


Janus Kinase 2 (JAK2) protein controls the signal transduction of the erythropoietin, thrombopoetin, and related receptors that control erythrocyte and megakaryocyte expansion. A somatic mutation of JAK2-V617F in the exon 14 of the JAK2 gene (9p24) is the most common cause of myeloproliferative disorder called polycythemia rubra vera (PRV).1-3
Polycythemia rubra vera is characterized by elevated hemoglobin, red cells mass, platelets and white cell counts. The incidence of PRV is 0.4-2.8/100,000 persons/year in Europe and the prevalence is 44-57/100,000 persons.3 The PRV is most common in those aged between 50-70 years and the risk of death with PRV is 1.6 times higher than the general population. We present a patient whose first clinical manifestation of the PRV was chorea though chorea as the first presentation of the PRV is rare (less than 5%). However, other neurological manifestations like headache, visual symptoms or cognitive impairment are common in PRV.1-3
Polycythemia rubra vera is a chronic disease and the treatment protocol should be individualised. Phlebotomy is performed to reduce hematocrit below 45% to improve blood circulation. Since this condition leads to hyperviscosity, low dose aspirin is recommended to reduce the risk of thrombosis.2 However, in people above 60 years of age with hypertension or previous thrombosis, drugs like hydroxyurea can be tried.2,4
An 80-year-old woman presented with abnormal limb and facial movements for 6 months. She was slightly fidgety and unsteady but reported no change in mood, memory or cognition. She reported headache after 6 months of the abnormal limb movements. She was taking a regular antihypertensive but no neuroleptics or antiemetics. She had normal mini-mental score (25/30), normal motor, sensory and cerebellar examinations except generalized involuntary, repetitive, jerky movements suggestive of chorea but no parkinsonism or dystonia.
The chorea was most prominent in orofacial region and her upper limbs. She demonstrated motor impersistence evidenced by ill-sustained tongue protrusion on request. Her routine blood tests revealed raised hematocrit of 57% (normal up to 52%), hemoglobin of 175g/L (normal value: 120-160gm/L), white cell count of 14x109/L (normal 4-11x109/L) and platelet counts 6.8x109/L (normal: 1.5-4x109/L) but normal serum erythropoietin level; normal serum copper, ceruloplasmin, ferritin & lipids; and no acanthocytes. The serum was negative for Lyme’s, human immunodeficiency virus and syphilis serology, connective tissue screen, paraneoplastic/antineuronal antibodies, autoimmune antibodies like N methyl D aspartate and voltage-gated potassium channel antibodies.
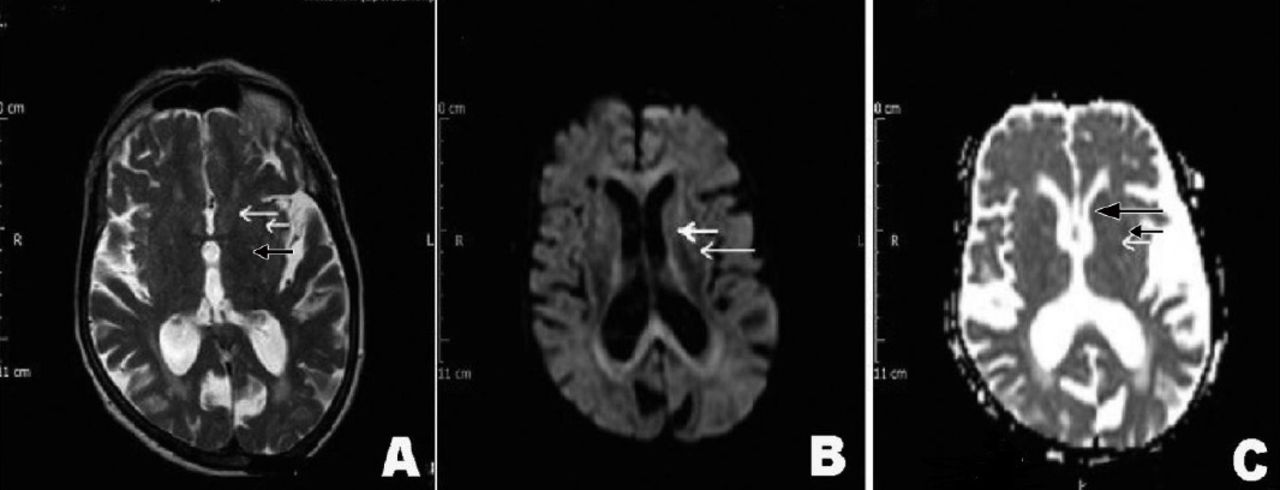
The magnetic resonance imaging showed no acute infarct, bleed or space-occupying lesions in the brain parenchyma including the striatum, basal ganglia, subthalamic region and the brain stem (Figure 1). The Computed tomogram scan of chest, abdomen, pelvis revealed no lymphadenopathy or space-occupying lesions. The genetic screening for Huntington’s disease, spinocerebellar ataxia 17 (SCA 17), dentatorubropallidoluysian atrophy revealed no pathogenic mutation. However, in view of her persistently raised haematocrit (54-56%) and platelet count (5.2-5.8x109/L) for 6 months on 3 successive occasions, she was tested for the JAK 2 mutation. Her JAK 2 V617F mutation was positive. She was diagnosed as generalized chorea due to PRV. Recently, her hematocrit dropped below 45% with regular phlebotomy though platelet count is still high (5.1x109/L) though chorea persisted. She was started on aspirin 75mg daily as per the advice of the haematologist.

T2 weighted Axial view Magnetic resonance imaging showing A) No infarct or space occupying lesion in the Caudate nucleus (large white arrow), putamen (small white arrow) or the Globus pallidus (black arrow), B) DWI image showing no hyperintensity to suggest acute vascular event in the Basal Ganglia (white arrows), C) The Acute diffusion coefficient MRI sequence showed no diffusion restriction in the Caudate nucleus (large black arrow), putamen (small black arrow) or Globus pallidus (white arrow).
Polycythemia rubra vera is a rare disease. It is even rarer for neurological features like chorea to be the first presenting manifestation. The literature suggests that chorea in PRV lessens with the improvement of the hematological parameters but our patient did not improve.1,2 The hyperviscosity due to the raised red cell mass in the neostriatal area probably led to the venous stasis, low blood flow, impaired oxygen and glucose metabolism, causing movement disorder.2,4,5 However, the persistence of chorea in our patient despite the improvement of blood viscosity raises 2 possibilities (namely, either hyperviscosity resulted in a lacunar infarct with irreversible injury to the striatum or the mechanism of chorea in PRV was not hyperviscosity alone).3,4 Lew J et al3 reported chorea in a patient with normal hematocrit but with positive JAK 2 V617F mutation. The other possible mechanisms of chorea are altered dopamine metabolism in platelets or receptor hypersensitivity secondary to estrogen deficit in post-menopausal women.4,5 However, magnetic resonance imaging is often inconclusive in polycythemic chorea like our patient.
Polycythemic chorea is more prominent in the orofacial and lingual muscles though it can be generalized also. Polycythemia rubra vera should be considered as one of the causes of adult onset treatable chorea. The other, more common, causes of chorea in the adult are genetic, drug-induced, infective, paraneoplastic or vascular.
In conclusion, an 80-years-old woman presented with predominantly orofacial and lingual chorea. She tested positive for JAK 2 V617F mutation and was diagnosed as PRV. The improvement of hematocrit after phlebotomy did not lead to the resolution of her chorea.
Acknowledgment
The author would like to thank Dr. Nick Hollins, Consultant Radiologist, Royal Cornwall Hospital NHS Trust, Uinted Kingdom, for reviewing the MR images.
Footnotes
Disclosure. Authors have no conflict of interests, and the work was not supported or funded by any drug company.
- Received August 2, 2018.
- Accepted November 7, 2018.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.