


Abstract
Objectives: To explore the perspective on Decompressive craniectomy (DH) of each of these specialties to establish common grounds for improved clinical practice.
Method: An electronic survey was distributed via email and social media groups to members of these specialties in Kingdom of Saudi Arabia and the Gulf countries. Local practices, common triggers for referral for DH, perceived outcomes of these procedures, individual impression of what constitutes good clinical outcomes were explored.
Results: There are 89 physicians participated: 41 (46.1%) neurologists, 34 (38.2%) neurosurgeons, and 14 (15.7%) intensivests. Participants are mostly practicing in intermediate volume centers or high volume centers. Half of the neurosurgeons preferred to be consulted immediately on candidates with large middle cerebral artery (MCA) strokes. The most important referral trigger for DH was clinical changes. The modified Rankin Scale (mRS) cutoff for good clinical outcome was 3 for 73.6% of respondents. There was agreement that DH only improves survival (64.4%). A third of the neurologists considered it to improve functional outcome compared to 15.4% of intensivests and 14.8% of neurosurgeons. There was agreement (66.7%) that patients older than 60 years with involvement of more than one territory should be excluded from DH. Only 7.7% of neurosurgeons excluded patients with dominant hemispheric strokes.
Conclusion: Our physicians’ views are variable in what’s called acceptable outcome, and further studies are needed to to test the characteristics that helps in decision making such as hemisphere dominancy, time onset of stroke and vital radiological signs. This is seen despite the literature being full of data that supports the DC over medical management in malignant MCA infarction. Better multidisciplinary education initiatives are needed to unify the understanding and help improve the practices in this challenging subset of patients.
The middle cerebral artery (MCA) supplies most of the cerebral hemisphere and most of its functional areas and its infarctions related to its occlusion are considered the most common vascular territory affected in ischemic strokes. Less than 20% of middle cerebral artery infarction patients’ recover to independent living with very few achieving complete recovery.1,2 A subset of patients with massive stroke in the MCA territory undergo cytotoxic edema which ends up with elevated intracranial pressure (ICP), decreases cerebral perfusion pressure (CPP) and either fatal herniation up to 80% of the cases or severe disability. Surgical management of malignant MCA stroke is standardized as a hemispheric Decompressive craniectomy (DC) with expansive duraplasty. This type of surgery results in significant reduction of the intracranial pressure from the brain edema and prevent herniation by allowing the brain to swell outward without causing midline shift and uncle herniation. This method may reduce mortality and morbidity if performed in the first 48 hours of the MCA insult.3
The decision whether to perform DC remains a controversial issue despite supporting evidence form randomized trials with no definitive evidence-based guideline is available to date.4 Five randomized clinical trials studied the mortality and morbidity in hemicraniectomy as compared to non-surgical management. The DECIMAL1 trial was an open, prospective, randomized, multi-center trial that included 38 patients. While HAMLET4 trail was also an open, randomized multicenter trial but included 68 patients. Another trial called DISTENY5 was a controlled, prospective, randomized clinical trial enrolled 32 patients. However, these studies were subject to different interpretation given their small sample sizes and the relatively low number of patients with independent recovery as opposed to those with moderate disability. Thus, their findings did not widely translate into a describable change in medical practice. The aim of this study is to explore the perspective on DC of different specialties involved in the management decisions and the care of stroke patients, and to study the factors that influence the decision based on perceived or actual effectors.
Methods
Participants
We contacted physicians who are involved in the management of patients with complicated ischemic stroke; in secondary and tertiary care centers. These included neurologists, neurosurgeons, and, critical care physicians (intensivests). We omitted all those who did not complete the electronic survey.
Study design
A cross-sectional descriptive study was conducted on physicians in the Kingdom of Saudi Arabia and the Gulf region. An email was sent to all potential participants. In addition, participants were approached via social media and smart phones applications. Participant’s identity and centers of affiliation were not collected. The study period was from January to April 2016. The data sheet was in the English language. Data was entered and analyzed using the statistical analysis was performed by the IBM SPSS Statistics for Windows version 22.0 (IBMCorp, Armonk, NY, USA).
Data sheet
The online survey, consisted of multiple clinical case scenarios. Participants were informed that this survey is not meant to examine them personally. Answer sheets of all were anonymous throughout the study and after its conclusion. We collected data on the practice setting, clinical experience and, geographical location of practice to correlate collected data with the standard of service provided.
Statistical analysis
Collected data were analyzed with SPSS version 22. The chi-square test was used for analysis categorical variables, while the T-test was used for continuous variables. Factors affecting DC option of management were assessed by Logistic regression.
Result
A total of 300 emails were sent. Out of all questionnaires that have been collected, 92 physicians participated and completely filled out the questionnaire. Analyzing study subjects’ characteristics, (54%) with clinical experience of less than 10 years. Others, with experience exceeded 10 years (46%). Among multi-specialties involved, neurologists were predominant in this study (45%), followed by Neurosurgeons (38%) and, intensivests comprising 17% of our respondents. The vast majority’ work in a tertiary hospital (73%), followed by secondary hospitals (23%).
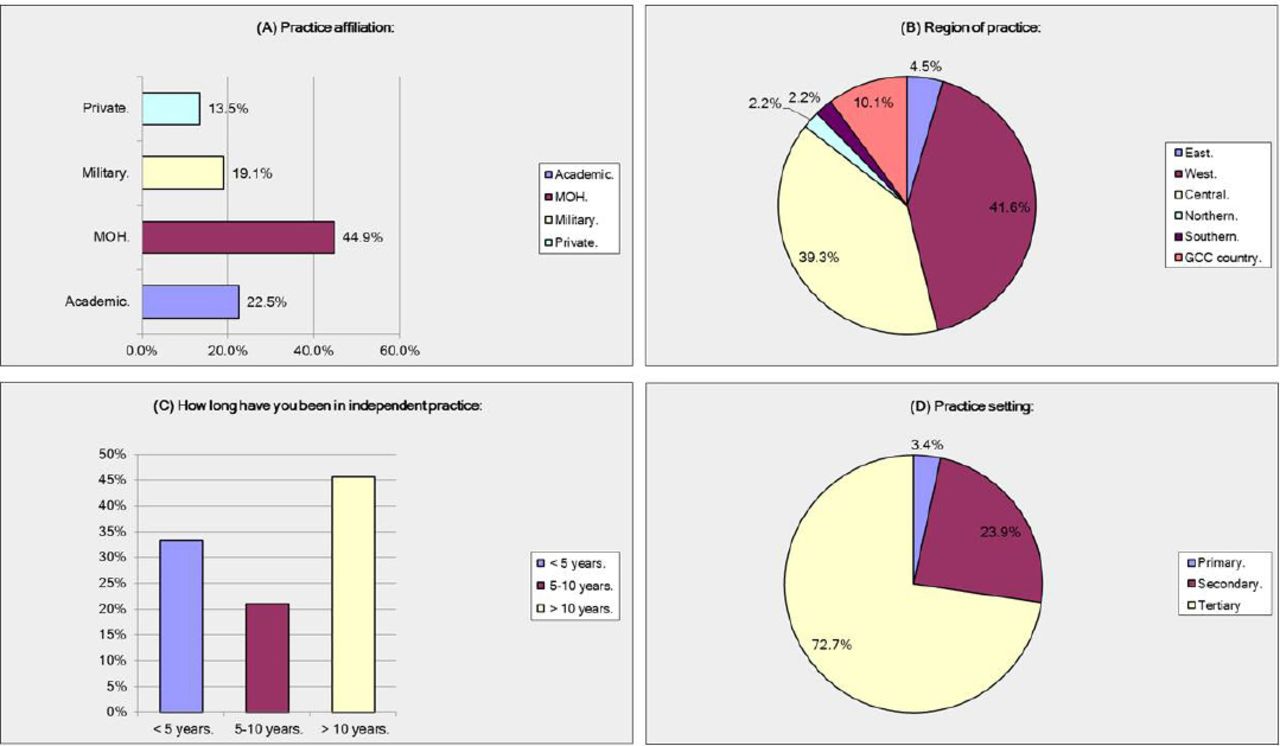
While addressing the geographical location of practice, most of the replies were from central (40.5%), and western regions (40.5%) of Saudi Arabia. A lesser response rate was obtained from other national regions in the kingdom (9%), and by other Gulf coalition countries (GCC) (10%) (Figure 1).

Demographics of participating physicians.
Intuitively, affiliation of participant showed most to be working in the ministry of health (45.1%). Also, contribution from academic (23.1%), military (18.6%) and, private (13.2%) physicians were encountered. Although, (48%) of respondents declared that they admit 50-150 stroke cases per year, the implementation of stroke protocol was suboptimal (30%). Moreover, (69%) of subjects do not have a stroke unit or dedicated Neuro ICU in their work flow. However, angiography suites were available in the majority of centers (75.3%). Surprisingly, (83%) of subjects believed that ICP monitoring is of great value, (17%) agreed that it delivers no value.
The imaging modality of choice in acute ischemic stroke is a CT scan of the head (78%). The IV thrombolysis is offered routinely in (55%) of centers. Before giving IV t-PA, Patient/family consent was considered mandatory according to 85.2% of respondents. Referral to neurosurgery is carried out in more than 5 cases for DC per year (52.8%), but others stated that less than 5 are referred (47.2%) annually.
Analyzing proper timing of neurosurgical involvement for acute ischemic stroke, the majority went with an immediate DC at the time of neurosurgical consultation (53%), followed by when radiological changes are present (32%) and, when concomitant with clinical changes (10%). A minority indicated that the ideal timing is 24 hour post imaging (5%). Regarding proper timing for prophylactics DC, this was considered to be not specific in (36.4%), another opinion that is better not to be offered (31.2%), furthermore, some prefer to extend it after 24h (17%), 12h (5%) and, 6h (10.4%) respectively; the latter being a reflection on the concept of early utilization of DC. Analyzing proper timing of therapeutic DC with a trigger the majority with to be upon identification (80.3%). Concerning radiological triggers, compression of the lateral ventricle with midline shift (46.2%) and, followed by hypodensity >50% MCA territory (35.9%), are the most important triggers. Whereas, worsening GCS >2 is the most significant clinical trigger (57.2%). However, the most important trigger found to be the clinical trigger (59%), followed by Neurosurgeon threshold to operate (18%), Radiological trigger came third (17%) and, ICP monitoring came fourth (8%).
Surgical procedure is performed as Craniectomy and Duraplasty (57.3%), Other prefer Craniectomy alone (42.7%). In addition, it is preferred to defer necrosectomy (removal of infarcted tissue) (79%) with, avoiding EVD insertions (62%).
As to the outcome stratification, majority of respondents selected 3 as the cut-off for a good outcome by mRS (74%). The most substantial impression of outcome found to be improved survival (65.3%). Statistically, significant bad influence factors to proceed with surgery, are age >60 with more than one territory (67%), followed by papillary changes (20.27%) and, dominant hemisphere (12.16%) (Table 1).
Survey answers per respondents’ specialty.
Discussion
In this study, we explored the perspective of physicians including neurologists, neurosurgeons, and intensivests regarding decision making of whether they prefer DHC in malignant MCA infarction or medical management and the factors that influenced their decision. Our study showed that 30% of neurologists, 15 % of neurosurgeons and intensivests considered DHC surgery has better functional outcome in comparison to conservative medical management alone in intensive care with ICP monitoring.
There is an agreement that the predicted reduction of morbidity mortality is attained by proper timing of DC within 48 hours of stroke onset.3 This is at great discrepancy with our findings, given the attitude of caring physicians to proceed with DC in our study was based on clinical deterioration in 59% of instances or with complete disregard of dangerous radiological signs by 53% of respondents. The factors influencing toward conservative management in our study were age >60, patients with more than one territory involved (67%) which was different from the existing data that preferred hemisphere dominancy.2
Our findings were similar to prior cross-sectional studies in different settings. DISTENY5 trial was a controlled, prospective, randomized clinical trial enrolled 32 patients, DISTENY-S2 study surveyed 1859 physicians from 62 countries regarding the treatment decision depending on these factors: (1) dominant versus non-dominant hemispheric stroke: 47% of physicians would go for DC in dominant hemisphere compared to 12.6% of our respondents2 while in DECIMAL trial that was an open, prospective, randomized, multi-center trial included 38 patients, found similar outcome in both dominant and non-dominant hemispheric stroke patients.1 (2) mRS acceptable outcome: 74% of our respondents agreed on mRS of 3 to be acceptable outcome which is expected from previous studies1,2 that showed similar results.
A third of our respondents believe that DC can improve functionality and 64% believes it greatly improves survival rate. In the DECIMAL1 trial, the absolute mortality risk reduction with DC was 53%. HAMLET4 trail that was an open, randomized multicenter trial included 68 patients showed 38% absolute risk reduction and in DISTENY5 trail 12% showed decrease in 30-days mortality with those who underwent DC as compared to 53% mortality in medically treated patients. Our study limitations include the geographically concise areas involving physicians in west and central Saudi Arabia, mostly neurologists which showed high response rate. Also the under availability of stroke units and neurointensivests in the respondents’ facilities. Lastly, the physicians’ opinion does not necessarily reflect the patient or decision-makers opinions and biases in regards to decision making process.
We recommend further studies to geared towards establishment of a comprehensive guidelines that governs our practices in line with pre-existing literature on what best serves the patient’s health and wellbeing in our loco-regional health systems.
In conclusions, our physicians’ views are variable in what’s called acceptable outcome, and further studies are needed to to test the characteristics that helps in decision making such as hemisphere dominancy, time onset of stroke and vital radiological signs. This is seen despite the literature being full of data that supports the DC over medical management in malignant MCA infarction. Better multidisciplinary education initiatives are needed to unify the understanding and help improve the practices in this challenging subset of patients.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received March 9, 2017.
- Accepted February 14, 2018.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.