


Article Figures & Data
Figures
- Figure 1
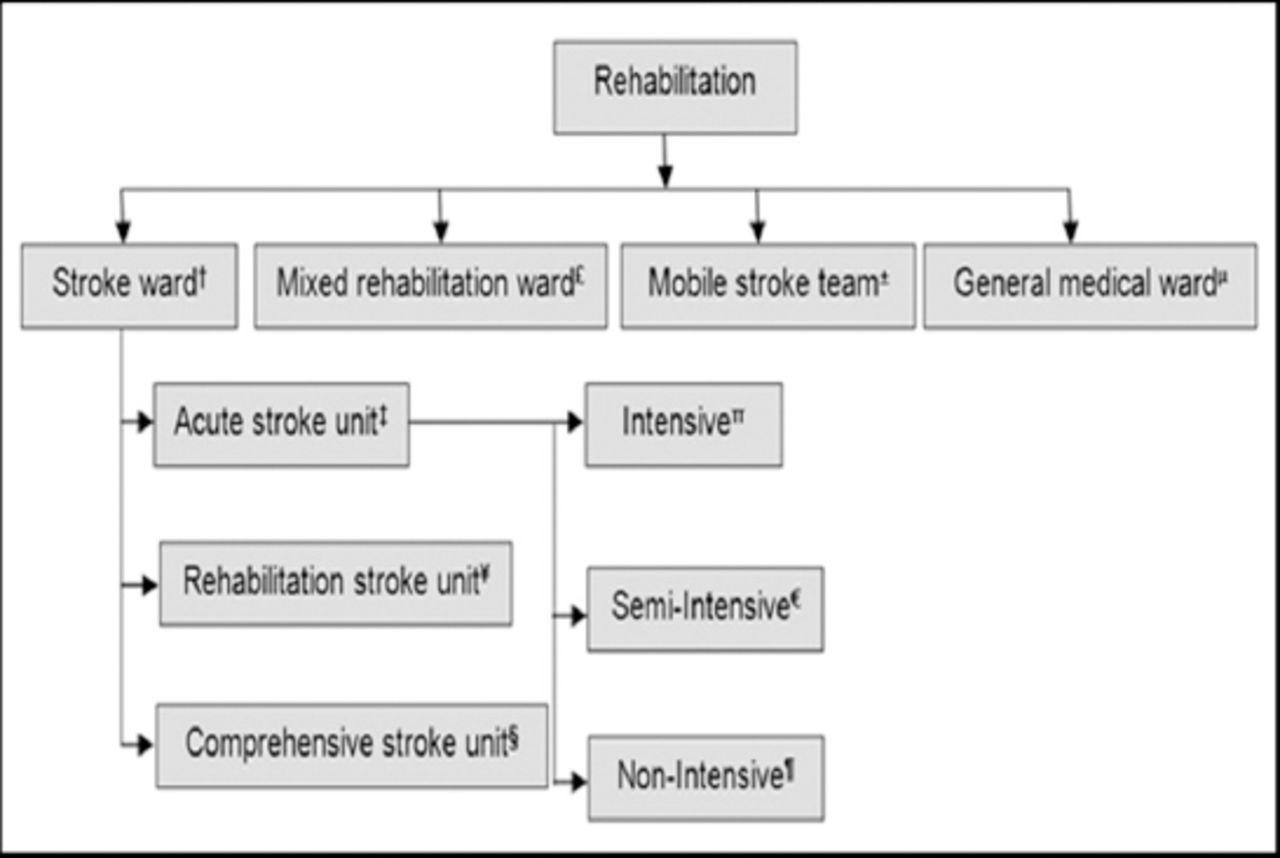
Elements of a stroke unit associated with improved outcome. †A multidisciplinary team including a specialist nursing staff. ‡Stroke patients are assessed in the acute care hospital by a physical therapist or rehabilitation physician who decides the level of mobility impairment and the capacity to endure treatment. Patients are discharged early within 7 days. πModel of consideration with constant checking, high medical attendant staff, and life support. €Model of consideration with constant checking, high medical attendant staff, yet no life support facilities. ¶Model with no high medical attendant staff or life support facilities. ¥A wide scope of therapeutic and rehabilitative services and settings that give consideration to patients admitted after intense administration in a hospital setting. Patients are accepted after a period of usually of 5 to 7 days or more. §Rehabilitation offered for at least several weeks if necessary. £A multidisciplinary group gives a non-specific rehabilitation service, not only watching over stroke patients. ±A multidisciplinary group (barring nursing staff) gives care in an assortment of settings. µAn intense medicinal or neurology ward without routine multidisciplinary information.
- Figure 2
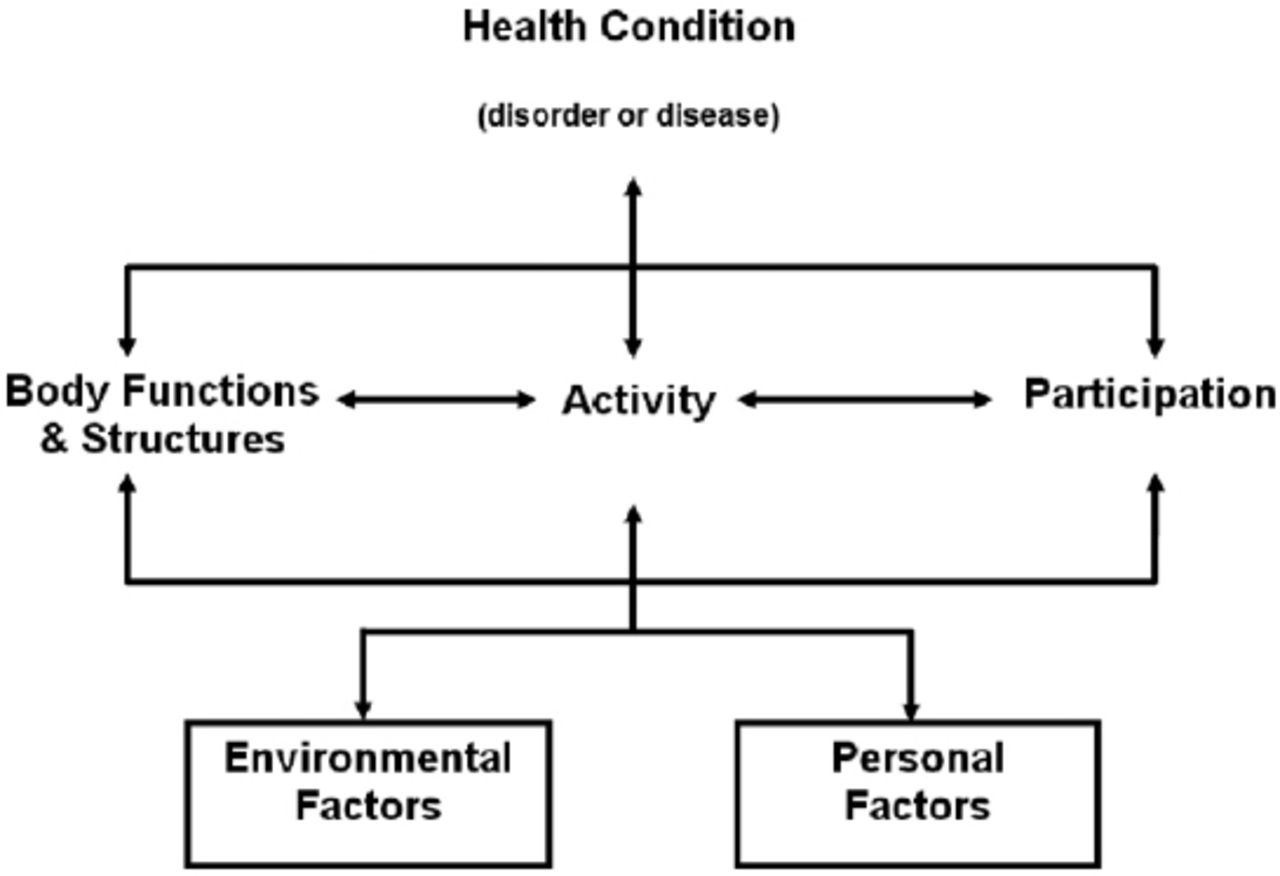
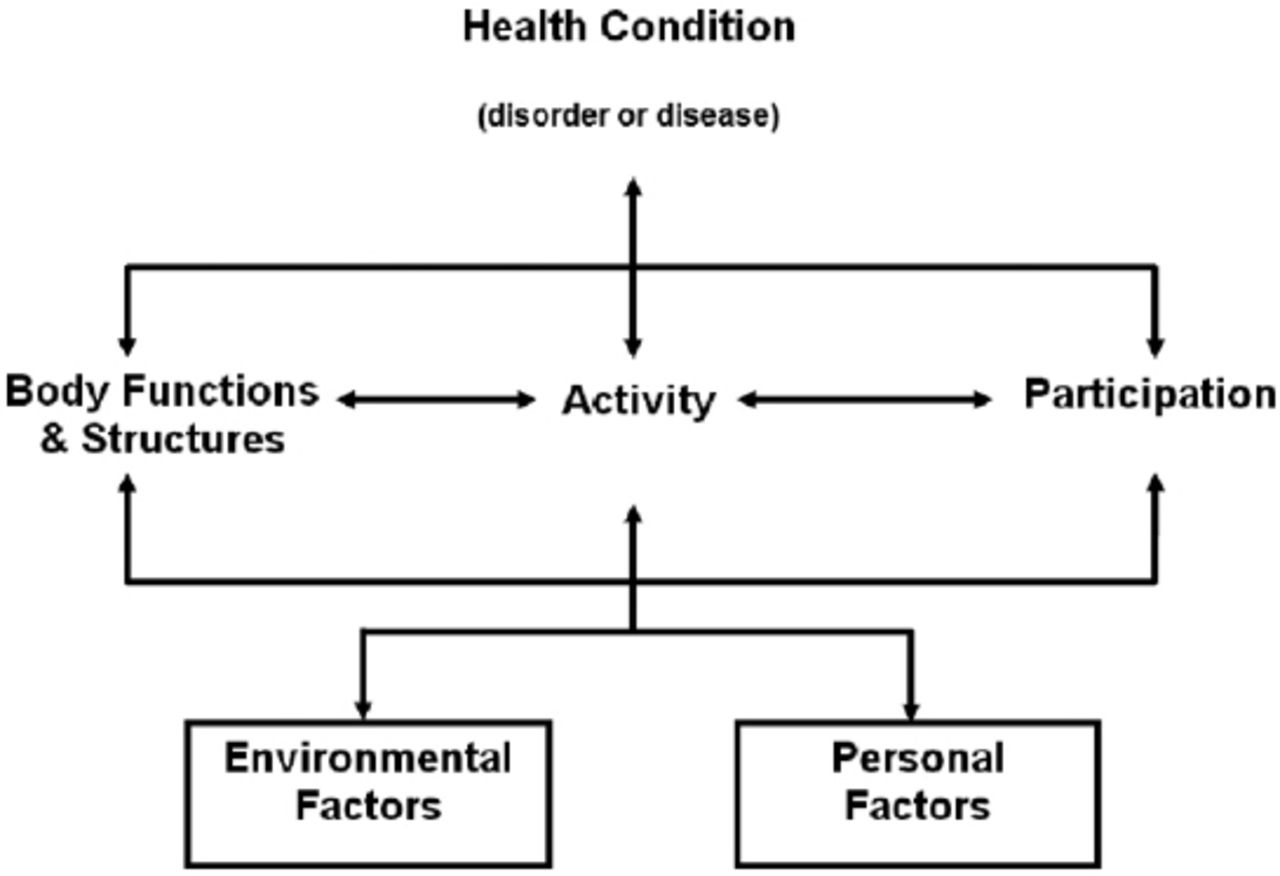
Interactions between segments of the International Classification of Functioning, Disability, and Health model.

Tables
Member Responsibility Patient and family Characterizes objectives, assumes control over own rehabilitation program and long-term disability administration Rehabilitation nurse Creates a restorative environment, case administration, family instruction, skin and bowel/bladder care Rehabilitation social worker Appraisal and administration of family and community assets, discharge arrangements, case administration Physician Therapeutic administration of inability, oversees comorbid conditions; included less outside of serious rehabilitation settings Occupational therapist Appraisal and treatment of self-consideration aptitudes; upper extremity disability, splints, and assistive devices Physical therapist Appraisal and treatment of mobility issues; quality, adaptability, balance, continuance, coordination, help with mobility Orthotics/prosthetics Suggests, plans, manufactures, and gains individualized equipment Speech and language pathologist Appraisal and administration of communication disorders, swallowing Psychologist Appraisal and administration of cognitive, behavioral, and effective status; connects with the perceptual-motor and language status Dietetics and nutrition Appraisal and administration of the dietary state, extraordinary eating regimens, enteral and parental feeding Recreation therapist Appraisal and administration of leisure preferences, adoptions, and integration into the therapeutic plan Optometrist Appraisal and administration of low vision weaknesses and disability - Table 2
A selection of outcome measures that have demonstrated construct validity in stroke rehabilitation by using the International Classification of Functioning, Disability, and Health domains.44,45
Body structure and function Activities Participation 1. Beck Depression Inventory 1. Action Research Arm Test 1. Canadian Occupational Performance Measure 2. Behavioral Inattention Test 2. Barthel Index 2. EuroQoL Quality of Life Scale 3. Canadian Neurological Scale 3. Berg Balance Scale 3. Assessment of Life Habits (LIFE-H) 4. Clock Drawing Test 4. Box and Block Test 4. London Handicap Scale 5. Frenchay Aphasia Screening Test 5. Chedoke McMaster Stroke Assessment Scale 5. Medical Outcomes Study Short-Form 36 6. Fugl-Meyer Assessment 6. Chedoke Arm and Hand Activity Inventory 6. Nottingham Health Profile 7. General Health Questionnaire-28 7. Clinical Outcome Variables Scale 7. Reintegration to Normal Living Index 8. Geriatric Depression Scale 8. Functional Independence Measure 8. Stroke Adapted Sickness Impact Profile 9. Hospital Anxiety and Depression Scale 9. Frenchay Activities Index 9. Stroke Impact Scale 10. Line Bisection Test 10. Motor Assessment Scale 10. Stroke Specific Quality of Life 11. Mini-Mental State Examination 11. Nine-hole Peg Test 12. Modified Ashworth Scale 12. Rankin Handicap Scale 13. Montreal Cognitive Assessment 13. Rivermead Mobility Scale 14. Motor-free Visual Perception Test 14. Rivermead Motor Assessment 15. National Institutes of Health Stroke Scale 15. Six-Minute Walk Test 16. Orpington Prognostic Scale 16. Timed Up and Go 17. Stroke Rehabilitation Assessment of Movement 17. Wolf Motor Function Test 18. Dynamic Gait Index Name Number of citations Purpose Description Advantages Disadvantages Frenchay Aphasia Screening Test (FAST)52 240 Screening device to identify patients with communication difficulties FAST evaluates languages in 4 noteworthy ranges: appreciation, verbal expression, perusing, and composing.
Testing is engaged around a solitary, twofold sided jolt card delineating a riverside scene on one side and geometric shapes on the other and 5 composed sentences.
Scores from every test territory are summed to obtain an aggregate score out of 30. Ten points are accessible for each of the cognizance and verbal expression; 5 each for perusing and composingInterpretability: Age-stratified regulation of information is accessible; taking into account the appraisal of 123 people aged 20 to 81+.
Acceptability: FAST is short and straightforward, requiring less than 10 minutes of management.
Feasibility: FAST is easy to regulate notwithstanding during a bedside assessment. Test materials are straightforward and portableThe specificity of FAST appears, by all accounts, to be antagonistically influenced by the vicinity of visual field shortfalls, visual disregard or distractedness, lack of education, deafness, poor focus or confusion Fugl-Meyer Assessment of Motor Recovery after Stroke (FMA)53 656 The FMA is intended to evaluate motor function, balance, sensation qualities, and joint function in hemiplegic post-stroke patients The scale consists of 5 areas; motor function, sensory function, balance, joint range of motion and joint pain.
Scale items are scored on the premise of capacity to complete the item utilizing a 3-point ordinal scale where 0=cannot perform, 1=performs in part, and 2=performs completely.
The total possible scale score is 226 (100 for engine capacity; 24 for sensation; 14 for parity; 44 for scope of movement; and 44 for joint pain)Interpretability: The interpretability of the FMA is improved by the scale’s strong establishment in all around characterized phases of motor recovery. It is broadly utilized and globally acknowledged.
Acceptability: Administration of the entire test can be a long process; it takes 30-45 minutes.
Feasibility: The FMA should be regulated by a prepared physical or occupational therapist. Particular equipment is not required; it is managed over an assortment of settings and can be used in longitudinal assessmentsNeed a prepared specialist.
Takes significantly more time for evaluationsHospital Anxiety and Depression Scale (HADS)54 20593 A bi-dimensional scale was developed specifically to recognize instances of depression and anxiety disorders among physically sick patients The HADS consists of 14 items isolated into 2 subscales of 7 items each: the anxiety subscale (HADS-An) and the depression subscale (HADS-D).
The respondent rates every item on a 4-point scale extending from 0 (absence) – 3 (extreme presence).
Five of the 14 items were coded in reverse.
The aggregate scale score is out of 42 or 21 for each of the subscales.
Higher scores showed more noteworthy levels of anxiety or depressionInterpretability: No standards are accessible in English.
Acceptability: The scale is convenient and simple to utilize (2-6 minutes).
Feasibility: The HADS is easy to utilize and scoreNo institutionalization for age or gender has been performed.
Cut-off focuses utilized are not specifically well establishedModified Ashworth Scale55 257 To evaluate the adequacy of hostile to spastic medication in patients experiencing different sclerosis The unique Ashworth scale consists of 5 evaluations from 0-4. (0 = no increment in muscle tone; 1 = slight increment in muscle tone; 1* = slight increment in muscle tone; 2 = more stamped increment in muscle tone; 3 = significant increases in muscle tone; 4 = influenced part unbending in flexion or expansion) Interpretability: The first Ashworth and Adjusted Ashworth scales are essential clinical measures of tone.
Acceptability: While testing should be moderately concise, control of the affected appendage/joint may be uncomfortable for patients.
Feasibility: No particular equipment is requiredLower levels of unwavering quality. In investigations of post-stroke patients, the most widely recognized appraisals reported are 0, 1, and 1+. The largest amounts of between spectator and intra-observer assertion are noted among patients with a 0 rating Mini-Mental State Examination (MMSE)56 2771 The MMSE was created as a brief screening instrument to provide a quantitative appraisal of intellectual disability and to record subjective changes after some time The MMSE consists of 11 basic inquiries or errands. These are assembled into 7 cognitive spaces; introduction to time, introduction to place, enrollment of 3 words, consideration and computation, review of 3 words, language, and visual development.
A score of 23/24 is the most acknowledged cut-off point showing the presence of cognitive impairmentInterpretability: The MMSE is broadly utilized and the most acknowledged part was the cut-off scores, which were demonstrative of cognitive impairment.
Acceptability: The test is brief, requiring approximately 10 minutes to complete.
Feasibility: The test requires no specific equipment, requires little time and is inexpensiveIt is unrealistic to distinguish adequate cut-off scores for visual or verbal memory issues
Low reported levels of affectability among stroke patientsFunctional Independence Measure (FIM)57 1293 Measures the level of understanding the disability and demonstrates the amount of help required for the person to complete the movement of activity of daily living (ADL) Consists of 18 items: 13 motor assignments and 5 cognitive errands (considered fundamental ADL).
Tasks are evaluated on a 7 point ordinal scale that ranges in total assistance (or complete dependence) to complete independence. Scores range from 18 (least) to 126 (most elevated demonstrating level of function). Scores are for the most part appraised upon admission and dischargeFIM survey the ADL FIM is used to assess impairment among adults (18-64 years); Elderly adults (65 years or older).
FIM is utilized to assess mind damage, geriatrics, various sclerosis; orthopedic conditions including low back pain, spinal cord harm and stroke persistent individuals.
Excellent test-retest dependability.
FIM has high inward consistency and satisfactory discriminative abilities for rehabilitation patientsStandard error of estimationn mean (SEM) and insignificant recognizable. Change not built up.
There is no cut-off scores. FIM is not freely accessibleBathel Index (BI)58 10962 Evaluates the capacity of a person with a neuromuscular or musculoskeletal disorder to standard care 10 ADL exercises including feeding, bathing, grooming, dressing, bowel control, bladder control, toileting, chair transfer, ambulation, stair climbing.
Items are appraised based on the measure of help required to complete every activityArea of evaluation incorporates ADL; functional mobility; gait.
It sets aside less time to complete the evaluation.
It is an execution based measure. Equipment and preparation not requiredTest-retest reliability not established Action Research Arm Test (ARAT)59 275 The ARAT is a spectator appraised, execution based evaluation of upper extremity function and aptitude The ARAT has only 19 items, which are assembled into 4 subsets: grasp (6 items), grip (4 items), pinch (6 items), and gross movement (3 items).
All items are evaluated on a 4-point ordinal scale going from 0 to 3 where 0 represents no movement possible, and 3 represents normal performance of the taskInterpretability: As a Guttman scale, level of execution is effortlessly comprehended and contemplated.
Acceptability: Not proper for use with proxy; negligible weight for patients.
Feasibility: A broad gathering of items and a particular table are required. Testing must be completed in a formal settingIn patients with serious disabilities or close typical function, the scale may not be sufficiently delicate to identify changes in execution Motor Assessment Scale (MAS)60 698 The MAS was created to obtain a substantial and solid method for evaluating regular motor function following stroke The MAS consists of 8 items relating to 8 regions of motor function (recumbent to side lying, prostrate to sitting over the edge of a bed, adjusted sitting, sitting to standing, walking, upper-arm function, hand developments and propelled hand exercises).
Each parameter, except for general tonus, is evaluated utilizing a 7-point pecking order of useful criteria. Score extending from 0 (most basic) to 6 (generally complex)Interpretability: Scores mirror a task-oriented approach to assessment.
Acceptability: The test is generally straightforward and brief to manage.
Feasibility: The MAS is freely accessible in Carr et al.66 A time of direction and practice evaluation is prescribed preceding formal use in a clinical or exploration settingThe item “general tonus” is difficult to survey in a dependable manner.
The scoring pecking order connected with the propelled hand exercises itemSix-Minute Walk Test (6MWT)61 48 The 6MWT is a sub maximal test of functional activity limit The 6MWT led utilizing a lobby or tracks 100 feet long.
Patients select their own power of activity and are permitted to stop and rest during the test, at their own particular pace.
Performance on the 6MWT is measured by aggregate separation strolled in feet or meters within the 6 minutes.Interpretability: The 6MWT is a broadly utilized apparatus that gives a quantitative measure of sub-maximal activity limit. It is concurred that age, stature, weight, and gender all freely affect the 6MWT in healthy adults.
Acceptability: The 6MWT is moderately concise and heavily endured by patients; however, its utilization may be complicated by issues of continuance.
Feasibility: The test is brief, modest and easy to assessIt is highly recommended that 6MWT combined with other measures for a better estimate Stroke Impact Scale (SIS)62 760 Surveys health status after stroke A 59 item measure, 8 domains are assessed: strength (4 items), hand function (5 items), ADL/IADL (10 items), mobility (9 items), communication (7 items), participation/role function (8 items).
Each item is rated on a 5-point Likert scale in terms of the difficulty the patient has experienced in completing each item.
Cumulative scores are obtained for every space, scores range from 0-100.SIS assessment including ADL; cognition; communication; depression; functional mobility; gait; general health; life participation; quality of life; social relationships; social support; upper extremity function SIS assessment is patient reported outcomes Medical Outcomes Study Short-Form-36 (SF-36)63 355 The SF-36 is a non-specific health survey developed to survey health status in the all inclusive community The SF-36 consists of 8 measurements or subscales: physical functioning, role limitations-physical bodily pain, social functioning, general mental health, role limitations-emotional, vitality, and general health perceptions.
Each of the 8 summed scores is directly changed onto a scale structure 0-100 to obtain a score for every scale. Furthermore, a physical component (PCS) and mental segment score (MCS) can be obtained from the scale itemsInterpretability: Utilization of the scale scores and synopsis part scores represents lost data and reduction in potential clinical interpretability.
Acceptability: Fruition time is approximately 10 minutes for either the self-finished or interview managed questionnaires.
Feasibility: It has been used as a mail survey with reasonably high completion rates reportedHigher rates of missing information have been accounted for among older patients when utilizing the self-finished type of organization.
The SF-36 does not fit the era of a general synopsis score.
The level of test-retest unwavering quality reported in the stroke population demonstrates that the SF-36 may not be sufficient for serial correlations of individual patientsNottingham Health Profile (NHP)64 138 The NHP was intended to be a brief, subjective measure of wellbeing incorporating the social and belongings of illness The NHP consists of 2 sections. Part I consists of 38 parameters grouped into 6 subsections: physical mobility (8 items), pain (8 items), sleep (5 items), social isolation (5 items), emotional reactions (9 items), and energy level (3 items). All parameters are weighted and given an aggregate score of 100.
Part II consist of 7 items: paid livelihood, employment around the house, social life, individual connections, and sexual coexistence. These parameters are not weighted. A score out of a total of 7 is obtained by including the quantity of positive reactions. Higher scores correlate to poorer wellbeing status.Interpretability: The NHP has been generally utilized in many countries. A complete client’s manual is accessible, as are populace standards.
Acceptability: The NHP is short and basic form and requires little time to complete.
Feasibility: The test can be managed as either a self-report or verbal postal overviewThe NHP to some degree is a constrained measure.
The NHP is not suited for use in the all inclusive communityReintegration to Normal Living Index (RNLI)65 340 The RNLI was created as a short and straightforward approach to evaluate, quantitatively, the extent to which people who had encountered traumatic or debilitating sickness achieve reintegration In the RNLI, 11 decisive explanations were produced. Each of these announcements is appraised by the respondent on a 10 cm visual analogue scale (VAS): does not portray my circumstance (1 or negligible reintegration) and completely depicts my circumstance (10 or most extreme reintegration).
Individual item scores are summed to obtain an aggregate score out of 110, which focuses on the relative changes over time to obtain a score out of 100Interpretability: There are no generally accepted standards for understanding.
Acceptability: A short and straightforward assessment of the RNLI represents negligible patient weight.
Feasibility: The RNLI is accessible for free. It can be utilized to evaluate longitudinal studiesThe perfect composition of the subscales is questionable.
Reliability and legitimacy have not been significantly studied within the stroke populationEuroQoL Quality of Life Scale (EQ5D)66 3144 The EQ5D is a non-specific recorded instrument, created by a multi-nation, multi-disciplinary group, used to depict well-being and esteem. The EQ5D is a self-reported survey, consisting of 2 sections.
Part I consists of 5 measurements: mobility, self-care, usual activities, pain/discomfort and anxiety/depression).
Each measurement is represented by 3 articulations comparing to 3 levels: item-1 (some problems), 2 (moderate problems), and 3 (extreme problems).
Part II consists of a VAS in which respondents rate their present condition of wellbeing from 0 (worst imaginable) to 100 (best possible)Interpretability: EQ5D utilizes population base utility weights to obtain a standard arrangement of utility qualities for the 5-digit wellbeing state from the 5-domain index.
Acceptability: Short and straightforward, reports of missing information are blended.
Feasibility: It is a self-reported questionnaire that may be regulated as a postal or phone survey or in a face-to-face interviewNot suitable for use in serial evaluations of individual patients.
Reliability was lower when the post-stroke intermediary respondent completed the questionnaire for understanding on the patient’s behalf
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.