


Abstract
This case series described changes in motor outcomes across 4 cases of older adults (mean age – 64.75) with chronic stroke (>6 months) after implementation of a 6-week proprioceptive neuromuscular facilitation-based program. Findings of this study were compared with a previously reported case. At baseline, all cases presented with motor impairments that increased their fall risk such as impaired balance, lower extremity strength, and mobility. Outcomes were measured using the Mini-BESTest, posturography, 5 times sit-to-stand test, upright motor control test, and 10-meter walk test. All cases completed 1 hour of therapy 3 times a week for 6 consecutive weeks at a university-based outpatient rehabilitation clinic. Positive outcomes in balance, strength, and mobility were seen in all cases. Proprioceptive neuromuscular facilitation can modify motor outcomes to decrease fall risk in older people with chronic stroke. Chronicity of stroke, age, and co-morbidities may influence the degree of improvements expected in these motor outcomes.
Stroke is a prevalent condition associated with high global burden of disease. In 2010, an estimated 33 million people live with chronic stroke, an 84% increase in the past 2 decades.1 Individuals living with stroke have multiple long-term motor impairments with strength, balance and mobility that negatively impact participation and quality of life.2 These motor impairments increase risk for falls and may compound the multiple-system physiologic decline associated with aging.3 While several studies have reported that most gains from rehabilitation occur with the first 6 months after stroke, improvements have still been noted following well-targeted exercise therapy programs in more chronic presentations.4 Interventions grounded in modern theories of neuromuscular re-education and neuroplasticity are needed to improve rehabilitation efforts and optimize functional outcomes.5
Proprioceptive neuromuscular facilitation is a form of neuromuscular re-education that has been used in improving the function of patients with stroke.6,7 Preliminary empirical evidence describes how a proprioceptive neuromuscular facilitation-based program coupled with the principles of neuroplasticity has the potential to generate positive outcomes in an older adult with chronic stroke.6 However, despite the increase in published literature on the effects of proprioceptive neuromuscular facilitation, there is still limited evidence that explores how a proprioceptive neuromuscular facilitation using modern principles of neuroplasticity can improve motor outcomes. There is also a need to explore the characteristics of patients that would likely benefit from this type of program.
This study aimed to compare the changes in motor outcomes after a proprioceptive neuromuscular facilitation program across 4 new cases of older people with chronic stroke with different chronicity and disability severity. Further, this study aimed to relate the findings with those from a previously published case report that demonstrated the potential usefulness of the proprioceptive neuromuscular facilitation program.6 Each case described in this study showed chronic stroke with varying clinical presentations including differences in strength, balance, and mobility. The variations in each case may allow generation of hypotheses related to the potential benefits of a proprioceptive neuromuscular facilitation-based program, and which patients are likely to benefit from this intervention.
Case Report
Patient’s information
The study included 4 new cases of older adults (mean age - 64.75 years) with chronic stroke (>6 months post-stroke) receiving therapy from an outpatient clinic in an urban, metropolitan setting from September 2016 to May 2017. We also present the findings from another participant (labelled XXX in this paper) which was published as a case report6 to relate the changes noted in the 4 new cases. All patients were medically stable and referred to physical therapy. Patients had varying severity, chronicity, and presentations of stroke and were at risk for falls (Table 1). Patients were deemed to have a high risk for falls due to older age, history of stroke, poor mobility and physical inactivity, presence of chronic medical conditions such as diabetes or osteoarthritis, or risk for falls based on their baseline balance assessments. Figure 1 shows the general study timeline.
Baseline demographic information of 4 older adults with chronic stroke who received proprioceptive neuromuscular facilitation.
General time line of intervention of 4 cases that received proprioceptive neuromuscular facilitation.
Case 1
A 65-year-old male who sustained a left sided stroke 18 years ago resulting in right hemiparesis. He began consistent therapy only one year before the current study due to financial constraints. His prior therapy consisted of weekly one hour sessions of task-oriented strengthening, balance, and gait training. He joined regular therapist-led weekly group exercises at the same clinic.
Case 2
A 62-year-old male who sustained his second right-sided stroke a year prior to participating in the study. The first stroke occurred 10 years earlier. He received prior therapy focusing on balance and functional ambulation using a quad cane, however, he did not use the cane outside of therapy. He primarily used a wheelchair propelled by his caregiver inside the house and in the community. He was able to stand from his wheelchair with close guarding to walk with a cane for about 10 steps before reporting fatigue and fear of falling.
Case 3
A 63-year-old female with a left-sided stroke 9 months prior to the start of the study. She received outpatient therapy a month prior to the current study. She walked with a quad cane with close guarding at home and contact guarding in the community. Although she performed basic activities of daily living by herself, she had multiple instances of near falls at home and in the community while standing or walking.
Case 4
A 69-year-old female with a left-sided stroke 9 years prior to the current study. She reported multiple instances of falls at home during walking and activities of daily living. She received therapy prior to the study and was ambulatory at home and used a wheelchair for community ambulation. She had impaired balance, lower extremity strength, decreased ankle range of motion, decreased gait speed, and had low self-efficacy in walking and performing tasks without assistance.
Clinical findings
All of the 4 new cases received treatment based on a similar framework published in an earlier study6 following the principles of proprioceptive neuromuscular facilitation and modern principles of neuroplasticity.5 Motor outcomes were assessed at baseline and after 18 intervention sessions by a trained independent assessor using standardized assessment tools as reported in a previously published case report.6 Lower extremity strength was measured using the Upright Motor Control Test (UMCT) and the Five Time Sit-to-Stand Test (FTSST), balance confidence was measured using the Activities-specific Balance Confidence scale (ABC), balance was measured using the Mini-Balance Evaluation Systems Test (Mini-BESTest) and Limits of Stability test (LOS) on the NeuroCom® Balance Master® (Natus, Pleasanton, CA, USA), and mobility was measured using the 10-meter walk test (10MWT). Pertinent clinical findings are presented in Table 1 and results of the pre-test are presented in Table 3.
Summary of proprioceptive neuromuscular facilitation interventions and progressions of exercises received by four cases of older adults with chronic stroke.
Results of pretest and posttest of the lower extremity strength, balance, balance confidence, and mobility of four older adults with chronic stroke that received proprioceptive neuromuscular facilitation.
Therapeutic intervention
Each case received 18 one-hour sessions (3 times a week for 6 weeks) of individualized treatment at an out-patient clinic from a licensed physical therapist who received specialized training in administering proprioceptive neuromuscular facilitation (Figure 1). Treatment were performed as described in Adler 2008.8 Interventions were based on the baseline assessment, and followed a similar intervention framework of a previously published study.6 Interventions are summarized in Table 2.
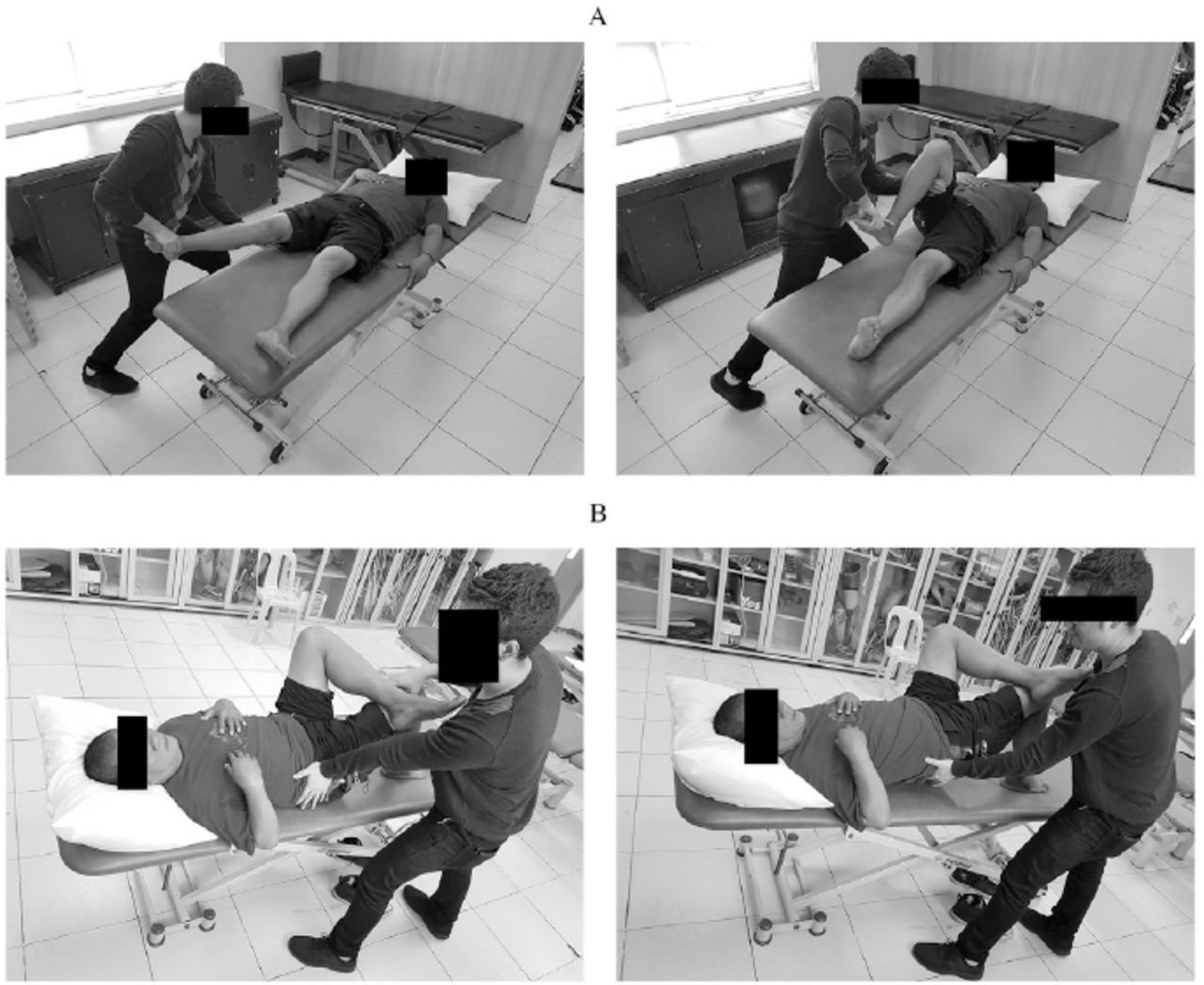
Resisted mat exercises included pelvic and lower extremity patterns, pelvic bridging, rolling, and sitting (Figure 2 a-b). Exercises were repeated 5-20 times up to tolerance, and modified based on response. Exercises difficulty was modified by changing the position, increasing intensity of the exercise, changing practice environments, or by changing amount of support. Manual resistance was applied during functional activities to facilitate performance.
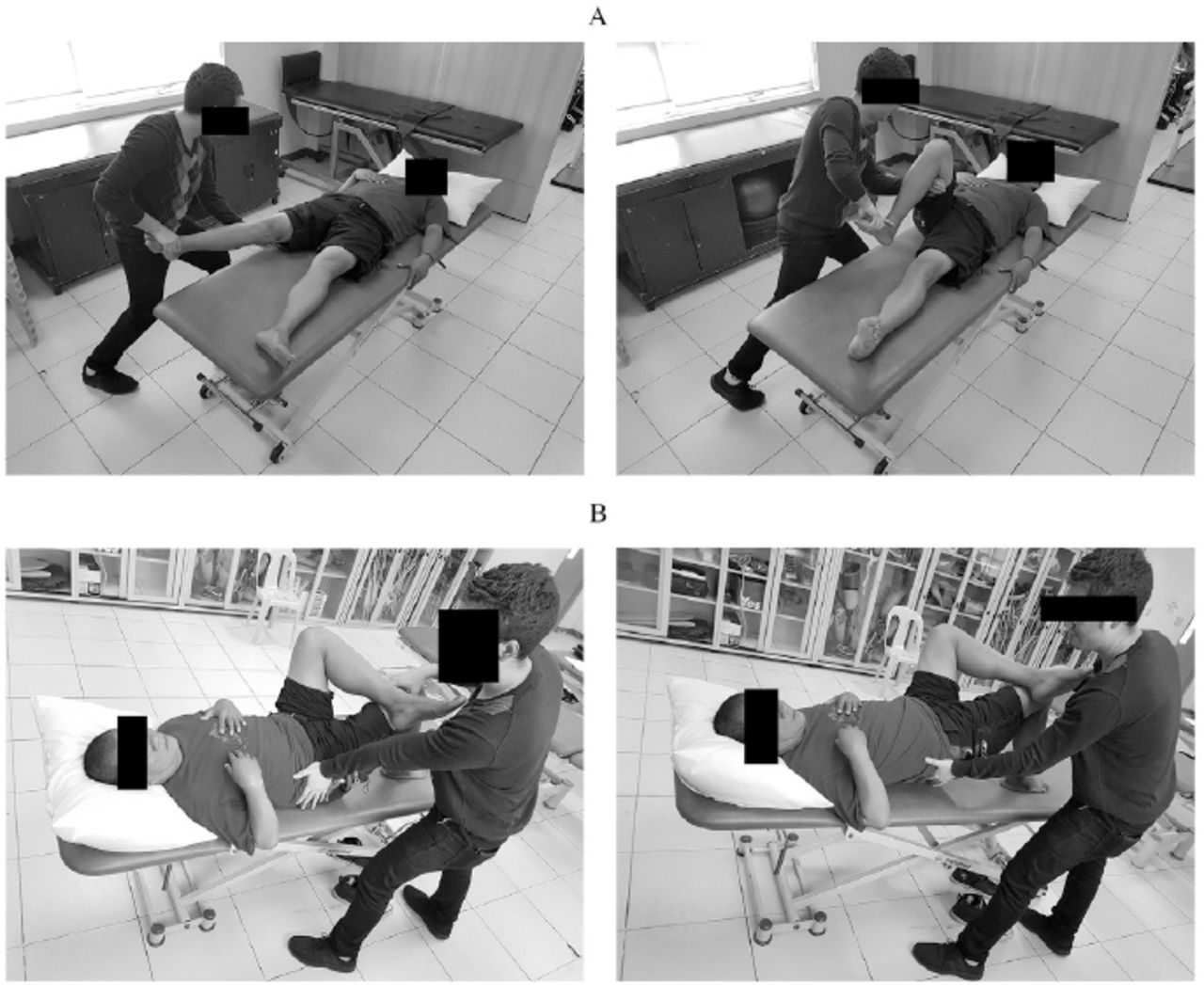
Proprioceptive neuromuscular facilitation mat exercises consisting of: A) lower extremity flexion-adduction with knee flexion and B) pelvic bridging with resistance
Hand placement, traction, approximation, and stretch to stimulate mechanoreceptors and guide movement were emphasized. Verbal and visual cues were given to facilitate correct movement. Proprioceptive neuromuscular facilitation techniques were used to elicit specific responses, and target specific goals (Table 2).
Gait training consisted of balance exercises in standing, resisted gait training, or walking in different directions. Balance exercises included stabilizing reversals with resistance at the pelvis or shoulders, and one-legged standing (Figure 3a-b). Difficulty was increased by changing amount of support or applying manual resistance on different areas while the patient holds the position. Resisted gait involved resistance at the anterior or posterior pelvis to facilitate forward or backward walking respectively (Figure 3c). Weight shifting was emphasized by asking the patient to hold the position for 5–6 seconds followed by instructions to exaggerate each step. Walking in different directions included forward, backward and sideward walking, and cross-over steps, and were progressed by increasing the duration or changing the environment (inside or outside the clinic).
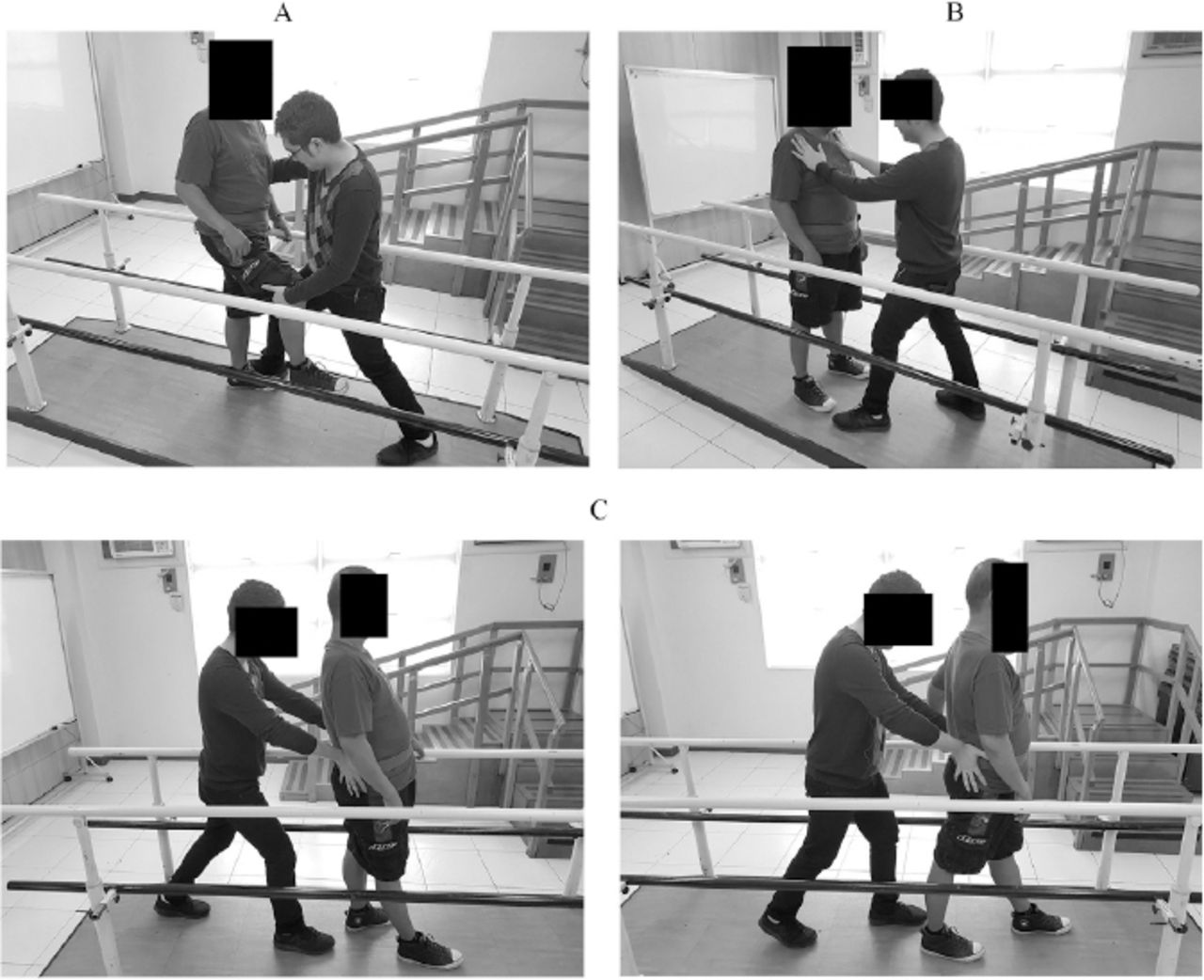
Proprioceptive neuromuscular facilitation gait exercises consisting of A) one leg stance with resistance B) stabilizing reversals and C) resisted backwards gait.
Although there were similar exercises such as lower extremity patterns and gait training, there were individualized differences in the plans of care of each case. For example, practicing stairs was emphasized if this was a therapy goal, or more exercises targeting impairments (pelvic and trunk weakness) or confidence were included if these were limiting movement more.
Follow-up and outcomes
All cases completed 18 sessions of intervention with no adverse outcomes. Each case showed varied degrees of change in their lower extremity strength, balance, confidence, and mobility. Significance of changes in outcomes were analysed descriptively using available minimal clinically important difference and minimal detectable change as described in a previous study.6 Summary of pretest and posttest results are found in Table 3.
Results of pretest and posttest of the lower extremity strength, balance, balance confidence, and mobility of four older adults with chronic stroke that received proprioceptive neuromuscular facilitation.
Cases 2 and 3 showed a change of one level on their UMCT-extension scores. No change in the UMCT-flexion scores was seen in any of the cases. Cases 2, 3, and 4 also showed significant change in their FTSST scores. Case 4 no longer used her cane to stand from sitting at posttest. Case 1 showed no significant change in strength in both the UMCT and the FTSST. Improvements in lower extremity strength were consistent with improvements in Case XXX.
Cases 2, 3, and 4 showed significant changes on the Mini-BESTest. Case 2 showed improvement in the reactive balance components of the test, while case 3 showed improvement in the mobility components. All cases also showed varied positive changes in LOS (improved reaction time, end-point excursion, movement velocity, and directional control). Balance confidence for cases 3 and 4 increased, while there was a decrease in case 2. Despite variety in ABC scores, all cases reported general positive changes in functional status. Cases 2 and 4 still required a wheelchair when ambulating outdoors, but both were able to walk indoors with a cane and supervision. Case 3 no longer required supervision when walking both indoors and outdoors. Improvements in balance, specifically in reactive balance and LOS, were consistent with case XXX.
Lastly, cases 2 and 3 markedly improved in gait velocity. Case 2 showed improvement in both self-selected and fast velocity, while case 3 showed improvement in fast velocity. These changes in gait velocity are consistent with case XXX.
Discussion
This case series showed that proprioceptive neuromuscular facilitation improved motor outcomes in 4 older adults with chronic stroke. The 4 new cases introduced in this study were consistent with the findings of a previously published case report,6 but also showed some differences in the extent of the changes observed. Despite the older age and the chronicity of stroke, proprioceptive neuromuscular facilitation improved multiple fall risk factors. Variations in these changes may be attributed to the severity of co-morbidities, impairments at baseline, chronicity of the stroke, individualization of treatment, and individual characteristics (history of falls, motivation, and goals). A limitation of this study is that follow-up on the maintenance of changes after post-test was not obtained.
The amount and severity of the co-morbidities appeared to have influenced outcomes. Cases 1 and 4, which had some form of cardiopulmonary, systemic, or musculoskeletal condition, had more limited tolerance to exercise than those without severe co-morbidities. In order for changes in motor control to take place through neuroplasticity, repetition and intensity are important. The severity of co-morbidities and their effects on the body may have limited the amount of exercise tolerated. Case XXX was similar with case 3 which did not have co-morbidities that significantly affected performance. Although the co-morbidities negatively impacted outcomes, all cases still showed improvements in the current study. This is important as patients with multiple co-morbidities are often excluded from published literature which may not be reflective of the type of patients commonly seen in practice.9
The change in levels of physical activity from baseline may have also affected variations in improvements across the 4 cases. Notable improvements in motor outcomes and function were seen in cases 2 and 4, which had lower baseline performance compared to the others. Given that the patients had therapy prior to the study, changes seen in the present study may have been caused by the increased frequency of intervention (3 times a week). This is also consistent with the previously reported case where physical activity was increased with the intervention. Proprioceptive neuromuscular facilitation and neuroplasticity principles espouse that for training to be effective, exercises should be frequent and intense to elicit synaptic changes.5,8 Increases in physical activity for patients with stroke lead to improved function and health.10
Time after stroke is also important when considering recovery. Time delays allow for greater establishment for self-taught compensatory strategies which affects rehabilitation.5 Case 3, who had the shortest duration of stroke episode appeared to have greater changes in motor outcomes. The remaining cases which had longer duration of stroke still improved in some motor outcomes to a lesser degree, and these changes were consistent with the previous case report which also had a more chronic presentation. Despite proposed time frames post-stroke where therapy is projected to be most-effective, changes in neural structuring are expected to work at any time.4 Although patients with stroke may experience a plateau in recovery, studies suggest that post-stroke rehabilitation that incorporates modifying a patient’s exercise regimen (e.g. intensity, new exercises) are important in motor rehabilitation.6 Stroke chronicity of the cases in this study varied greatly. Although earlier exposure to intensive and frequent therapy such as the intervention used in this study is beneficial, it is worth noting that all cases still benefitted to some extent.
The last factor was the individual differences of each plan of care. Although interventions were based on proprioceptive neuromuscular facilitation and neuroplasticity principles, plan of care was modified based on assessment and goals. It was important to practice what was most salient5 and what the patient was capable of.8 Furthermore, exercise intensity and progression were customized based on the responses. Exercises were removed if it was consistently difficult and were not progressed until they were performed in a coordinated manner, and with minimal fatigue. For example, cases 2 and 4 were given more preparatory mat activities as they had more difficulty with walking early in the intervention. Meanwhile case 3 tolerated the exercises better and progressed faster which might have contributed to her significant gains.
Overall, despite individual differences, each of the four new cases exhibited some gains in motor outcomes after the intervention, consistent with previous findings.6 Proprioceptive neuromuscular facilitation is both feasible and potentially beneficial for these types of patients. An important clinical implication of this study is that patients may still experience positive changes after proprioceptive neuromuscular facilitation despite chronicity of their stroke or their advanced age. A major consideration for the results were attributed to the exercises being designed consistent with principles of neuroplasticity.
In conclusion, this study showed that a proprioceptive neuromuscular facilitation program coupled with principles of neuroplasticity was safe and effective in improving the motor outcomes of four older adults with chronic stroke. Individual patient characteristics need to be considered when planning for intervention which may affect the amount of change seen during therapy. Although changes were seen despite chronicity and advanced age, it appears that patients with less chronic stroke, and with less co-morbidities may potentially benefit more from proprioceptive neuromuscular facilitation. Future studies are warranted to test these hypotheses in a larger sample.
Illustrations, Figures, Photographs
All figures or photographs should be submitted in a high resolution (minimum 300 DPI) electronic version saved in jpeg or tiff format. Original hard copies of all figures may be requested when necessary. Photographs will be accepted at the discretion of the Editorial Board. All lettering, arrows, or other artwork must be done by an artist or draftsman. If arrows are used please ensure they appear in a different color to the background color, preferably black with a white border, or white with a black border. If arrows distinguish different items on the figure then different arrow styles should be used ie. long, short, wide, narrow. Written informed consent for publication must accompany any photograph in which the subject can be identified. Written copyright permission, from the publishers, must accompany any illustration that has been previously published.
Acknowledgements
The authors acknowledge the contribution of the following individuals toward the completion of this study: Ms. Adjannie Ishtar Estuita, DPT and Mr. Frances Rom Lunar, MPT in independent assessment; Ms. Charlemaine Deane Perez, MPT in treatment implementation; and Ms. Alma Labro in project management.
Footnotes
Disclosure. This work was supported by the University of the Philippines Manila National Institutes of Health under the Student Researcher Grant 2014 (project number: NIH 2014-014).
- Received August 24, 2018.
- Accepted December 25, 2018.
- Copyright: © Neurosciences
Neurosciences is an Open Access journal and articles published are distributed under the terms of the Creative Commons Attribution-NonCommercial License (CC BY-NC). Readers may copy, distribute, and display the work for non-commercial purposes with the proper citation of the original work.
In this issue




{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.