was the most used drug in 138 patients (60%). Forty six patients (20%) took clomipramine (Sigma -Tau, Rome, Italy) and 20 (8.7%) were put on fluoxetine (Lilly, France). The daily highest used dose for amitriptyline and clomipramine was 75 mg. Other drugs administered were maprotiline, carbamazepine (Novartis, Italy), propranolol (Sterop Group, Belgium), and gabapentin (Universal Corporation, Kikuyu, Kenya). In 15 patients, a benzodiazepine (Sterop Group, Belgium), was punctually administered in order to manage insomnia. Of all, 79 patients were put on abortive therapy for headache at least once during the follow-up period. Among them, 65 (86%) took ibuprofen (Agog Pharma, India) and 8 received paracetamol (Hebei Jiheng Group, China). More than half of the patients were being treated (self-administration medication, health centers or district hospitals) prior to consultation at our clinic (Table 2). For 73 (48.7%) of them a combination of several drugs was administered, 20 received NSAIDs in combination with opioid therapy, 8 received antidepressant including one in combination with NSAIDs, 2 were on opioid therapy. Unfortunately, remaining 47 patients were not able to recall the names of the drugs they consumed.
Of all, 132 (46%) patients were correctly and monthly monitored for a period of 3 months (Table 3). Of these, 79 (59.8%) experienced an improvement in their clinical condition (in terms of severity, frequency, and duration of attack). The 3-month period outcome was not associated neither with type headaches (primary or non-primary) (p=0.126) nor with the waiting time before consulting our neurological clinic (p=0.117).
Neurological examination results, management and outcome. N=287
Among the 37 with migraine, 17 were correctly followed for a 3-month period. All of them (100%) experienced an improvement in their clinical conditions although 12 of them continued to present less severe attacks. Among 32 suffering from episodic TTH, only 16 did not disappear from the out-patient neurology clinic, 10 (62.5%) of them experienced improvement in their clinical conditions although 9 of them continued to present less severe attacks. They were 35 out of 97 suffering from chronic TTH to be monitored over the same period, 18 of them (51.4%) experienced an improvement in their clinical conditions, although 13 of them continued to present less severe attacks.
Among 79 patients who presented with an improvement in their clinical condition, only 7 (8.9%) were direct victims of the 1994 Rwandan genocide. Among 53 patients who did not present an improvement of their clinical conditions, 15 (28.3%) were direct victims of the 1994 genocide. There was a statistical association between outcome and the fact of being or not 1994 direct genocide victim (p=0.003).
Discussion
The aim of this study was to determine the pattern, management and outcome of headaches among patients treated in our setting. Its results suggest that headache disorders represent the one-quarter of all neurological consultations. They affect especially females (66.9%) and the younger working-age group (78% being <45 years old). One-third (33.8%) is represented by chronic TTH, amitriptyline is the most used drug (60%) in their management, and almost 60% of patients available to follow-up experienced an improvement in their clinical condition. In our study, headache represents 25.8% of all neurological consultations. Our results are consistent with those from Cameroon where the percentage of 31.9% has been recently reported among all neurological admissions.2 This raises a serious concern considering the enormous burden that headache disorders may constitute in our settings in terms of absenteeism from work and school, health related expenses and comorbidities.
In our study, 78% headache suffers were <45 years. This result is consistent with previous studies11,12 reporting that headache disorders prevalence was higher in the age groups of 18-45 years in both genders and declined after the fourth decade. The high proportion of students in this study (33.4%) may partly be explained by the fact that BUTH is easily accessible to students as it is located in the university neighborhood. In addition and as discussed above, headache disorders afflict mostly young people.
As reported in previous almost all studies13-15 female predominance is seen in our study (female/male ratio 195/92=2, 1). The influence of oestrogens and progesterone on headaches after menarche and the greater propensity for females to seek medical attention for headaches are the most evocated reasons to explain this higher female prevalence.16
Our results suggest that overall, chronic headache represents 33.8% against 11.2% for the episodic one. It has been reported that the percentages of the adult population with an active headache disorder are 46% for headache in general, 11% for migraine, 42% for tension-type headache and 3% for chronic daily headache.17,18 According to the recently published data from Zambia, 19 migraine represents 22.9% in all population, 22.8% for tension-type headache and 11.5% for headache lasting more than 15 days per month. Our results can not be compared to the above overall figures because our study suffers from the selection bias inherent in a tertiary referral population. It only concerns patients presenting with headaches at out-patient clinic and not in the general population. It is expected that the patients who suffer the most frequent or persistent symptoms would be the most inclined to seek medical attention.
Our results suggest that overall, pMOH represent 6.7%. This result is consistent with what has been recently reported from Zambia: 7.1% (1-year prevalence).19 This similarity is curious since these 2 studies have different methodological approaches: population-based versus single-centered. This raises nevertheless, the issue of the burden of this type of headache in sub-Saharan Africa although there would be limits to comparing prevalence of MOH across studies and over time.20
Three cases were attributed to neurocysticercosis in this study. Indeed, a recent study21 has mentioned the high prevalence of cysticercosis in the area where this study was conducted. The decision as to when to undertake neuro-imaging is a complex one. Warning features (or “red flags”) in the history and on examination helped to target those who need neuroimaging investigations, but sometimes, investigations were carried out at the request of patients who could afford them. Thus, brain CT scan was performed in 40.8% of cases, and this helped to identify brain lesions as a potential cause of headache in 16 patients. The use of brain MRI helped to diagnose 2 cases of cerebral venous thrombosis, although the discovery of a single case of no specific white matter abnormality, 3 intracerebral calcifications, 2 brain atrophy, 1 ischemic stroke, and 1 arachnoid cyst with MRI and CT scan could be regarded as incidental.22 Overall, 23 (8%) patients were found to have a possible pathological cause of their headache by using neuroimaging. This result is close to that found by Locker et al: 13.4%.23 It is important to note that of 117 (40.8%) patients underwent computed tomography of the head; 101 (86.3%) were normal. This number exceeded the percentage (21.8%) of patients presenting with headache to the emergency department in the UK who underwent computed tomography,24 again probably due to the tertiary referral nature of this population. Ordering brain imaging should be based on painstaking history-taking and neurological examination to avoid needlessly wasting limited resources. In our study, 178 patients underwent fundoscopy; 173 (97.2%) were normal. One hundred forty eight patients underwent EEG; 141 (92.2%) were normal. These high rates of investigation with low yield raises the question of whether published standards are being complied with in the way subsequent investigations are ordered.24-26
Nearly 80% of patients required maintenance pharmacological treatment. In the Rwanda health system, patients first consult health centers (level 1) before being transferred to the district hospital level (level 2). The patient reaches the tertiary hospital only after being treated without improvement at the district hospital. Furthermore, the tertiary neurology clinic in which this study was conducted is the one of only 2 staffed by neurologists in the whole country. Thus, only selected patients are followed at this neurology clinic. This may help explain the high proportion of patient in whom prophylactic therapy was necessary. The tricyclic antidepressant amitriptyline plays an important role in the management of headache disorders.27-29 For migraine prophylaxis, it is thought to be more cost-effective than propranolol or topiramate.30 It was the most used drug in our clinic (60%) because of its affordability and availability. However, there was no improvement in the clinical condition in about 40% of patients. This raises the question of how to increase access to other alternatives therapies in our settings.31 Indeed, among 35 patients suffering from chronic TTH who had follow-up data available, 18 (51. 4%) experienced an improvement in their clinical conditions, although 13 continued to present less severe attacks. This result confirms the poor outcome that characterizes TTH.32 Benzodiazepine was used in 15 patients in order to treat insomnia. It is known that chronic tension-type headache has high prevalence of insomnia which can require medication.33 Although benzodiazepines (BZDs) play a role in the management of headache disorders,34 medical personnel should be aware about the risk of dependence and headache related to BZDs abuse.35
Association between stress and headache has been described.36 Some authors have noted a high prevalence of depression and posttraumatic stress disorders in post genocide Rwandan society.37-39 This context may help explain the poor outcome observed among patients who were direct victims of the 1994 genocide and perhaps also the high prevalence of chronic TTH.
Study limitations
Our study included patients presenting with headaches at out-patient clinic and not in the general population. Furthermore, it covered only a 36-month period. More than half (54%) of the patients included in this study were not available for follow-up after a 3-month period. It would be therefore risky to generalize its findings. Despite these limitations, these baseline results are however, very important as they concern the only Rwandan tertiary neurology service being fully functional during the period covered by the study.
In conclusion, the results of this study suggest that headache is prevalent in neurology clinic in Rwanda. It strikes especially female and the younger working-age group. Most neuroimaging investigations ordered were normal. Amitriptyline was widely used. A significant number of those suffering from headache disorders had poor outcome. It is therefore, essential to educate doctors about international classification headache disorders use, paraclinical investigations ordering, and pain killer’s prescription. Creating support group for those headache suffers could create an interesting alternative to pain killer therapy.
Footnotes
Disclosure
The authors declare no conflicting interests, support or funding from any drug company.
- Received October 4, 2015.
- Accepted February 17, 2016.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.